Demographic characteristics of rural households
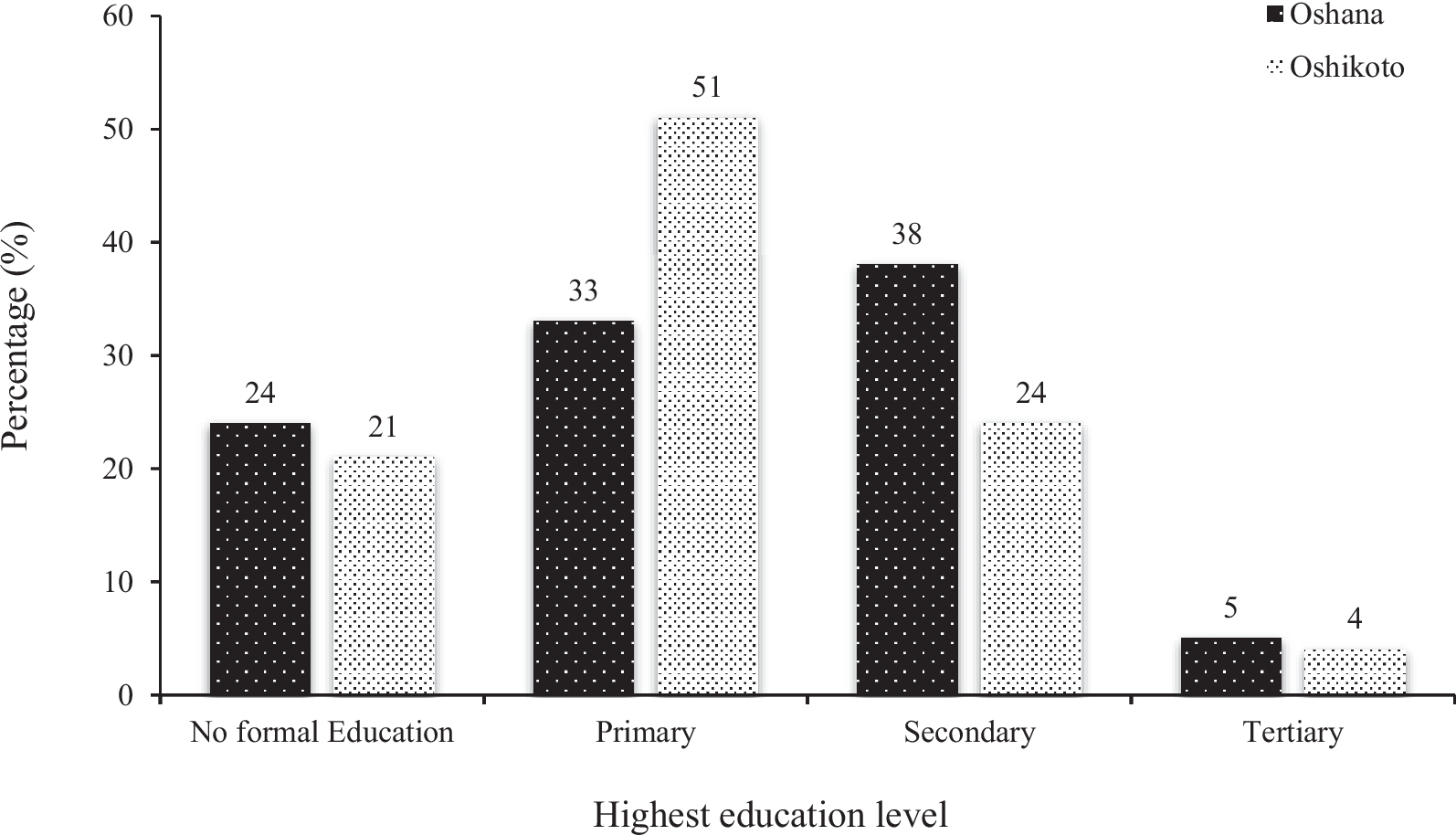
The demographic data showed that, only 5% and 4% of the childcare providers from Oshana and Oshikoto regions, respectively received tertiary education. The low level of education among them could be attributed to the cultural practice in rural areas where most women are married at an early age as well as to high rates of teenage pregnancies in rural areas which lead to early school dropouts [18]. Also, childcare providers from both regions were mostly subsistence farmers and this could be explained by the low level of education among the respondents which may be contributing to inability of securing better employment. Policy interventions focused on nutrition and childcare for childcare providers are recommended.
Six months of exclusive breast feeding is highly recommended by the World Health Organization as the breastmilk is a vital source of sustenance to children [19]. Additionally, breastmilk is known to have a significant effect on cognition, behavioural, and mental health in children [20]. Therefore, this may support the findings of this study that majority of the children were breastfed for more than 12 months and majority of them (95.8%) do not experience any health challenge as reported by their care providers. This study found a significant association between breastfeeding length and wasting in Oshikoto region. It is therefore important that children be exclusively breast-fed for the first 6 months of life as recommended by WHO and thereafter they should be fed complementary foods that are nutritionally safe and adequate while continuing to be breast-fed until 2 years and above [12]. At policy levels, it is recommended that initiatives that support and educate mothers on benefits of extended breastfeeding be implemented and strengthened.
Food consumption pattern
A diversified diet is essential for children to meet their nutritional demands and ensure normal health, growth, and development. The dietary diversity scores in this study refers to the number of main food groups that were consumed by under 5 years children for the minimum of 5 days in a week. The mean dietary diversity scores of children from Oshana and Oshikoto regions were 4±1 SD and 5±1 SD, respectively. These figures were higher than those reported in a study conducted in Ghana [21]. The minimum dietary diversity scores among children from the Oshana and Oshikoto regions aligned with those documented in children from Sub-Saharan Africa in previous studies [14, 21,22,23].
A low dietary diversity score observed among the children in this study indicates that most children, primarily in Oshikoto region, are unlikely to meet their nutritional demands. This suggests the need to implement community-based programs to educate childcare providers about the importance of diversified diets and supporting initiatives that enhance agricultural practices in rural areas. For instance, establishing community gardens to ensure the availability of a variety of nutrient-rich food crops in rural areas. However, this study did not establish an association between minimum dietary diversity and nutritional status. These results are consistent with the study of [24]. Other studies in Africa have found an association between dietary diversity and nutritional status [14, 25,26,27].
Grains, roots and tubers and flesh foods, were popularly consumed by children from both regions, followed by legumes and nuts, as well as other fruits and vegetables. These consumption patterns are in accordance with the findings of other studies [25, 28, 29].
The high consumption of staple food among children in rural household of Oshana and Oshikoto regions may also be attributed to their availability in terms of socioeconomic status, cultural beliefs, and traditional dietary practices. Jang [30] reported that, socio economic status may affect and defines the availability of food in terms of quantity and quality as well as in relation with cultural and food practices in the households. Thompson and Amoroso [31] further reported the existence of a shift from diverse diets to the diets that are mainly high in carbohydrates in the Sub-Saharan Africa, due to declining incomes. Oniang’ o, Mutuku and Malaba [32] also reported that, in African communities, locally available staples such as maize, cassava and sweet potatoes generally form the basis of a meal, which is complemented with legumes or food from animal sources to make the meal nutritious. These findings align with this study, as staple cereals, ombidi, beans, chicken, beef, oshikundu and fish were amongst the foods that were mostly consumed by the children in a week.
The low consumption of dairy products, eggs or vitamin A-rich fruits and vegetables in this study have also been documented by previous authors [33, 34]. This is a nutritional concern among these populations, as WHO recommends frequent consumption of eggs, fruits, and vegetables for optimal growth and development [12].
The consumption of vitamin A rich fruits and vegetables among the study subjects was the least compared to other foods such as cereals. However, vegetables such as ombidi and beans were mostly consumed by the children from both regions, and this may be attributed to their local availability in the regions. The low consumption of variety of fruits and vegetables by the study subjects is consistent with that of Anane and co-workers [28] who found out that consumption of grains, root, and tubers were relatively higher in their study but low for Vitamin A-rich fruits and vegetables for under five years children in Ghana. The study findings also concur with that of Vahatalo and co-workers [29] who observed a high consumption of millet, maize and milk as well as an extremely low consumption of fruits and vegetables among children in Kaokoland in Namibia. Fruits form a basic part of healthy nutrition despite their low consumption pattern in the study. They provide vitamins, minerals, fibre, as well as many vital substances, which aid in preventing non-infectious diseases such as cardiovascular disease, diabetes and cancer [35]. The daily consumption of fruits and vegetables is also highly recommended by the food and nutrition guidelines for Namibians [36]. However, the low consumption of fruits and vegetables in the study may also be influenced by the availability of fruits in the region, education level and affordability [37]. However, this study could not find an association between education level and food consumption. Nevertheless, the low consumption pattern of fruits in the study may indicate unhealthy and unbalanced dietary food consumption among rural children, which may subsequently escalate susceptibility to various diseases and children mortality.
The findings of this study also revealed that, majority of the children from Oshana and Oshikoto regions were fed food that was either produced at home and from the market. These findings align with research results reported by other studies [38, 39]. The consumption pattern observed in this study might also be influenced by economic and climatic factors. Namibia being one of the African countries which are affected by drought, experiences minimal agricultural production [40]. Despite most childcare providers being subsistence farmers, they are unable to produce sufficient food for their families, leading to the necessity to supplement their staple food by purchasing items from the market.
Additionally, the study found that the proportion of children receiving solid, semi-solid, or soft foods per day differed between the two regions. Children from Oshikoto mostly consumed meals 1 to 3 times a day, while those from Oshana mostly consumed meals 4 to 6 times a day. The recommended minimum meal frequency for non-breastfeeding children is 4 or more meals a day [12]. A higher proportion of children (70%) from the Oshana region met the recommended minimum meal frequency compared to children from the Oshikoto region (32%). The minimum meal frequency for both regions was lower than those reported by Belew and co-workers [22]. Additionally, the minimum meal frequency for the Oshikoto region was lower than the 41.9% reported in Sub-Saharan Africa [41], but the recorded 41.9% in Sub-Saharan Africa was also lower than that found in the Oshana region.
The low minimal meal frequency observed in the Oshikoto region indicates that most children were not meeting their energy requirements, suggesting vulnerability to malnutrition [42]. The lower frequency of food consumption per day among some of the study participants may be attributed to limited food availability in rural households and poor income. The families might have insufficient income to purchase a variety of food for their children, leading them to be fed only a few times a day, conserving food for the next day. This is supported by Anane and co-workers [28] who revealed that, food affordability and availability may affect the consumption of food among children. The children from rich families tend to consume more food compared to those from poorer families.
Most children consumed either 375g or 250g of food per meal, and only a few had more than 7 meals a day or consumed 500g of food per meal across both regions. These patterns of meal consumption are consistent with the observations made by Williams and Smith [39].
Furthermore, a small proportion (27% and 0.5%) of the children from Oshana and Oshikoto regions respectively, were fed a minimum acceptable diet. A minimum acceptable diet is crucial to children for their growth and development, despite its low prevalence in this study. However, this study could not establish a significant association between minimum acceptable diet and nutritional status. The lack of association between minimal acceptable diet and nutritional status is in accordance with the findings of Niyigena and co-authors [24]. The low prevalence of minimum acceptable diet indicates the risk of children to malnutrition. It is therefore important that children maintain an adequate dietary intake to attain their daily energy by consuming a varied, healthy, and balanced diet. This underscores the importance of fostering collaboration with health care facilities and conducting awareness campaigns in rural areas to educate childcare providers on proper feeding practices and nutrition for children. Moreover, implementation of policies becomes imperative to improve food environments and eliminating access barriers to diversified diets, thereby mitigating high prevalence of malnutrition among rural children.
Nutritional status
Anthropometric measurements are normally used in the assessment of nutritional status of individuals in communities. Evaluation of the nutritional status of people was established to be a crucial tool in public health and a possible indicator of living standards [43]. According to the findings of this study, the recorded prevalences of wasting, and underweight from the two regions are in line with the survey results of Fred [44] in Namibia who reported that, nearly 9% of the children were wasting and 26% were underweight. The prevalence of wasting and underweight among the children under 5 years has also been reported in previous studies in rural areas of Sub-Sahara Africa, however their figures were found higher than for this study [44,45,46,47]. However, this study may potentially overlook children who were wasting as bilateral pitting oedema was not assessed.
The prevalences of stunting recorded in this study for Oshana and Oshikoto regions are higher than the findings of the Namibian Demographic and Health Survey (NDHS) (2013) which reported that nationally, 24% of children under five years were stunted and 8% were severely stunted with a high percentage of stunting accounted for children from rural areas [4]. The stunted children’s heights were found to be lower, relative to their ages and this is an indicator of chronic malnutrition among those children.
Even though the results of the study showed that many of the children who participated in the study had normal weight for age, normal height for age and normal weight for height, the observed prevalence of wasting (24.6%), overweight (5.6%), underweight (18.1%), and stunting (29.8%) are a source of public health concern. Thus, improvement of the health and nutritional status of children through adequate dietary intake can diminish the effects of malnutrition on growth and development of rural children. Several studies have documented the factors that are responsible for stunting and wasting among the children under 5 years. These factors include inappropriate infant feeding practices, optimal duration of exclusive breastfeeding, socioeconomic status (education level, occupation, household income) as well as living in rural areas [45, 48, 49].
This study observed the associations between breastfeeding length, the amount of food consumed, frequency of food consumption/MMF and the types of food consumed by children under the age of 5 with wasting. The consumption of pearl millet thick/ thin porridge, fresh fish consumption and higher frequency of meal consumption was associated with a significant decrease in the odds of having severe/moderate wasting, suggesting a strong protection against wasting which is of practical importance. Whereas an increase in the amount of food was associated with the increase in the odds of children being moderately wasted. Conversely, longer breastfeeding duration showed a non-significant decrease in the odds of severe overweight (p > 0.05), suggesting insufficient evidence to conclude a significant effect on severe overweight odds.
Nevertheless, the observed associations between food consumption patterns and nutritional status in this study align with those reported by other authors [50, 51] and are consistent with several studies in Africa and Asia which indicated that, the amount of food (small portion sizes), inadequate dietary diversity and low meal frequencies contribute to poor nutritional status of children including stunting, wasting or underweight [52,53,54,55]. Underweight and wasting are forms of acute malnutrition which may results from recent food deficit, thus, a reduced frequency of meal consumption among children, which was also observed among some of the study participants may result in low energy levels escalating the risk of adverse nutritional status [53].
Additionally, staple cereals which are regularly consumed in the study may contain natural toxicants which may potentially interfere with the absorption of essential micronutrients from foods consumed by children [50]. This could result in compromised nutritional status such as wasting which was linked to the consumption of pearl millet thick/thin porridge among the study participants. Hence, there is a crucial need for a comprehensive investigation into the natural toxicants present in these staple foods. Moreover, an association was observed between beans consumption and overweight among children from Oshana region. However, it was noted that vegetables consumption appeared to be linked to a reduction in overweight cases [56]. These findings suggest that other factors including dietary feeding practices (example; the consumption of food high in saturated fat and sugar) as well as lack of physical activities might be the potential contributors to overweight among these children [57]. However, to gain a comprehensive understanding of the complex factors influencing overweight among these children, further research needs to be conducted. Promoting healthy dietary habits and addressing the underlying socio-economic factors that may influence food consumption patterns in rural areas may improve the nutritional status and overall health of children.




留言 (0)