
記住我

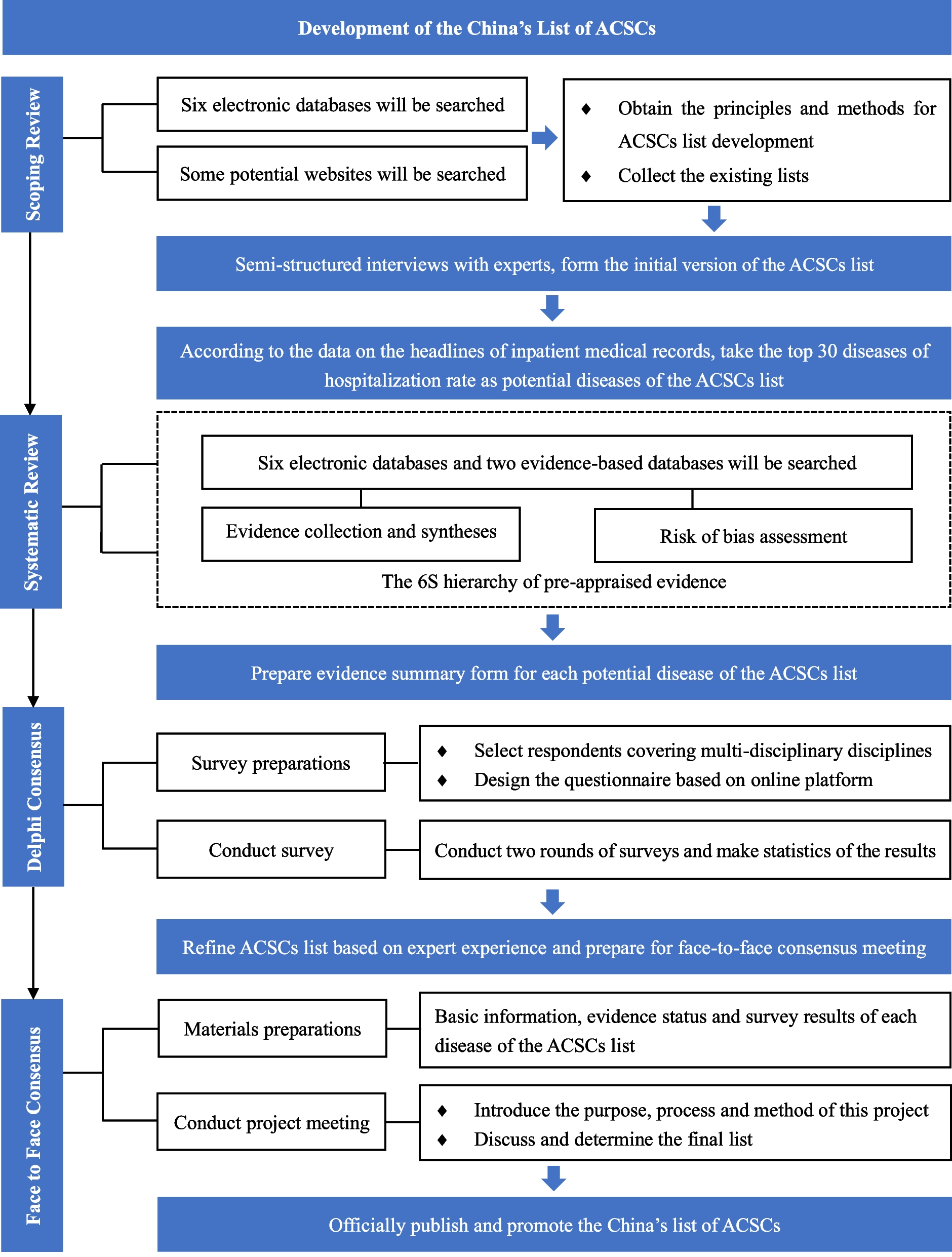
To develop China’s context-specific list of ACSCs, we will follow a proven multistep process used in the development of similar lists [5,6,7,8,9,10, 30,31,32,33,34,35], including scoping review, semi-structured interviews, descriptive study, systematic review, Delphi consensus survey and face-to-face consensus. Table 1 describes the multistep development process of the China’s ACSCs list, which includes: (1) establishment of working groups; (2) generations of the initial list; (3) optimization of the list; and (4) approval of the final list version. Figure 1 illustrates the development process.
Table 1 Description of the multistep development processFig. 1
Flowchart of the development process
Step I: establishment of working groupThe primary aim of this step is to identify individuals who are relevant to participant in the project. The working group will include: (1) an Advisory Group with seven participants; (2) a Delphi Panel with 21–29 participants; (3) an Evidence Review Team with eight participants; and (4) a Coordination Team with two participants. When determining the number of members in each group, we have taken into account both practical feasibility and the distribution of personnel in previous studies' working groups and clinical practice guidelines.
Advisory groupThe Advisory Group is a multidisciplinary group including seven researchers who have substantial experience in health policy making or evidence-based medicine, and have certain degrees of understanding of ACSCs. Specifically, they will be responsible for (1) establishing other working groups; (2) managing conflicts of interest; (3) approving development proposals; (4) examining and approving the final report; and (5) supervising the development process and providing advice and guidance when necessary.
Delphi panelThe Delphi Panel will incorporate 21–29 multidisciplinary representatives from across the country, with specialties in diverse areas such as clinical medicine, epidemiology, evidence-based medicine, health policy and health economics. At least 80% of these members are clinical workers, with half being general or primary care physicians. Specifically, they will be responsible for (1) voting until consensus is reached on the list's contents; and (2) finalizing the report.
Evidence review teamThe Evidence Review Team will incorporate eight researchers with experiences in evidence-based medicine. Their primary responsibilities include: (1) searching, evaluating, synthesizing, and grading evidence; and (2) creating summary tables to describe evidences identified.
Coordination teamThe Coordination Team is in charge of managing the project at different stages of implementation. They will coordinate the list development process and ensure its completion according to the established timeline. Specifically, the Coordination Team will be responsible for (1) coordinating the work of other working groups; (2) drafting and developing the protocol; (3) conducting semi-interviews, surveys and organizing consensus meetings; (4) documenting the entire list development process in details; and (5) preparing the preliminary draft of the report.
Step II: Generations of the initial listThe main purpose of this step is to develop the initial list, which is accomplished by reviewing published lists, further supplementing them through expert interviews, and selecting the diseases with the highest hospitalization rates in China as potential diseases of the China’s ACSCs list. It includes three sub-steps: (1) review of published lists by scoping review; (2) semi-structured interviews to understand participants’ views and experiences on ACSCs; and (3) calculation of hospitalization rates by a descriptive study to identify the top 30 diseases with highest hospitalization rates in China.
Review of published listsWe will search, review and classify the published literature and reports related to ACSCs and their development, collect the existing versions of lists, and obtain the principles and methods of ACSCs list development, specifically the criteria for including or excluding diseases of the list. These contents will also serve as key conditions and content in the subsequent semi-structured interviews, Delphi surveys, and face-to-face consensus.
The Evidence Review Team will systematically search the existing literature and reports regarding ACSCs based on six commonly used Chinese and English databases, including China National Knowledge Internet (CNKI), China Biology Medicine disc (CBMdisc), Wanfang Database, MEDLINE (via PubMed), Scopus, and Web of Science. There will be no publication status restrictions. To sort out the development methods of the ACSCs list and extract relevant disease information, e.g., specific types and codes, we will also conduct additional search on Google and the official websites of major international medical quality research institutions, including AHRQ, NICE, CIHI, OECD and World Health Organization (WHO). To minimize potential bias, literature searching, screening, and information extraction will be independently performed by two reviewers in pairs, and any disagreements will be resolved through discussion. Detailed inclusion and exclusion criteria are presented in Table 2.
Table 2 Inclusion and exclusion criteriaSemi-structured interviewsTo gather participants' views and experiences on ACSCs, as well as to explore potential relevant diseases for the initial version of the ACSCs list, semi-structured interviews will be conducted with relevant researchers of ACSCs, particularly focusing on clinical workers and general or primary care physicians. We will identify participants through convenience sampling with the support of the Advisory Group, contact them via emails, and conduct face-to-face or online interviews. The sample size will be guided by “information power” (a model for assessing the adequacy of sample sizes in qualitative research) [36, 37].
The interview outline will be determined by referring to previous studies, and in order to gain a wealth of information, the outline will be sent to the participants in advance. The main points of the interviews will include: (1) whether the diseases identified in the preceding step belong to China’s list of ACSCs, including whether timely and effective outpatient services can prevent potential avoidable hospitalizations, whether they can alleviate the condition and avoid aggravation once an incident occurs, as well as whether 48-h hospitalization is necessary when there is a hospitalization indication; (2) what other diseases can be added to the China’s ACSCs list that meet the above criteria; and (3) any additional matters concerning the development of the ACSCs list. Pre-interviews will be conducted when necessary to guarantee the successful completion of the interview.
Each interview is scheduled for approximately 40 to 50 min and will be recorded with the participant's consent for subsequent transcription. The interview records will be sent to the participants for check and approval. Since the views and experiences of participants are qualitative variables, we will summarize and draw conclusions based on content analysis [38]. The Coordination Team will review and verify the results. If a new disease is proposed by more than half of the participants, it will be added to the initial list. In case of disagreements, they will consult with the Advisory Group.
Calculations of hospitalization rateBy analyzing the data from the cover pages of inpatient medical records, which include patients' demographic information, admission details, and discharge information, we will identify the top 30 diseases with the highest hospitalization rates in China. The formula for calculating hospitalization rates is as follows:
$$Hospitalization\,rates=\frac\times 100\%$$
Since the hospitalization rates are quantitative variables, we will calculate absolute frequencies and proportions. Those diseases that are both found in the top 30 hospitalization rates list and the initial version of the list will be regarded as potential diseases. If feasible, the economic burden of the diseases will also be calculated and included as a criterion for selection.
In this step, we conjecture that certain diseases with high hospitalization rates may not necessarily be ACSCs and that certain diseases may have highly variable hospitalization rates due to large differences in treatment, both of which need to be determined in the subsequent steps.
Step III: Optimization of the listThe published list of ACSCs is primarily based on expert opinions rather than available evidence. Previous research indicates that selection of defined ACSCs should be based on evidence rather than expert view [34]. This step also incorporates the “evidence retrieval and synthesis” process in the guideline development [27,28,29], thus aimed to collect and synthesize the evidence of the previously identified conditions and consult with experts. The optimization of the list includes two sub-steps: (1) evidence evaluation of each potential disease in the list by systematic review; and (2) a Delphi consensus survey to identify appropriate diseases to be added into China’s list of ACSCs.
Evidence evaluationFor each potential disease, we will conduct a systematic evidence search, selection, evaluation and grading according to the evidence appraised principles of Fig. 2, which is adapted from the 6S hierarchy of pre-appraised evidence [39]. The electronic databases are six commonly used Chinese and English databases, including CNKI, CBMdisc, Wanfang Database, MEDLINE (via PubMed), Scopus and Web of Science, and two evidence-based medical databases e.g., the Cochrane Library and Epistemonikos. There will be no publication status restrictions. The evidence evaluation and grading tools are the most commonly used ones, which match the corresponding study types, for example, the AMSTAR tool for systematic reviews [40]. To minimize potential bias, literature searching, screening, and evidence evaluation and grading will be performed by two reviewers in pairs independently. In addition, corresponding evidence summary forms will be created for each potential disease to be further investigated via Delphi consensus surveys.
Fig. 2
The evidence appraised principles
Delphi consensus surveyThe purpose of the Delphi consensus survey is to revise the ACSCs list based on expert experiences to further obtain face-to-face consensus. We will identify the respondents through online queries combined with recommendations from the Advisory Group, and build a multidisciplinary team of experts from all over the country, with an emphasis on including a higher proportion of clinicians as previously mentioned. We will conduct two rounds of surveys based on "Wenjuanxing" (https://www.wjx.cn/app/survey.aspx) to collect opinions and provide feedbacks to respondents. To eliminate possible interference, feedbacks will be anonymized with basic information of the respondents. Consistency in participants across both surveys is maintained, with those in the second round having the option to abstain due to special circumstances. Moreover, we will thoroughly evaluate potential conflicts of interest among participants to ensure that all respondents have no significant conflicts of interest.
The Delphi surveys focus on whether the diseases determined from preceding steps are really belong to the China’s ACSCs list, comprehensively considering existing evidence and real practice, and whether there are any other conditions that meet the criteria but have not yet been included. Detailed background information on this project will be explained in the questionnaire to prevent participants from distorting their opinions and answers. For each potential disease added into the ACSCs list, the respondents can exclusively select "agree", "disagree" or "not sure", or they can add other relevant important diseases and with further explanations on the underlying reasons. After the survey, the Coordination Team will summarize the survey results, collect all suggestions and comments, and revise and improve the ACSCs list according to those suggestions and comments. Diseases with more than 75% "agree" from respondents will be included in the list, and those with more than 50% "disagree" from respondents will be deleted. The ACSCs list will be listed in descending order according to the survey results.
Step IV: approval of the final list versionWe will organize a face-to-face consensus meeting to determine the final version of ACSCs list that contains diseases and codes applicable under the context of China’s healthcare system. Based on the results of the Delphi survey, the Coordination Team will compile the names, codes, evidence status, and the percentage of "agree" received from respondents for each disease included in the ACSCs list. We will create a final report to be disseminated among attendants for the consensus meeting. The Coordination Team will also determine the meeting time, duration (3–5 h), and location of the meeting, create the agenda and make relevant arrangements.
Prior to the meeting, the Advisory Group will conduct an updated assessment of potential conflicts of interest among all participants to ensure that no respondent has a significant conflict of interest. At the meeting, the chairman will introduce the participants and the meeting topic, provide the documents to be published with related information and evidence. Meanwhile, a brief introduction will be given to describe the main purposes and processes of the development of the ACSCs list in details. All participants, especially members of the Coordination Team and the Advisory Group, will need to review and reach consensus (≥ 75%) on the contents of the final version of the list through consensus discussion, which will be further disseminated via peer-reviewed journals, newspapers, academic conferences and other approaches.
Patient and public involvementPatient preferences and values are a major factor when it comes to selecting health services. The evaluation of medical quality not only considers the accessibility of health services and health outcomes, but also includes the patient's experience and satisfaction. To account for the preferences and values of patients and the public in seeking health services, we will include two or three relevant representatives in the face-to-face consensus process. Our strategy for participant enrollment entails the use of convenient sampling, targeting individuals with common or widespread diseases and their caregivers. However, due to logistical limitations, it is not possible to enlist representative patients for each specific condition. Consequently, we will favor those with enhanced health literacy to ensure the ease of gathering their insights.
留言 (0)