
記住我

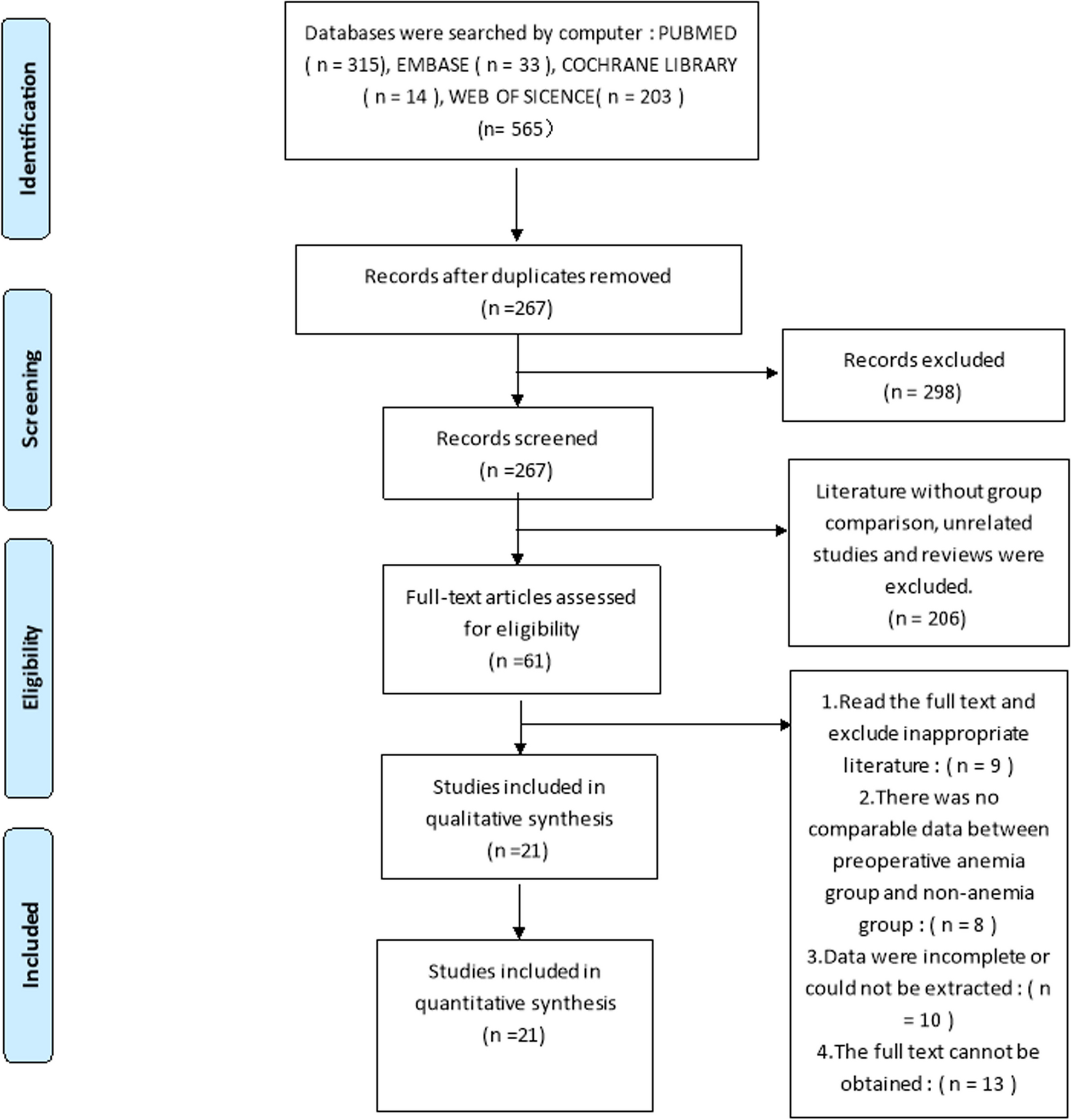
In this study, a total of 150 elderly patients with pelvic fragility fractures were included in the evaluation, of which 19 were not eligible for inclusion, and 13 refused to participate. The 118 eligible patients were divided into two groups by random number table, namely the observation group (Observation) and the control group (Control). Artificial intelligence (Tianji Orthopedic Robot) was used to implant the anterior and posterior ring fracture cannulated screws for fixation. After the screw channel was established, the observation group was implanted with bone cement (#CLVP, Dezhou Jianjie Medical Equipment Co., LTD, Dezhou, China) using the spinal vertebral body forming sleeve system, and immediately implanted the hollow screw to complete the bone cement reinforcement. The control group underwent conventional treatment, which involved the implantation of cannulated screws to stabilize the fractured end of the pelvis. All patients were followed up for 1 year after treatment, during which 4 patients died and 4 lost contacts in the control group; 3 patients died and 6 lost contacts in the experimental group. Finally, 50 cases in the Observation group and 51 cases in the Control group was collected with complete follow-up data (Fig. 1). All participants have signed informed consent, and the study was approved by Cangzhou Hospital of Integrated Traditional Chinese Medicine and Western Medicine. The study was performed in strict accordance with the Declaration of Helsinki, Ethical Principles for Medical Research Involving Human Subjects.
Fig. 1
Research framework of this trail
Inclusion Criteria:
(1)Participants aged 60 years or older.
(2)Pelvic fractures resulting from low-energy injuries, such as falls from a standing position.
Exclusion Criteria:
(1)Patients younger than 60 years with high-energy trauma.
(2)Pelvic fractures caused by pathological conditions, including metastatic tumors, hormone-related fractures, and open fractures.
(3)Participants with incomplete clinical or follow-up data.
(4)Fractures located in other regions of the lower limbs.
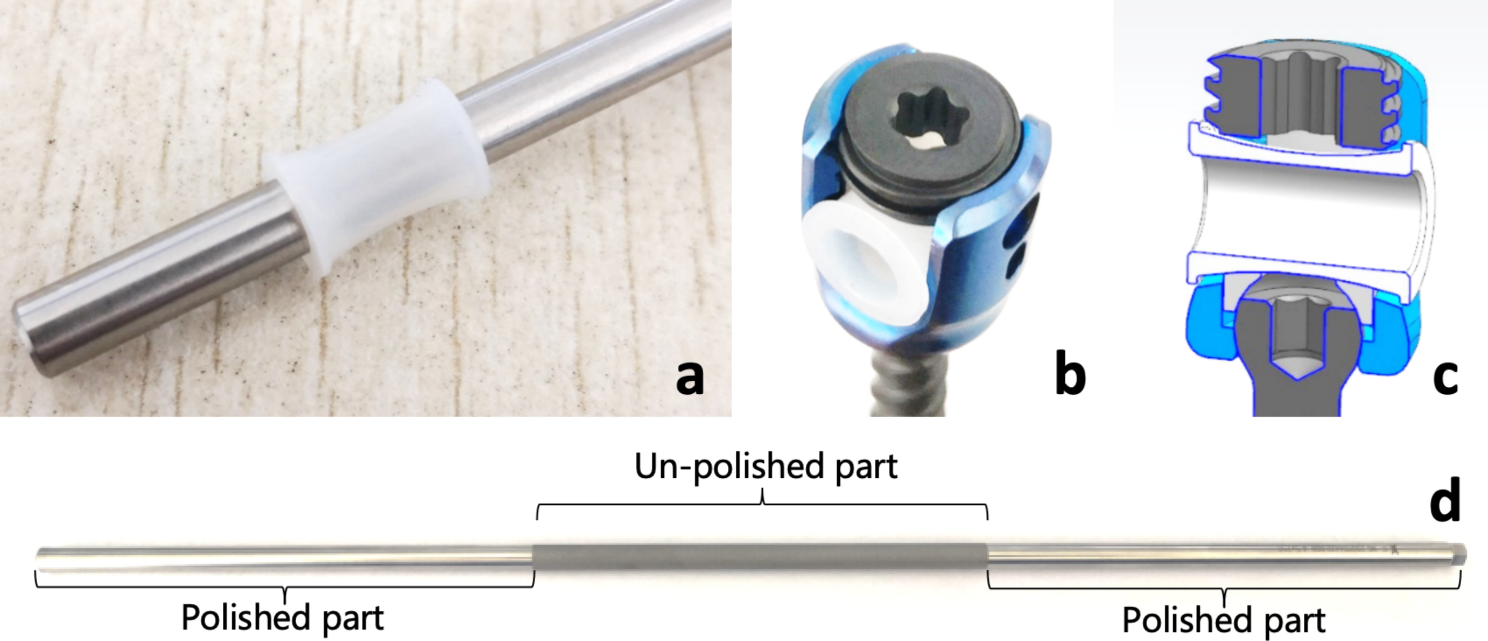
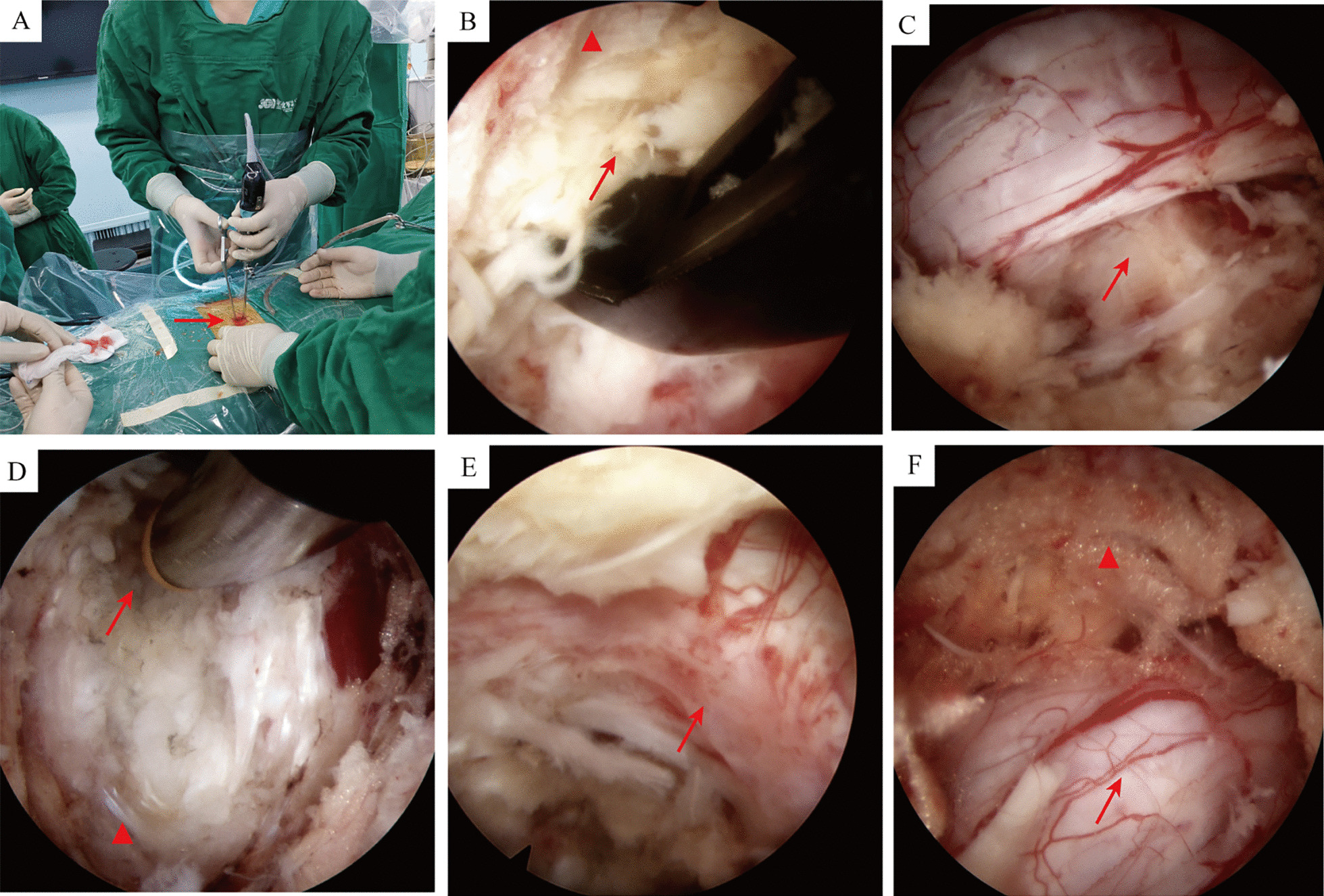
Surgical procedureObservation Group: After general anesthesia, the patients were placed in a supine position, and standard sterilization and draping were performed. For patients with significantly displaced pelvic fragility fractures, bone traction reduction was employed. The surgical procedure included the following steps: (1) 3D Image Acquisition: 3D images of the pelvic region were obtained and transferred to the Tianji screen. (2) Planning and Screw Placement: Suitable entry points and directions for screw insertion were selected to complete the planning of the target screws. (3) Tianji Orthopedic Robotic Arm Execution: The Tianji robotic arm was used to perform screw guide K-pins insertion to verify the position first. The spine vertebral body shaping cannula system was used to implant bone cement, followed by the insertion of the hollow cannulated screws under the guidance of fine guide pins, completing the technique of cement reinforcement at the screw end.
Control Group: The Tianji robotic system was used for image acquisition, planning, and conventional implantation of hollow cannulated screws for fixation.
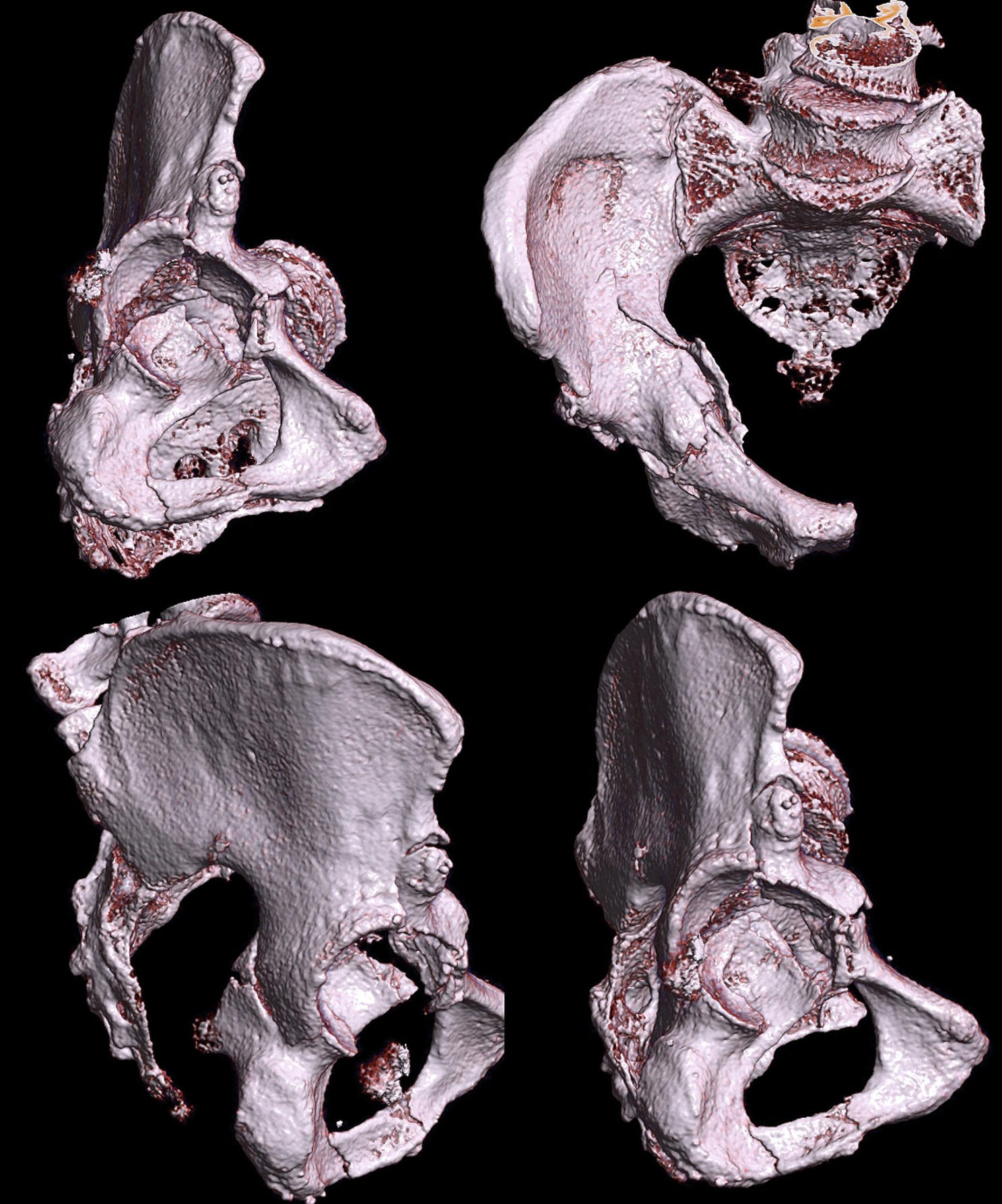
Fracture healing assessmentFracture healing was evaluated based on follow-up radiological findings and physical examinations. X-rays revealed a blurred fracture line with evidence of continuous callus formation. Additionally, there were no tenderness or axial percussion pain detected during the physical examination at the affected site, leading to the assessment of clinical healing of the fracture. It should be noted that our primary comparison focuses on clinical healing time and does not include functional aspects such as Majeed functional scores. The determination of patients’ clinical healing time in our study primarily relied on imaging data reviewed by specialized orthopedic and radiology professionals.
Majeed scoreThe Majeed Pelvic Score, a specific scoring system introduced in 1989, encompasses five aspects: pain, work, sitting, sexual activity, and standing, which is further divided into walking aids, unassisted gait, and walking distance. Each aspect is graded from excellent to poor, with higher scores indicating better patient recovery. The criteria for the Majeed Pelvic Score are as follows: for pre-injury employed individuals, a perfect score is 100 points, with scores > 85 considered excellent, > 69 to 85 good, > 55 to 69 fair, and ≤ 55 poor; for pre-injury unemployed individuals, the maximum score is 80 points, with scores > 70 considered excellent, > 55 to 70 good, > 45 to 55 fair, and ≤ 45 poor. According to the “Guidelines for Minimally Invasive Surgery for Pelvic Fractures in China (2021)”, the Majeed score is a commonly used method for assessing postoperative efficacy and follow-up of pelvic fractures.
Visual analog scale (VAS)VAS is a utilized tool of pain assessment. At one end of the scale, patients are presented with a descriptor indicating “no pain,” while the opposite end represents the most intense pain imaginable. Patients are then instructed to place a mark on the line that corresponds to their current pain level, with the distance from the “no pain” end serving as a numeric representation of pain intensity. Typically, this distance is measured in millimeters or centimeters, allowing for precise pain quantification. A score of 0 indicates no pain, and a score of 10 indicates unbearable severe pain.
Statistical analysisSPSS 19.0 was utilized for data analysis. The data are presented as median (interquartile range) or n (percentage), and statistical comparisons were conducted using the Mann-Whitney test or Fisher’s exact test or Chi-square test.
留言 (0)