Lumbar interbody fusion (LIF) is a well-established surgical technique for treating degenerative spinal diseases [10], with advantages in stabilizing painful segments, restoring lumbar lordosis, correcting spinal deformities, and decompressing nerves [11]. However, conventional open lumbar fusion surgery has always been associated with greater tissue damage, more blood loss, and slower postoperative recovery [12], which is detrimental to the patient. To minimize surgical trauma and postoperative complications, spine surgeons are committed to combining minimally invasive concepts with endoscopic techniques. The emergence of spinal endoscopy has enabled spinal surgery to make the leap from open to minimally invasive surgery. Studies have shown that spinal endoscopic lumbar fusion can obtain favorable results in the treatment of degenerative spinal diseases [13]. However endoscopic lumbar interbody fusion (Endo-LIF) is still associated with several limitations. Firstly, the surgical field of Endo-LIF is relatively limited. Because of the limitation of the operating trocar, it is difficult to tilt the instruments, and it is often necessary to tilt the operation table to observe the contralateral lateral recess. These processes will cause unnecessary trouble to the operator, resulting in prolonged operation time [14]. Secondly, because of the limitations of the operation tubular size, it is not possible to place larger cages, which may affect the intervertebral fusion [15]. The UBE technique allows the establishment of portals through the skin without the limitation of operating a trocar, meanwhile, ULIF can place a larger cage and adjust the cage angle more conveniently, which may be the reason why ULIF has better fusion rate [16]. Previous studies have shown that ULIF presents the advantages of less trauma, less bleeding, faster postoperative recovery, and favorable fusion rate [5]. A meta-analysis by Yu et al. [17] indicated that compared to conventional TLIF, ULIF has the advantages in relieving postoperative pain, shortening hospital stay, and enhancing functional recovery. Liu et al. [12] performed a prospective cohort study and found that ULIF has the advantages of minimizing surgical trauma and reducing inflammatory reaction compared to posterior lumbar interbody fusion (PLIF). Our study also found that ULIF showed favorable results in alleviating postoperative pain and improving functional recovery.
The learning curve reflects the speed of mastering skills over a certain time. For beginners, it is usually the number of cases required to reach relative stability in surgical technique [18]. The learning phase of ULIF also requires a lot of clinical experience and a lot of practice. Different from unilateral biportal lumbar discectomy (UBLD), ULIF requires endoscopy insertion into the vertebral body space for endplate preparation and needs to place the cage and adjust the orientation under indirect visualization during operation, which is not exactly similar to open lumbar fusion surgery. Even for spine surgeons with UBE experience, there are still challenges in the early learning phase of ULIF. Chen [19] found that for spine surgeons with no arthroscopic experience, operative time gradually steadied after completing 24 cases of UBLD, suggesting that the surgeons were able to achieve a more proficient and stable performance level. Xu [20] found the significant reduction in operation time for spine surgeons after completing 54 cases of UBLD. After completing 89 cases, the success rate of the procedure began to be stable, suggesting that experience was still required to achieve a higher success rate after overcoming the learning curve. Kim [21] considered that at least 34 cases were needed to master the ULIF. Although the definition of the learning curve is influenced by a variety of subjective factors, surgeon experience, team coordination, surgical instrumentation differences, and differences in operating room procedures may all influence the definition of the learning curve. We can conclude objective and replicable experiences to provide technical references and reduce unnecessary learning time and costs [18].
CUSUM was first described by E.S. Page in 1954 and was initially used as monitor performance in the manufacturing industry. Since then, it has been implemented to assess technical training in a variety of procedures [22]. CUSUM analysis is an excellent statistical metric to quantitatively assess the learning curve, while the CUSUM chart is a precise representation of the temporal relationship between the chronological number of cases performed and a surgeon's ability in a specific surgical task [23]. In this study, the CUSUM analysis for the operation time showed that the operation time started to plateau gradually when surgical cases reached 29 cases, operation time in the mastery phase was approximately 40 min shorter than those in the learning phase (133.55 ± 22.76 mins vs. 175.38 ± 34.23 mins). However, operation time cannot be used as the only indicator for evaluating the learning curve, and simply selecting operation time as the definition of the learning curve may lead to bias [24]. It is not only the proficiency of the surgeons that determines the learning curve but also the safety and health interests of the patients. Therefore, we further verify the learning curve of ULIF through RA-CUSUM analysis [25]. RA-CUSUM takes the surgical failure rate as a parameter. We defined all complications that occurred after ULIF as the occurrence of surgical failure and thus constructed a learning curve based on the surgical failure rate. In this study, the RA-CUSUM analysis showed that the success rate of surgery began to stabilize gradually when the surgical cases reached 41 cases. The complication rate was significantly lower in the mastery phase (17.07%) than in the learning phase (2.6%) (P < 0.05). Notably, the CUSUM analysis-based learning curves showed similar results between the two stages of complication rates. In our study, spine surgeons had some experience with UBLD (no less than 150 cases). Therefore, even at the early stage of the ULIF learning phase, there are more advantages in the coordination of two hands and the stabilization of one hand compared to surgeons without UBE experience. This probably explained why even when faced with the more challenging ULIF in our study, the surgeons still had fewer cases to overcome the learning curve than with the UBLD. In our center, spine surgeons are required to undergo standardized training as well as practice on models and solids before they can perform UBE, and to accumulate experience with at least 90 cases of UBLD before they can perform ULIF, which is a natural learning process [20]. ULIF is based on UBE and traditional open surgery, and performing ULIF without UBE experience is very difficult and may cause a negative impact on the safety of the patients as well as surgical outcomes. There are some suggestions on how to shorten the learning curve. We recommend that beginners should choose easier cases in the early stages, while the right-sided approach may be more comfortable for right-handed people to minimize the difficulty of the practices and overcome the curve of UBLD before proceeding to ULIF. In the early stages, the application of the 0° endoscope allows beginners to adapt more quickly to the UBE technique. Additionally, the spinal canal should be completely explored before the end of the procedure, and the viewing portal and the working portal can be exchanged if necessary to expand the exploration range.
Cage subsidence were observed in two cases (1.08%) in this study, both of which occurred during the learning phase, suggesting that protecting the endplates in the early stage of ULIF was a challenge for spine surgeons. In theory, endplate preparation is the key to lumbar fusion. Damage to the endplate or a reduction in the contact area between the endplate and the cage are possible factors for cage subsidence [26]. Endplate preparation requires the insertion of endoscopy into the intervertebral space and removing the intervertebral discs using curette and disc reamers, which can easily cause bony endplate injuries when the instruments are inserted and removed, especially in patients with narrow intervertebral spaces. Additionally, there is a blind spot between the skin and the endoscope at cage placement, which may also be a factor in endplate injury. For beginners, several points should be considered when preparing endplates. While using endplate curettes to remove cartilaginous endplates, the changes in the endplate should be continually monitored with the endoscope, and the evidence of successful endplate preparation is multiple spots of bleeding from the bone. For the right-handed person, instrumentation in and out of the intervertebral space is best done through the right side of the patient, especially on the level L4/5 or L5/S1, because the working portal is located on the rostral side and on these levels the intervertebral space is tilted caudally. Our study found that BMI was a risk factor for surgical failure, which is similar to previous study [27]. Patients with greater BMI are subjected to greater axial stresses on the cage, which may lead to cage subsidence; therefore, in patients with greater BMI, the length of weight-bearing should be appropriately prolonged with close follow-up.
Dural tears were observed in three cases (1.63%), all of which occurred in the lumbar spinal stenosis. Due to the close attachment between the ligamentum flavum and the dural sac, the dural tears occurred when the ligamentum flavum was violently peeled off using the Kerrison rongeur. Since the tear was small, we used gelatin sponges for compression while maintaining lumbar drainage postoperatively [28]. Distributed in the midline or near the midline surface of the dural sac are meningovertebral ligaments varying in thickness and shape from thin strips to thick sheets, which are capable of connecting the dorsal side of the dural sac with the lamina and ligamentum flavum [29]. Insufficient dissection of this structure may be the primary mechanism of the dural tears. We recommend removing the thin strips between the ligamentum flavum and the dural sac with the bent probe and confirming the detachment before biting off the ligamentum flavum. Furthermore, laminectomy that is wide enough to expose the cephalic and caudal edges of the ligamentum flavum, and removal of the ligamentum flavum en bloc, will also help to minimize injury.
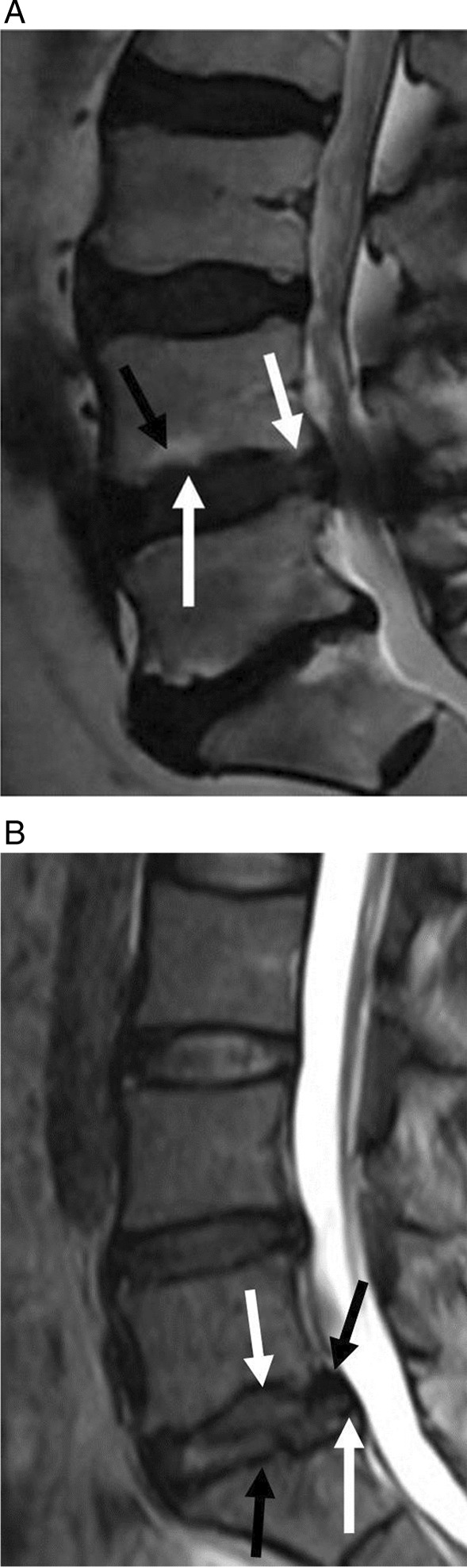
Epidural hematoma were observed in two cases (1.08%), however, the two cases did not have any symptoms, which was called asymptomatic epidural hematoma. In patients undergoing lumbar spine surgery without drainage, MRI can detect up to 89% of asymptomatic epidural hematoma [30], whereas the incidence of symptomatic epidural hematomas is less than 1% [31, 32]. Although most cases with epidural hematoma are not accompanied by any clinical symptoms, we still recommend aggressive MRI for early exclusion of symptomatic epidural hematoma in patients presenting with symptoms of postoperative nerve injury. Our study found that hypertension was the risk factor for surgical failure. In patients with suboptimal vascular conditions, blood pressure elevation will be more significant at the end of anesthesia, which will lead to unpredictable bleeding [33], and even epidural hematoma. Studies have shown that [34, 35] using drainage after lumbar surgery significantly reduced the incidence of postoperative asymptomatic epidural hematoma, and we similarly suggest that drainage should be used after ULIF regardless of the bleeding volume. Notably, surgical bleeding may lead to the occurrence of epidural hematoma [31]. The depth of the anesthesia of the patients may influence the pressure of the spinal canal and the blood loss [36], thus from the beginning of the procedure the physician should monitor the anesthesia and provide appropriate control of the depth of the anesthesia. Continuous intraoperative saline irrigation has advantages in controlling bleeding. Keeping the saline level 50–60 cm above the plane of the surgical incision and maintaining the water pressure at 25–30 mmHg can keep a clear surgical field while controlling bleeding better.
There are still some limitations in our study. First, this was a retrospective study, and all surgeries were performed by the same spine surgeon, which is potentially biased. Therefore our experience is not applicable to other spine surgeons. Due to a variety of practical factors, other spine surgeons may overcome the learning curve earlier or later than we did in our case. Second, the spine surgeon in this study had prior experience performing the UBE technique. Considering that all spine surgeons at our center are required to perform UBLD before ULIF, we do not have sufficient data to further analyze the learning curve of ULIF for surgeons lacking UBE experience. Future large-sample, multicenter, prospective studies are still needed for further verification.


留言 (0)