Literature search results
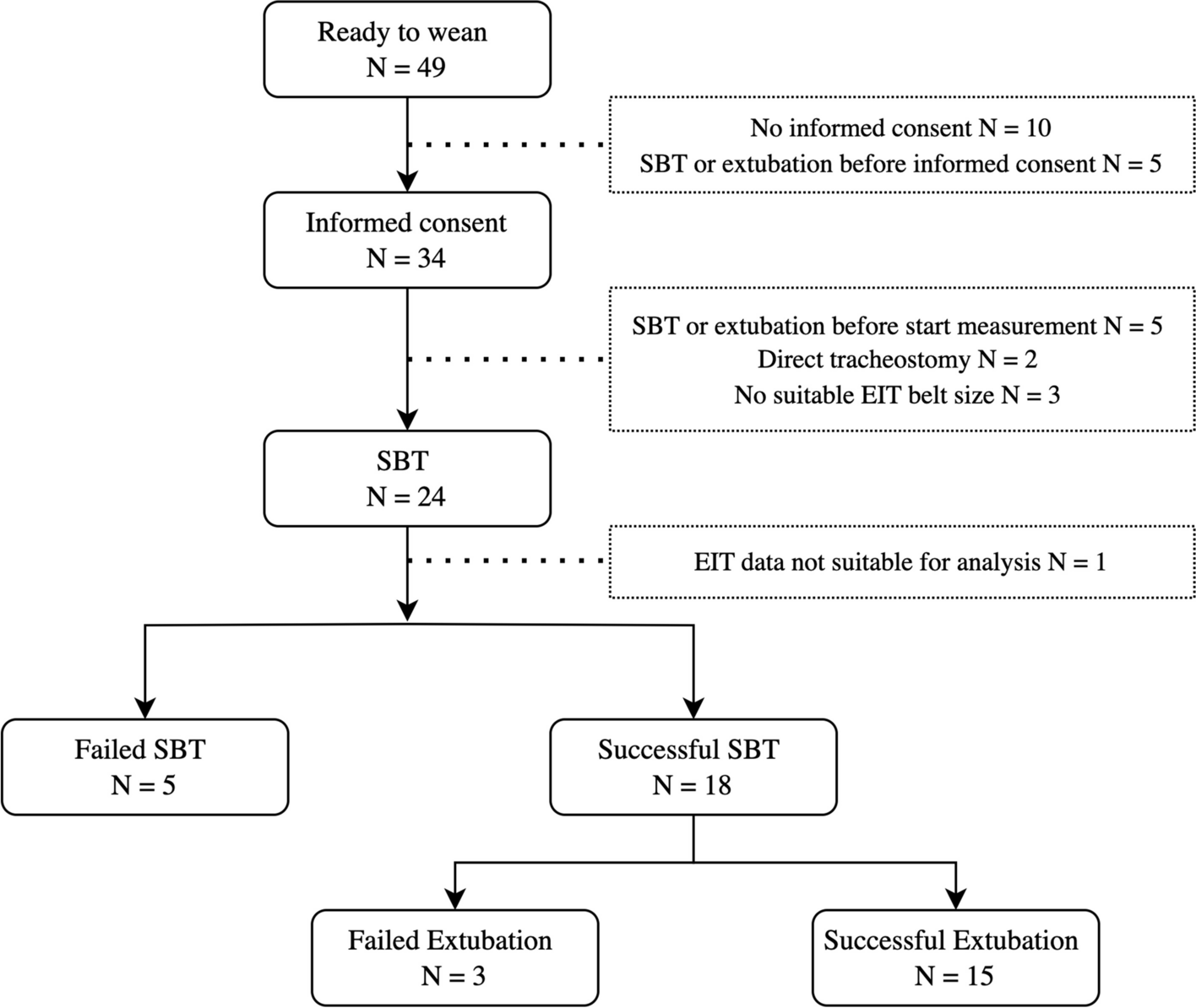
The initial search retrieved 933 results from MEDLINE, 473 from Pubmed, 453 from Embase and 7 from Cochrane Collection through June 30, 2023. In Fig. 1, the flow-chart with details on the included and excluded papers are shown. After removal of duplicates, 878 papers were uploaded into Mendeley. First-stage screening by reviewing titles and abstracts excluded 861 publications for not addressing both lung biopsy and SSc-ILD; 17 articles were identified as relevant and assessed for eligibility. After the second-stage screening, 4 articles were excluded because they were not pertinent to the research item. To capture other potentially relevant articles, we also evaluated the full list of references from Reviews, which lead to manual inclusion of 1 additional article which was found to be pertinent to the research item. Finally, 14 articles met all the inclusion criteria constituting the final pool of this SLR (Fig. 1).
Characteristics of the enrolled studies
Characteristics of the included studies are summarized in Table 1. The 14 studies selected in this systematic literature review included 364 SSc-ILD patients. The majority of studies (9/14) were retrospective single center studies. 11 studies based SSc diagnosis on ARA 1980 criteria, whereas two studies used the ACR 2013 diagnostic criteria [20, 21]. In 7 of the included studies, follow up data were available, with a mean duration of 5 years (+/- 4.44).
Table 1 Characteristics of the enrolled studiesPopulationClinical characteristics and lung function
Diffuse cutaneous SSc was variably present in the cohorts, ranging from 30 to 100% of cases. Female predominance was observed in all studies, ranging from 64 to 100%. Mean age in the studies ranged from 42 years to 64 years. Pulmonary function tests (PFTs) were available in all studies except one by Felicio et al. [22] Mean FVC was 73.98 (+/-17.3), mean DLCO was 59.49 (+/-16.1). PFTs value from Yamakawa et al. were not included in the analysis because of lack of separate data for patients with SSc [23].
Autoantibodies pattern
Only 3 studies had ANA data available showing ANA positivity in 96%, 73% and 100% of evaluated patients, respectively, [24,25,26]. Eight studies [19, 22, 23, 27,28,29,30] included data on anti-SCL70 antibodies positivity (median percentage 33%, range 0-69.6), 4 of them also evaluated ACA positivity (median percentage: 6.55%, min 3, max 32.5) [19, 23, 24, 27], and only 3 mentioned anti-RNP positivity (median percentage: 20%, min to (?), max 28) [23, 24, 27].
Previous or current treatments
In the included studies, previous treatment was poorly characterized. All patients in De Carvalho et al. study [31] (N = 18) and 20/25 patients from Xiao et al. [24], were naïve to treatment. The only previous treatments mentioned were corticosteroids (CCS, 5 patients) and cyclophosphamide (CYC, 3 patients). Five out of 14 studies provided information on ongoing treatment at the time of biopsy and the most common drugs used were CYC and CCS [18, 22, 26, 28, 29].
Lung biopsy techniques
Lung biopsies were obtained by surgery in 13 studies: VATS in 6) [18, 23, 25, 26, 28, 31, 32] and open surgical biopsy in 7) [22, 24, 28,29,30, 33, 34]. In one study, endobronchial biopsy was performed to study the bronchial mucosa [27]. None of the studies used transbronchial forceps biopsy or cryobiopsy for lung tissue sampling.
Few studies provided information on guidelines for surgical biopsy. The majority of studies highlighted the importance of avoiding CT honeycombing areas, e one study specified only that two or three biopsy specimens per patient were sampled [31] and in four studies, samples were taken in more than one lobe.28 33 26 None of the studies mentioned adverse events related to the biopsy procedure.
HRCT features
Radiologic findings are summarized in Table 2. CTs or HRCTs were performed in all studies, but in nine radiologic features were not reported. In the remaining five studies HRCT findings were available for 118 patients. NSIP features were reported in 89/118 (75.4%), and UIP in 14/118 (11.9%) patients. Only Yamakawa et al., reported PPFE in 4/72 (5%) cases; the same Authors reported 10/72 cases (13.8%) as unclassifiable ILD by HRCT [19, 22, 23, 26,27,28, 31, 34].
Table 2 SSc-ILD, radiologic and histopathologic features and correlationsHistopathologyMajor histopathology findings
Major histopathology findings are summarized in Table 2. In 12 studies, the histopathologic patterns are described, but 4 of them selected only NSIP cases. In the remaining 8 studies (261 LBx) the prevalence of NSIP, detected at the biopsy, was 70.9% (185/261 lung biopsies). The other histopathologic features were UIP in 21/152 cases (13.8%); end stage lung in 7/152 cases (4.6%), centrilobular fibrosis in 15/152 cases (9.8%), RB-ILD in 6/152 (3.9%), and pulmonary hypertension in 2/152 cases (1%) [18, 22,23,24, 26, 27, 30, 33, 34]. Only one study reported 11/32 biopsies as unclassifiable [23].
In 5 studies, NSIP was further classified into cellular or fibrotic (Table 2). Across all studies, fibrotic NSIP was the most prevalent feature in 63.4% (range 16–100%) of cases, while cellular NSIP was less frequently reported: 16.1% (range 0 to 58%).
The presence of CLF (interstitial fibrosis centered on membranous and respiratory bronchioles associated to foreign matter in the lumen due to microaspiration) was assessed in two studies only [28, 35]. Christmann et al. evidenced the presence of CLF in 5/ 21 patients, whereas the other 16 patients presented a NSIP pattern [28]. De Souza et al. showed that CLF was present as an isolated finding in 21% of patients, while some focal regions of this pattern were also found in 84% of patients with predominant NSIP [35].
Radiologic-pathologic correlations
The 4 studies reporting radiologic-pathologic correlations in 73 patients are summarized in Table 2.
Harrison et al. (year of publication 1991) showed that SSc patients without apparent CT changes can have pathologic findings on biopsy: 8 upper or middle lobe biopsies from regions defined as normal by CT were found to have not otherwise specified fibrosis histologically. In 21 cases, CT and histology were concordant in detecting ILDs and 3 normal lungs. In all 3 cases negative both at CT and histology electron microscopy could detect early changes [33].
Three studies (with a total of 46 cases) reported the correlation between HRCT and pathologic patterns: 41 cases showed a NSIP-HRCT pattern, and among them in 36 cases NSIP-HRCT was concordant with histopathology (88%, range 62-100%). Five NSIP-HRCT cases were histologically classified as UIP, (12%) [19, 26, 35]. All UIP-HRCT cases had honeycombing and were confirmed by as UIP on biopsy (4/27 total cases, 15%) [19, 26]. De Souza et al. reported one case of radiological UIP classified as NSIP by pathology [35].
De Souza evaluated HRCT features of patients with CLF and described that centrilobular or airway centered and patchy distribution of the lung involvement were features of CLF patients, while patients with histological NSIP showed peripheral and more diffuse distribution of ground-glass at HRCT: CLF was always associated with coexisting esophageal dilation (> 4 cm diameter) and with a higher frequency of centrilobular nodules (83%) [35].
Cellular findings on histopathology
Biopsy cellularity was examined in a few studies, either on bronchial mucosal biopsies or lung samples. In 23 patients, Sehlstedt et al. evaluated endobronchial biopsies and reported a higher number of neutrophils [27]. In lung biopsies, Harrison et al. evaluated neutrophils, eosinophils, macrophages, lymphocytes, and lymphoid aggregates in o the alveolar spaces and interstitium (determining inflammation): plasma cells were found in the interstitium and lymphoid aggregates and germinal centers were adjacent to bronchioles [33]. In lung biopsies, Yamakawa et al. found plasma cells infiltrate, lymphoid aggregates, germinal centers and fibroblastic foci, both in patients with SSc-ILD and ILD patients with SSc antibodies but without other clinical features of SSc [23].
Molecular findings on histopathology
In 4 studies, data on gene expression, cytokines and other molecular findings in lung or endobronchial biopsies were reported [27]. In mucosal endobronchial biopsies, Sehlstedt et al. found a lower epithelial IL-8 and NFkB expression in SSc-ILD samples compared to controls [27]. Christmann et al. compared gene expression of macrophage markers, chemokines, collagen, as well as transforming growth factor β– and interferon (IFN)–regulated genes, in lung biopsies of SSc-NSIP and controls. They found that expression of these genes correlated with progressive lung fibrosis defined by progression in radiological score (FibMax). Immunohistochemistry confirmed increased markers of collagen (COL1A1), IFN (OAS1 and IFI44), and macrophages (CCL18 and CD163). Moreover, several genes correlated with both the change in FibMax and the change in % predicted forced vital capacity, including IFN and macrophage markers, chemokines, and heat-shock proteins [28]. Parra et al. evaluated different expression of proteins regulating NO synthesis, and found that higher levels of iNOS, IL-13 and bFGF expression in lung biopsies of SSc patients with cellular and fibrotic NSIP correlated with the amount of parenchymal fibrosis [30]. More recently Xiao et al. evaluated 25 lung biopsies in SSc-ILD and found that the hedgehog pathway activation was increased in the lung tissue of SSc-ILD patients and this was decreased by pirfenidone, Sufu (suppressor of fused) was upregulated in lung fibroblasts after pirfenidone challenge, and pirfenidone inhibited the phosphorylation of GSK-3b signalling [24].
Prognostic significance of histopathology featuresMortality
Among the 14 selected studies, only 4 studies reported SSc-ILD mortality data [18, 19, 23, 29], and only 2 reported the histopathology correlation with survival [18, 19]. Major findings are summarized in Table 3.
Table 3 Prognostic significance of histopathology findings in SSc-ILDCompared to UIP, NSIP showed better survival rates, but only in the Fisher et al. study did this reach statistical significance (median survival in years 15.3 for NSIP compared to 3 for UIP, p = 0.007) [18, 19]. Pooling the 5 years mortality from the two studies, the difference between histopathologic UIP-SSc and NSIP-SSc didn’t reach statistical significance: overall mortality for UIP-SSc was 37.5% (6/16) compared to 13.8% (9/65), p = 0.06 [18, 19]. Bouros et al. reported no difference in survival for UIP vs. NSIP nor for PFTs trends between fibrotic and cellular NSIP (15 and 47 total cases respectively) [18]. Baseline FVC and DLco, higher BAL eosinophils, DLco deterioration at 3 years and honeycombing at CT significantly correlated with mortality of SSc-ILD [18, 23].
Two prognostic studies compared CTD-ILD to idiopathic NSIP (iNSIP) and there was no mortality difference [22, 31]. Felicio et al. compared 20 iNSIP to 21 CTD-NSIP (10 were SSc-NSIP) confirming the overall good prognosis of NSIP in both groups (overall survival 135 months for iNSIP and 227 months for CTD-NSIP) [22]. De Carvalho et al. compared 22 iNSIP to 18 SSc-NSIP (all fibrotic) finding a higher collagen and elastic fibers content in the SSc-NSIP group, but without prognostic differences on univariate Kaplan Meyer analysis [31].
Disease progression
In 3 studies the functional decline of SSc-ILD was evaluated (Table 3) [18, 26, 35]. Only Kim et al. compared the functional decline between NSIP and UIP, reporting a better outcome after immunosuppressive treatment for NSIP compared to UIP (15% FVC improvement in 5/12 NSIP cases treated with CCS and CYC, compared to no improvement in the 5 UIP patients and a decrease in the CRP score after treatment only in the NSIP group) [26]. Only De Souza compared functional decline between NSIP and CLE without finding any statistically significant difference [35].









留言 (0)