Maxillofacial fractures constitute one of the most frequent pathologies treated at Maxillo-Facial Units. They represent an important public health and economic problem. The epidemiology is variable and dependent on socioeconomics factors, geographical area and cultural and racial differences [1]. The most common causes of facial fractures include assaults, falls, traffic accidents, sports accidents and work accidents [9].
National Healthcare Expenditure Accounts data in 2019 show that Italy spends about 118 billion euros per year on health care with the cost of maxillofacial injuries calculated to be approximately 160 million euros.
The incidence of maxillofacial fractures varies widely among different countries, and a large number of studies [10,11,12] have been performed regarding their epidemiology. The epidemiological analysis of maxillofacial fractures is essential to identify these injuries and to better address preventive measures and healthcare expenditure resources.
A common finding in many studies is that male patients are more frequently affected by maxillofacial bone trauma than female patients [13] probably due to a higher rate of mobility, an intense social interaction with a higher probability of being involved in criminal or violent situations and a greater inclination to participate in dangerous or extreme sports. This is consistent with our results; in our group, the majority of the patients included were males. In our experience, men were more frequently involved in interpersonal violence, whereas women in domestic accidents. In the literature, interpersonal violence has often been reported in patients living in socially disadvantaged conditions in the urban centers of developed countries [1, 14]. Therefore, the most common cause of facial trauma in males is road traffic accidents followed by assaults, falls, sports-related accidents and work-related accidents. The most frequent cause of facial injuries in females is road traffic accidents follow by accidental falls, assaults, work-related accidents and sport-related accidents.
As previously mentioned, our cohort reported a different epidemiology. This might be due to the peculiarity of the reference period. In fact, we report a greater frequency of traumas resulting from interpersonal violence as compared to road traffic collisions. The peculiarity of the period considered in the study, indeed, consists not only in the closure of commercial and recreational activities but also in the introduction of measures such as smart working.
As described in the literature [8], facial fractures, generally, tend to be mandibular fractures with a condylar involvement, whereas in interpersonal violence accidents, the zygomatic complex, orbit and nose are the most common bones involved. In this study, we have classified the fractures in terms of high and low impact. In agreement with the previously mentioned literature findings, in our cohort we found that the interpersonal violence injuries were predominantly nasal and zygomatic fractures (low impact fractures). In contrast to the scientific literature, we detected a lower frequency of high impact fractures (96 low impact and 59 high impact), a finding which might also be a result of the introduction of the lockdown restrictions.
The analysis of maxillofacial traumatic injuries revealed a predominance of young adult, male patients with the injuries most commonly caused by motor vehicle accidents. Our findings disagree with those presented in the literature in this case. Indeed, we report a median age at admittance for interpersonal violence of 26 years of age and for traffic road collisions of 36 years of age.
The severe acute respiratory syndrome SARS-CoV-2 was first recorded in China at the end of December 2019 and then spread like wildfire worldwide. Within a few weeks, it had had an immense impact on the population, community and individual behaviors and habits.
Since the start of the COVID-19 pandemic, maxillofacial elective surgery was gradually reduced nationwide and clinical work scaled down in order to keep services running without putting both the healthcare workers and patients at risk. As already shown elsewhere in the literature, national holidays, seasonal trends and natural disasters like the pandemic emergency influence the incidence of trauma [15].
The pandemic and the related restriction measures are linked to increases in depression and anxiety, isolation and loneliness, alcohol and cannabis misuse and unemployment and other economic problems [4, 16]. This may be the reason why in our analysis we have observed a prevalence of facial injuries mainly due to assaults and domestic accidents. In our cohort, we have also identified three cases of suicide attempts, two of which happened during the restriction period. Many experts have voiced concerns that mental, economic, behavioral and psychosocial problems linked to the COVID-19 pandemic might have contributed to a rise in suicidal behaviors [16].
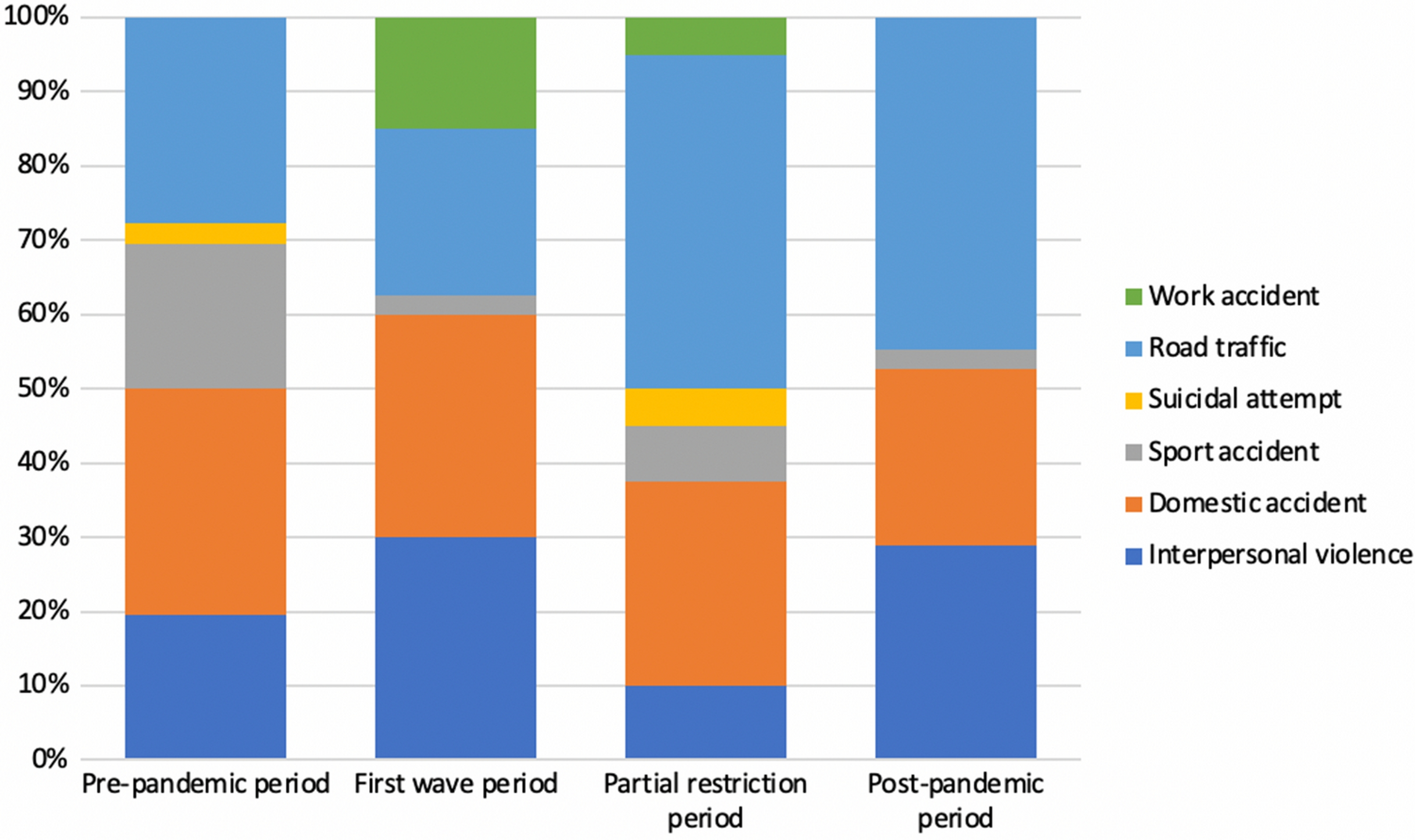
Our statistical analysis has also highlighted that when the restrictions were stricter (the first wave period) an actual shift in the causes of admission for trauma was observed. We compared the pre-pandemic group causes of admission versus each single period afterward. Only the comparison with the first wave demonstrated a significant statistical difference (p = 0.002). This finding is confirmed by the further analysis performed by means of the Fisher’s exact test on the first wave group versus the restriction and post-pandemic groups. Furthermore, when looking at the descriptive analysis, it is striking that the admissions for traffic collisions were more frequent during the pre-pandemic (27.8%), partial restrictions (45%) and post-pandemic (44.7%) periods. In contrast, the majority of the patients admitted during the first wave lockdown were victims of interpersonal violence (30%) and domestic accidents (30%). In fact, during the first wave lockdown the rate of admissions for road traffic accidents was the lowest of all the four phases (22.5%), due to the introduction of government measures such as smart working and traveling admitted only for emergency reasons.
During the partial restrictions and post-pandemic periods, the rates for interpersonal violence and domestic accidents were 10, 28.9, 27.5 and 23.7%, respectively. These findings demonstrate that these rates were lower when the restrictions were loosened. This is probably a consequence of the fact that during the lockdown the forced house sharing and forced confinement at home may have generated a rise in aggression and an increase in domestic trauma.
It is interesting to note that, contrary to what might have been expected, the prevalence of maxillofacial traumas has not decreased during the lockdown period. This observation has already been reported in the literature by other authors who have not found significant differences in terms of the prevalence [2] and severity [4] of facial traumas during lockdown periods. This is due to a shift in the etiology of fractures, with a reduction in traumas due to road accidents and an increase in those related to other causes, such as interpersonal violence, domestic incidents and accidental falls.
The principal strength and novelty of this study lie in its pioneering analysis of the trends in the epidemiology of facial fractures throughout the various phases of the pandemic, extending into the post-pandemic period. This comprehensive approach allows for an assessment of whether the pandemic has had stable effects on people's habits sufficient to permanently alter the epidemiology of fractures. Understanding these changes is crucial, as it can inform future public health strategies and healthcare resource allocation. By identifying shifts in the causes and patterns of facial fractures, healthcare systems can better prepare for and respond to similar global health crises in the future, potentially leading to improved patient outcomes and more efficient use of medical resources.
However, the study is not without its limitations. Its retrospective nature is one such constraint, which may introduce biases related to data collection and analysis, limiting the ability to control for all potential confounding variables or to capture the full spectrum of relevant data. Additionally, being a single-center study poses challenges to the generalizability of the results. The data and conclusions drawn from one hospital or region may not accurately reflect the situation across the entirety of Italy, as regional variations in healthcare systems, population behaviors and pandemic impact can significantly influence the epidemiology of facial fractures.










留言 (0)