
記住我

This study adhered to the CONSORT guidelines. This randomized controlled study involved 102 patients with spinal metastases treated at three affiliated hospitals of Zunyi Medical University from December 2017 to June 2022. Patients were randomly assigned to two groups using a random number table : 52 patients in in the treatment group involving the combined NOMS decision system-utilizing multidisciplinary team and Revised Tokuhashi scoring system (i.e., the combined group)and 50 patients in the treatment group involving the Revised Tokuhashi scoring system only (i.e., the revised TSS-only group). The study was approved by the Ethics Committee of the affiliated hospitals of Zunyi Medical University. All patients signed an informed consent form and voluntarily participated in the study.
Inclusion/exclusion criteria for patients were as follows: (1) ≥ 18 years of age; (2) definite diagnosis of spinal metastases and willingness to undergo selected surgical treatment; (3) clear primary tumour, including lung cancer, breast cancer, prostate cancer, or kidney cancer; (4) follow-up duration after surgery ≥ 1 year with complete follow-up data; (5) expected survival period ≥ 6 months; (6) good general condition to tolerate surgery; (7) treated by experienced spine surgeons; and (8) having the surgical indications: (a) presence of spinal instability—Spinal Instability Neoplastic Score (SINS) ≥ 7 points, (b) presence of progressive neurological compression symptoms—epidural spinal cord compression (ESCC) grade ≥ 2, and (c) presence of refractory and intractable pain. The exclusion criteria for patients were as follows: (1) primary spinal tumours; (2) complications such as vertebral fractures and severe intervertebral disc herniation caused by factors other than metastatic tumours which may affect postoperative evaluation; (3) lack of complete medical history and/or loss to follow-up after treatment; (4) life expectancy < 6 months and responsive to narcotic analgesics or markedly responsive to radiotherapy; poor general condition (Karnofsky Performance Status 3 or poorer); or reduced will to live.
Preoperative clinical data in the two groupsAll patients underwent comprehensive preoperative examinations. The collected data included name, sex, age, type of primary tumouor, metastasis location, SINS (0–18 points, with 0–6 indicating spinal stability, 7–12 indicating potential instability, and 13–18 indicating instability; a score ≥ 7 points indicated surgical treatment), ESCC grade ( grade 0: tumouor confined to bone; grade 1: tumouor extends to extradural space without deforming the spinal cord; grade 2: spinal cord compression but cerebrospinal fluid visible; grade 3: spinal cord compression with no visible cerebrospinal fluid), preoperative VAS score (0–10 points, with higher scores indicating more severe pain), Eastern Cooperative Oncology Group (ECOG) performance status (0–5 grades, with higher grades indicating worse physical condition; level 0, normal activity capacity, no difference compared to preonset activity level; level 1, able to freely move and engage in light physical activities, including general household chores or office work, but unable to perform heavy physical activities; level 2, ability to freely move and perform activities of daily living but with lost work capacity; can be out of bed and active for at least half of the day; level 3, partially able to perform activities of daily living, spending more than half of the day in bed or wheelchair; level 4, bedridden, unable to perform activities of daily living independently; level 5, death), overall condition Karnofsky Performance Scale (KPS) score (0-100%, divided into ten grades, with higher scores indicating better physical condition), and negative psychological assessment score (using the self-rating anxiety scale (SAS), anxiety levels can be classified into four categories: normal, mild, moderate, and severe anxiety; normal, SAS score < 50; mild, SAS score between 50 and 59; moderate, SAS score between 60 and 69; severe, SAS score ≥ 70), neurological function status,Frankel classification, divided into A, B, C, D and E; 5 grades, with A, complete paralysis; B, incomplete loss of sensory function, no motor function; C, incomplete loss of sensory function, nonfunctional movement; D, incomplete loss of sensory function, functional movement; and E, normal sensory and motor function).
Study methodsMultidisciplinary team using NOMS and revised Tokuhashi scoring system group(1) Establish the multidisciplinary team: Led by orthopaedic surgeons, the team includes general surgery, oncology, radiology, pathology, pain management, nuclear medicine, endocrinology, rehabilitation, psychosomatic medicine, and anaesthesiology staff. Personnel from each specialty play a specific role, with orthopaedic surgeons overseeing and implementing the entire treatment plan, including surgical procedures. (2) Preoperative assessment and adjustment by the MDT: Upon admission, the team evaluated and adjusted the patient’s preoperative condition (correcting hypoproteinaemia, adjusting blood pressure, controlling blood sugar, regulating blood clotting function, and providing psychological support to enhance self-confidence) based on various indices such as primary tumouor, preoperative examination results, SINS, ESCC grade, VAS score, ECOG physical condition, KPS score, SAS score, and Frankel classification. The team collaboratively formulated the preoperative treatment plan and prepared the patient for surgery. (3) Surgical plan formulated and executed by the MDT: Based on the aforementioned indices, the MDT thoroughly discussed and strictly followed the NOMS decision system and the Revised Tokuhashi scoring system to assess each patient and develop a comprehensive surgical plan, choosing between excisional surgery and postoperative traditional external beam radiotherapy (cEBRT) or stereotactic radiosurgery (SRS), depending on the radiation sensitivity, ESCC grade, SINS, and the Revised Tokuhashi score. (a) For patients with ESCC grade ≥ 2, SINS ≥ 7 points, Revised Tokuhashi score ≥ 12 points, and a general condition tolerant of surgery, if radiotherapy-sensitive, en-bloc resection surgery and postoperative conventional external beam radiation therapy (cEBRT), if radiotherapy-insensitive, en-bloc resection surgery and postoperative stereotactic radiosurgery (SRS) are selected; (b) For patients with ESCC grade ≥ 2, SINS ≥ 7, Revised Tokuhashi score of 9–11, and systemic conditions who are surgery-tolerant, palliative surgery and postoperative traditional external beam radiation therapy (cEBRT) if radiotherapy-sensitive, and palliative surgery and postoperative stereotactic radiosurgery (SRS) if radiotherapy-insensitive; (c) For patients with ESCC grade < 2, SINS ≥ 7 points, Revised Tokuhashi score ≥ 12 points, and systemic conditions that tolerate surgery, if radiotherapy-sensitive, en-bloc resection surgery and postoperative conventional external beam radiation therapy (cEBRT) are selected, if radiotherapy-insensitive, en-bloc resection surgery and postoperative stereotactic radiosurgery (SRS) are selected; (d) For patients with ESCC grade < 2, SINS score of ≥ 7, Revised Tokuhashi score of 9–11, and systemic surgery-tolerant, if radiotherapy-sensitive, palliative surgery and postoperative conventional external beam radiation therapy (cEBRT) are selected, if radiotherapy-insensitive, palliative surgery and postoperative stereotactic radiosurgery (SRS) are selected.) (4) Multidisciplinary collaboration in surgery execution. (5) Postoperative care by the MDT: Infection prevention, psychological therapy, pain management, dietary and nutritional therapy, rehabilitation and functional training, and further treatment of the primary tumouor (radiotherapy, chemotherapy, and targeted therapy). (6) Discharge planning by the MDT: includes detailed plans for radiotherapy, chemotherapy, psychological therapy, rehabilitation training, and regular follow-up scheduling. (Fig. 1; Tables 1 and 2).
Table 1 Revised Tokuhashi prognostic scoreTable 2 Treatment selection table for NOMS combined with revised Tokuhashi scoring systemSolely treated according to the revised Tokuhashi scoring system group (1) Orthopaedic surgeons independently adjusted the preoperative conditionBased on various indices such as the primary tumouor, preoperative examination results, SINS score, ESCC grade, VAS score, ECOG physical condition, KPS score, SAS score, and Frankel classification, orthopaedic surgeons developed the preoperative treatment plan and adjust the patient’s condition, with oncological consultations for primary and metastatic lesions and anaesthesia evaluation one day before surgery. There was no involvement of pain management, psychosomatic medicine, radiology, or rehabilitation departments. (2) Orthopaedic surgeons independently formulated and executed the surgical plan. Strictly following the Revised Tokuhashi scoring system for patient assessment, surgeons chose between excisional and palliative surgery based on the Revised Tokuhashi score. (3) Postoperative management by orthopaedic surgeons included fluid replacement, anti-infection measures, empirical pain control, and rehabilitation exercises, with consultations from relevant departments as necessary. (4) Poststabilization, regular radiotherapy and chemotherapy plans were developed for tumouor treatment.
Fig. 1
Schematic depiction of the neurologic, oncologic, mechanical, and systemic (NOMS) decision framework [9]
Observed indicesPatients are regularly followed up in the outpatient clinic at 1, 3, 6, and 12 months after surgery. The two groups of patients with the same primary type of tumours were given the same type of chemoradiotherapy.
Intraoperative, postoperative, and follow-up observation indices includedintraoperative or postoperative complications, average postoperative hospital stay (days), and mortality rate.
Long-term postoperative follow-up assessments at 1, 3, 6, and 12 months included the following:(1)VAS score: The patient’s postoperative pain status was evaluated (0–10 points, with higher scores indicating more severe pain). (2) ECOG Performance Status: The recovery of the patient’s physical condition after tumouor surgery was assessed (0–5 grades, with higher grades indicating worse physical condition). (3) Karnofsky Performance Scale (KPS%) score: This score was used to assess the patient’s e ability to perform daily activities postoperatively and quality of life (0-100%, divided into ten grades, with higher scores indicating better physical condition). (4) Self-rating anxiety scale (SAS) score: The SAS was used to evaluate the patient’s postoperative psychological state (divided into normal, mild, moderate, and severe). (5) Neurological Function Status (Frankel Classification): Graded as A, B, C, D and E (A: Complete paralysis; B: Incomplete loss of sensory function, no motor function; C: Incomplete loss of sensory function, nonfunctional movement; D: Incomplete loss of sensory function, functional movement; E: Normal sensory and motor function).
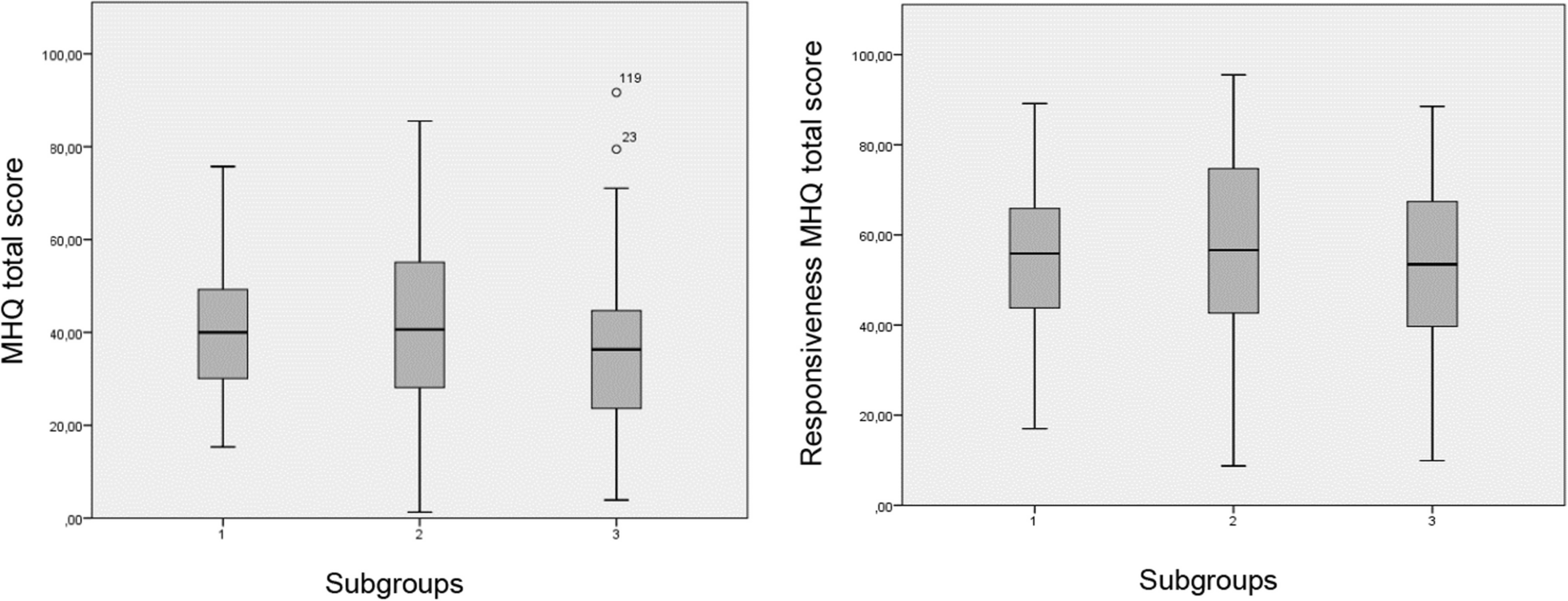
Statistical methodsWe used SPSS 25.0 (IBM Corp, Armonk, NY, USA) software for statistical analysis. Continuous data were presented as mean ± standard deviation (x ̅±s). Independent sample t-test or Mann-Whitney U-test was performed for quantitative data such as age, VAS score, KPS score, SINS score. Chi-square test, Fisher’s exact test, or rank-sum test were used for categorical data such as ECOG performance status, Frankel grade, SAS score categories, gender. P < 0.05 was considered to indicate statistical significance (See Fig. 2).
Fig. 2
留言 (0)