
記住我










Background: Cognitive behavioural therapy (CBT) has been shown to be effective for several psychiatric and somatic conditions; however, most randomized controlled trials (RCTs) have administered treatment in person and whether remote delivery is similarly effective remains uncertain. We sought to compare the effectiveness of therapist-guided remote CBT and in-person CBT.
Methods: We systematically searched MEDLINE, Embase, PsycINFO, CINAHL, and the Cochrane Central Register of Controlled Trials from inception to July 4, 2023, for RCTs that enrolled adults (aged ≥ 18 yr) presenting with any clinical condition and that randomized participants to either therapist-guided remote CBT (e.g., teleconference, videoconference) or in-person CBT. Paired reviewers assessed risk of bias and extracted data independently and in duplicate. We performed random-effects model meta-analyses to pool patient-important primary outcomes across eligible RCTs as standardized mean differences (SMDs). We used Grading of Recommendations Assessment, Development and Evaluation (GRADE) guidance to assess the certainty of evidence and used the Instrument to Assess the Credibility of Effect Modification Analyses (ICEMAN) to rate the credibility of subgroup effects.
Results: We included 54 RCTs that enrolled a total of 5463 patients. Seventeen studies focused on treatment of anxiety and related disorders, 14 on depressive symptoms, 7 on insomnia, 6 on chronic pain or fatigue syndromes, 5 on body image or eating disorders, 3 on tinnitus, 1 on alcohol use disorder, and 1 on mood and anxiety disorders. Moderate-certainty evidence showed little to no difference in the effectiveness of therapist-guided remote and in-person CBT on primary outcomes (SMD −0.02, 95% confidence interval −0.12 to 0.07).
Interpretation: Moderate-certainty evidence showed little to no difference in the effectiveness of in-person and therapist-guided remote CBT across a range of mental health and somatic disorders, suggesting potential for the use of therapist-guided remote CBT to facilitate greater access to evidence-based care. Systematic review registration: Open Science Framework (https://osf.io/7asrc)
Cognitive behavioural therapy (CBT) is a form of psychotherapy that focuses on the identification and modification of unhelpful thoughts and behaviour patterns and has been shown to be effective for a wide range of mental health and somatic disorders. 1–5 For example, a 2022 systematic review found moderate-certainty evidence that CBT delivered with physiotherapy probably resulted in large improvements in pain relief and physical functioning for patients with chronic low back pain, compared with physiotherapy alone.6 In 2022, more than 5 million Canadians (18.3%) met diagnostic criteria for a mood, anxiety, or substance use disorder,7 and 1 in 5 adults live with chronic pain.8 In 2019, the World Health Organization advised that access to CBT was essential for evidence-based health care;9 however, treatment access is an important barrier to care for people with mental health disorders10 and those with somatic disorders such as chronic pain.11 Access is particularly an issue in a country as geographically large and sparsely populated as Canada.
In Canada, CBT may be provided within existing government-funded health care services (e.g., hospital settings) and by private providers such as registered psychotherapists, social workers, and psychologists, in which case people without private insurance must pay out of pocket. In an effort to increase access, the government of Saskatchewan began providing funding for Internet-based CBT in 2015,12 as did the Ontario Ministry of Health through the Ontario Structured Psychotherapy Program, starting in 2020;13 however, the relative effectiveness of in-person and remote CBT is uncertain.
A previous systematic review addressed this question, searching the literature up to February 2017, and found that Internet-based CBT may be similarly effective to in-person CBT, but suggested that effectiveness could differ by the clinical condition being targeted.14 A 2019 health technology assessment by Health Quality Ontario found that Internet-delivered CBT was more effective than waitlist control for mild to moderate depression and social anxiety disorder, and may be effective for anxiety and panic disorder, but concluded the relative effectiveness of Internet-delivered CBT and in-person delivery was uncertain.10 Given that these 2 reviews restricted their searches to English-language trials, several relevant trials have been published since their literature searches were conducted, and neither review conducted analyses to explore subgroup effects, we sought to compare the effectiveness of therapist-guided remote CBT and in-person CBT by conducting a systematic review and meta-analysis.
MethodsWe registered the protocol for our systematic review on the Open Science Framework (https://osf.io/7asrc), adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) reporting checklist,15 and followed Grading of Recommendations Assessment, Development and Evaluation (GRADE) guidance.16
We made 4 changes to our registered protocol. We increased the sensitivity of our literature search strategy by introducing terms to capture randomized controlled trials (RCTs) that administered CBT via telephone and telehealth. We included the Cochrane Central Register of Controlled Trials (CENTRAL) among the databases that we searched and conducted a subgroup analysis of RCTs that administered CBT on an individual basis versus group therapy. Finally, we conducted a sensitivity analysis by pooling the effect of remote versus in-person CBT for depression in natural units (i.e., original, unaltered units) of the most commonly reported outcome measure among eligible trials.
In our systematic review, we explored the comparative effectiveness of therapist-guided remote and in-person CBT on primary patient-important outcomes among adults presenting with any clinical condition.
Data sourcesA medical librarian (R.J.C.) initially developed database-specific search strategies without language restrictions and searched MEDLINE, Embase, PsychInfo, and CINAHL from inception to May 11, 2022. We subsequently expanded our search strategy terms to increase sensitivity, included an additional database (CENTRAL), and re-ran our search of all 5 databases from inception to July 4, 2023 (Appendix 1, available at www.cmaj.ca/lookup/doi/10.1503/cmaj.230274/tab-related-content). One of the reviewers (S.Z.) searched the reference lists of all eligible articles and relevant systematic reviews to identify additional studies.
Eligibility criteria and study selectionWe included RCTs that enrolled adult patients (aged ≥ 18 yr) who were seeking treatment for any clinical condition, randomized to receive either therapist-guided remote CBT (e.g., teleconference, videoconference) or in-person CBT. We excluded studies that administered CBT without therapist guidance or studies that administered virtual reality treatments in which a therapist accompanied the patient, in person, during treatment. We also excluded RCTs that administered modalities of psychotherapy other than standard CBT (e.g., acceptance and commitment therapy, mindfulness-based CBT, dialectical CBT) or that administered CBT in addition to another psychological intervention (e.g., motivational interviewing).17
Pairs of reviewers independently screened titles and abstracts of identified citations and full texts of all potentially eligible studies. One author with graduate training in psychology (S.Z.) reviewed all citations and potentially eligible full-text articles, with an independent review by a second reviewer (M.A., B.E.I., L.Y., A.P., K.T., H.C.). The pairs of reviewers resolved discrepancies through discussion to achieve consensus or with involvement of a third reviewer (J.W.B.), if necessary. We used online systematic review software (DistillerSR, Evidence Partners) to facilitate literature screening.
For all full-text articles deemed by a reviewer to be potentially eligible for inclusion, a clinical expert (P.B.), blinded to trial results, assessed the intervention details to confirm eligibility. A second clinical expert (R.E.M.), also blinded to trial results, independently reviewed a subset of full-text articles (43%) where reviewers were uncertain as to eligibility. Agreement between clinical experts on the RCTs they both reviewed for eligibility was perfect.
Data extractionEach eligible RCT underwent duplicate data abstraction by pairs of trained reviewers (S.Z., M.A., B.E.I., L.Y., A.P., K.T.) working independently and using standardized, pilot-tested forms. Reviewers resolved disagreements through discussion or with the help of a third reviewer (J.W.B.).
We collected information on study characteristics, patient characteristics (as per study report), and treatment details (e.g., number of sessions, compliance rate, therapist background, level of therapist involvement, safety).
We extracted the effect on a patient-important primary outcome for each RCT, which we selected using the following hierarchy. 18 We first looked for the outcome declared as the primary outcome by the trial authors; otherwise, we chose the outcome measure used for sample size calculation or, lastly, we chose the first patient-important outcome reported in the results section of the publication. We defined a patient-important outcome as one for which, if the patient knew that this outcome was the only thing to change with treatment, they would likely elect to receive treatment.19 We included outcomes reported by patients, but not surrogate outcomes (e.g., changes in blood pressure). When outcome data were available at several time points, we used data from the longest follow-up.
Risk of biasSix reviewers (S.Z., M.A., B.E.I., L.Y., A.P., K.T.) used the Cochrane risk-of-bias tool for RCTs (RoB 2)20 to assess 5 domains, independently and in triplicate, namely bias arising from the randomization process, deviations from the intended intervention, missing outcome data, bias in measurement of the outcome, and bias in the selection of the reported results.
Pairs of reviewers (S.Z., M.A., B.E.I., L.Y., A.P., K.T.) explored selective outcome reporting by comparing the reported results with those proposed in the study protocol (if published or publicly available through a clinical trials registry, otherwise by comparing the reported results with those proposed in the study methods). Each trial was designed as having low risk of bias, high risk of bias or some concerns regarding bias.
Statistical analysisWe measured inter-rater agreement of the decision to include an RCT after reviewing the full-text paper using an adjusted κ statistic. 21 All patient-important primary outcomes across eligible trials were continuous but measured diverse domains with a range of instruments. For each study, we acquired the change from baseline for their primary outcome in each treatment arm. When a change score was not provided, we used mean values at baseline and end of follow-up to calculate the change score. When the standard deviation (SD) for change from baseline was not reported, we used methods described by Weir and colleagues22 and the Cochrane handbook to impute this value.23
We used the change score and associated SD for therapist-guided remote and in-person CBT to calculate the between-group standardized mean difference (SMD) using the metan package in Stata.24 We pooled effect estimates using a random-effects model and the DerSimonian–Laird method25 to derive the pooled SMD and associated 95% confidence interval (95% CI).23 We used Cohen’s d thresholds for classifying the magnitude of the SMD as small (0.20), medium (0.50), or large (0.80).26
We pooled the difference in compliance between in-person and remote therapist-guided CBT as the relative risk (RR) and 95% CI using a random-effects model. We rated the compliance thresholds used in RCTs as high (i.e., requiring patient to complete 100% of modules to be considered compliant), moderate (50%–80% of modules completed), or low (< 30% of modules completed).
We performed all statistical analyses using Stata version 17.0 (StataCorp LP). Comparisons were 2-tailed, and we set our level of statistical significance at p of 0.05 or less.
Subgroup analyses and meta-regressionWe used visual inspection of forest plots and the I2 statistic to determine statistical heterogeneity for our pooled effect estimate. 27 Following Cochrane guidance, heterogeneity of 0%–40% was considered as perhaps unimportant, 30%–60% as moderate, 50%–90% as substantial, and 75%–100% as considerable.23 We used meta-regression to establish if a priori factors explained between-study variability for the primary outcome, as long as 2 or more studies were in each subgroup, including clinical condition, whether CBT was provided individually or in group therapy, length of follow-up, and risk of bias.28 Our clinical experts (R.E.M., P.B.) did not anticipate that the delivery format of CBT would show systematic differences in effectiveness based on specific clinical conditions. We also used meta-regression to evaluate the association between number of treatment sessions and compliance rate by in-person or remote CBT.
We presented all subgroup analyses as forest plots to visualize differences. We assessed the credibility of statistically significant subgroup effects in regression analyses (test of interaction p ≤ 0.05) with the Instrument for Assessing the Credibility of Effect Modification Analyses (ICEMAN).29
Certainty of evidenceTwo reviewers (J.W.B., S.Z.) used the GRADE approach to summarize the certainty of evidence for our meta-analysis of primary outcome measures. With GRADE, evidence from RCTs begins as high certainty but may be rated down based on risk of bias, indirectness, imprecision, inconsistency, or small study effects.30 We considered the pooled effect estimate to be precise if the associated 95% CI included only 1 magnitude of effect based on Cohen’s d thresholds (i.e., large [0.8], medium [0.5], small [0.2], or less than small).26
If we found a credible subgroup effect among RCTs at low, some concern, and high risk of bias, we presented the pooled effect for studies at low risk of bias. If no significant subgroup effect was found, we pooled across all RCTs and did not rate down for risk of bias.23 We evaluated small-study effects with contour-enhanced funnel plots and the Egger test for continuous outcomes or the Harbord test for dichotomous outcomes.31
Sensitivity analysisWe conducted a sensitivity analysis by pooling end-of-study scores for primary outcomes instead of change scores. Post hoc, we pooled treatment effects in natural units among eligible RCTS that enrolled patients with depression to illustrate the comparative effectiveness of in-person versus therapist-guided remote CBT. We selected depression among presenting clinical conditions as this was the most common condition reported among eligible RCTs in which the same outcome measure, the Beck Depression Inventory-II (BDI-II; minimally important difference = 5 points),32 was often reported. We converted other measures of depression to the BDI-II using a validated approach,33 and pooled between-group change scores across RCTs as the weighted mean difference and 95% CI, and used the DerSimonian–Laird method and a random-effects model.25
Ethics approvalWe did not seek ethics approval for this systematic review and meta-analysis of published data.
ResultsOf 19 115 unique citations, 54 studies were34–87 eligible for review, including 52 English-language RCTs34–79,82–87 and single RCTs published in Mandarin80 and Persian,81 with a total of 5463 participants (Figure 1). Our original search yielded 32 eligible studies, with an additional 22 studies included with the expanded and updated search strategy (Appendix 1). At the full-text review stage, reviewers had almost perfect agreement (κ = 0.81). One RCT assigned participants to 3 arms (12 sessions of in-person CBT, 6 sessions of in-person CBT, and 6 sessions of remote CBT);63 we included data from the 2 arms with the same number of sessions. Another RCT randomized patients to 3 arms (CBT delivered in-person at the patient’s home, in-person CBT at a therapist’s office, or remote CBT);44 we combined data from both in-person CBT arms for our analysis.
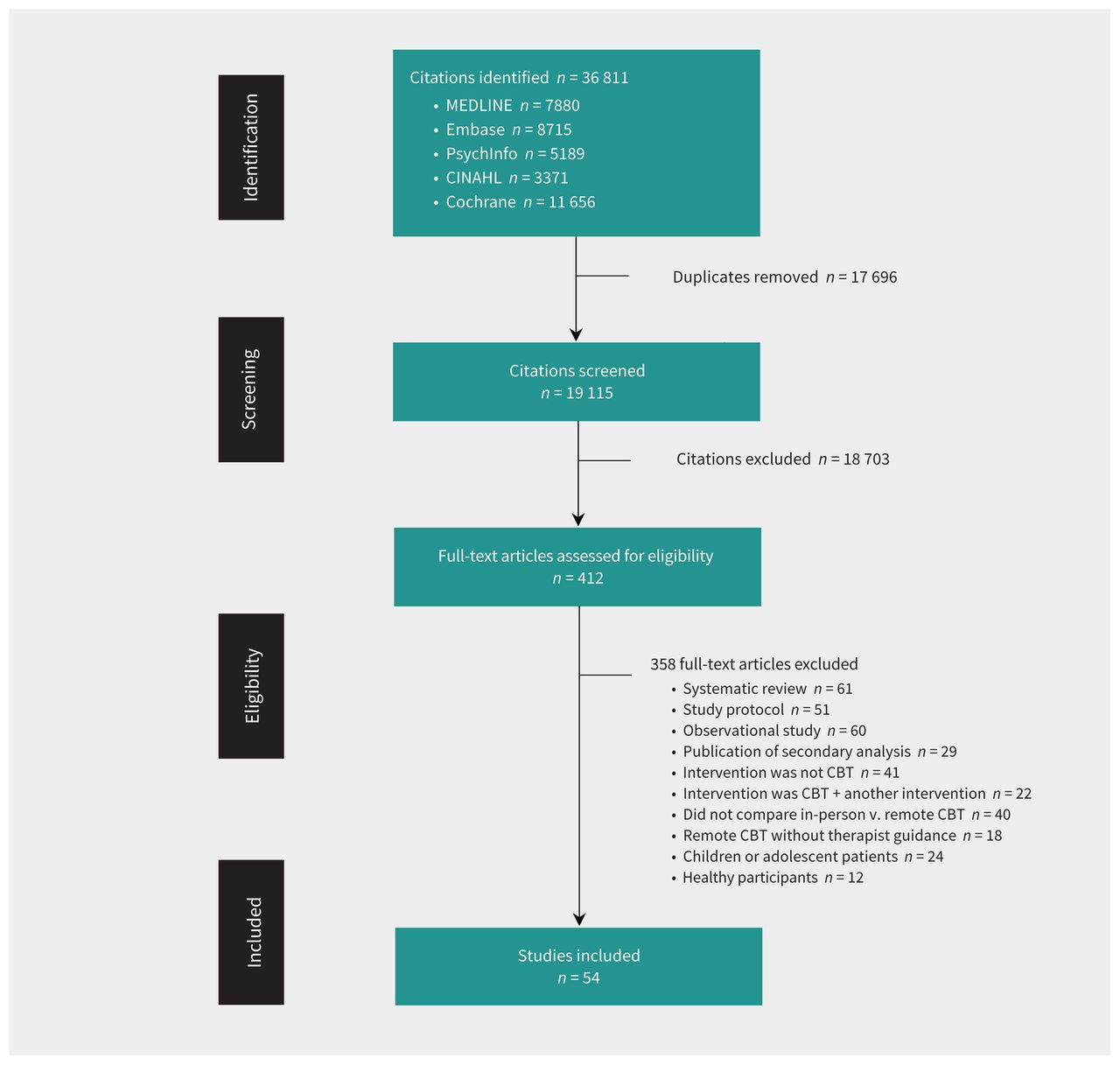 Figure 1:
Figure 1: Flow diagram of study inclusion. Note: CBT = cognitive behavioural therapy.
Eligible studies enrolled a median of 80 (interquartile range [IQR] 52–125) patients, 3354 (61.4%) of 5463 participants were female, and among the 52 RCTs that reported age, the median of the average age was 43 (IQR 35–51) years. Trials enrolled patients presenting with anxiety-related disorders (n = 17), depression and mood disorders (n = 14), insomnia (n = 7), chronic pain or fatigue syndromes (n = 6), body image or eating disorders (n = 5), tinnitus (n = 3), mood and anxiety disorders (n = 1), and alcohol use disorder (n = 1) (Table 1).
Table 1:Study characteristics
For delivery of CBT, 19 studies (35%) randomized patients to group therapy, whereas 32 (59%) provided individual therapy; 2 studies (4%) did not specify how CBT was provided and 1 RCT (2%) administered both group and individual therapy. Types of remote CBT included interactive voice response technology,34 computerized CBT,39,51,55,58,63 telehealth and telephone-based CBT,44,64,65,67,69,71,72,74,76–79,82–85 videoconference,57,66,68,73,75,86,87 and Internet-delivered CBT.35–38,40–43,45–54,56,59–62,70,80,81
Involvement of therapists in CBT interventions delivered remotely was variable. For 25 RCTs, remote CBT was delivered in real time by a therapist, requiring a time commitment equivalent to in-person CBT. For the remaining 29 RCTs, therapists supported remote CBT modules that patients completed on their own; when details on time spent by therapists was reported, the time commitment typically involved 10–30 minutes per module for responding to patient queries and evaluating submitted homework (Appendix 1, eTable 1).
Treatment duration ranged from 5 to 21 (median 10, IQR 7–12) sessions, and the median length of follow-up was 180 (IQR 90–252) days (Table 1). Among the 44 RCTs that reported patient compliance (Appendix 1, eTable 2), subgroup analysis found no significant difference between in-person or therapist-guided remote CBT; however, effects for moderate-and high-compliance thresholds showed substantial heterogeneity (Figure 2). Meta-regression also found no significant difference in compliance based on the number of treatment sessions for RCTs with high (p = 0.80), moderate (p = 0.07), or low (p = 0.75) compliance. We found no evidence of small study effects among RCTs reporting patient compliance (Appendix 1, eFigure 1 and eFigure 2).
 Figure 2:
Figure 2: Effect of patient compliance with remote versus in-person cognitive behavioural therapy (CBT). Weights are from random-effects model; continuity correction applied to studies with 0 cells. Note: CI = confidence interval, DL = DerSimonian–Laird, RR = risk ratio.
Safety data were reported by 16 of 54 RCTs (30%) and, of these, 9 (56%) reported no adverse events. Among the 7 RCTs that reported the occurrence of adverse events, 8 serious events were reported, namely suicidal ideation (2 patients, 1 in-person and 1 in remote CBT), hospitalization for a panic attack (1 patient, in-person CBT), victim of domestic violence (1 patient, remote CBT), death after emergency heart surgery (1 patient, in-person CBT), and overdose with acetaminophen (1 patient, remote CBT). One trial reported 2 serious adverse events unrelated to study participation without further details. No differences in serious or non-serious adverse events (e.g., increased anxiety) between in-person and therapist-guided remote CBT were observed (Appendix 1, eTable 1).
Risk of biasPatients and health care providers were unblinded in all RCTs and no study was at high risk of bias for deviation from the intended intervention; however, 5 studies (9%) were at high risk of bias for their randomization process, 10 studies (19%) for missing outcome data, and 9 studies (17%) for measurement of the outcome (e.g., study personnel were aware of intervention received by participants, the participant may have been influenced by knowledge of the intervention for patient-reported incomes) (Appendix 1, eTable 4). We found study protocols for 29 (54%) RCTs, (Appendix 1, eTable 5); 5 of 29 were at high risk of bias for selection of their reported results (Appendix 1, eTable 4).
Effect of in-person versus remote CBT on primary outcomesModerate-certainty evidence from 51 RCTs (5384 patients) showed little to no difference in effectiveness between in-person and therapist-guided remote CBT on primary outcomes (SMD −0.02, 95% CI −0.11 to 0.07) (Figure 3, Table 2; Appendix 1, eTable 6). We did not find evidence of small-study effects (Appendix 1, eFigure 3). Analysis using end scores also showed little to no difference in effectiveness between in-person and remote CBT (SMD −0.01, 95% CI −0.11 to 0.08) (Appendix 1, eFigure 4).
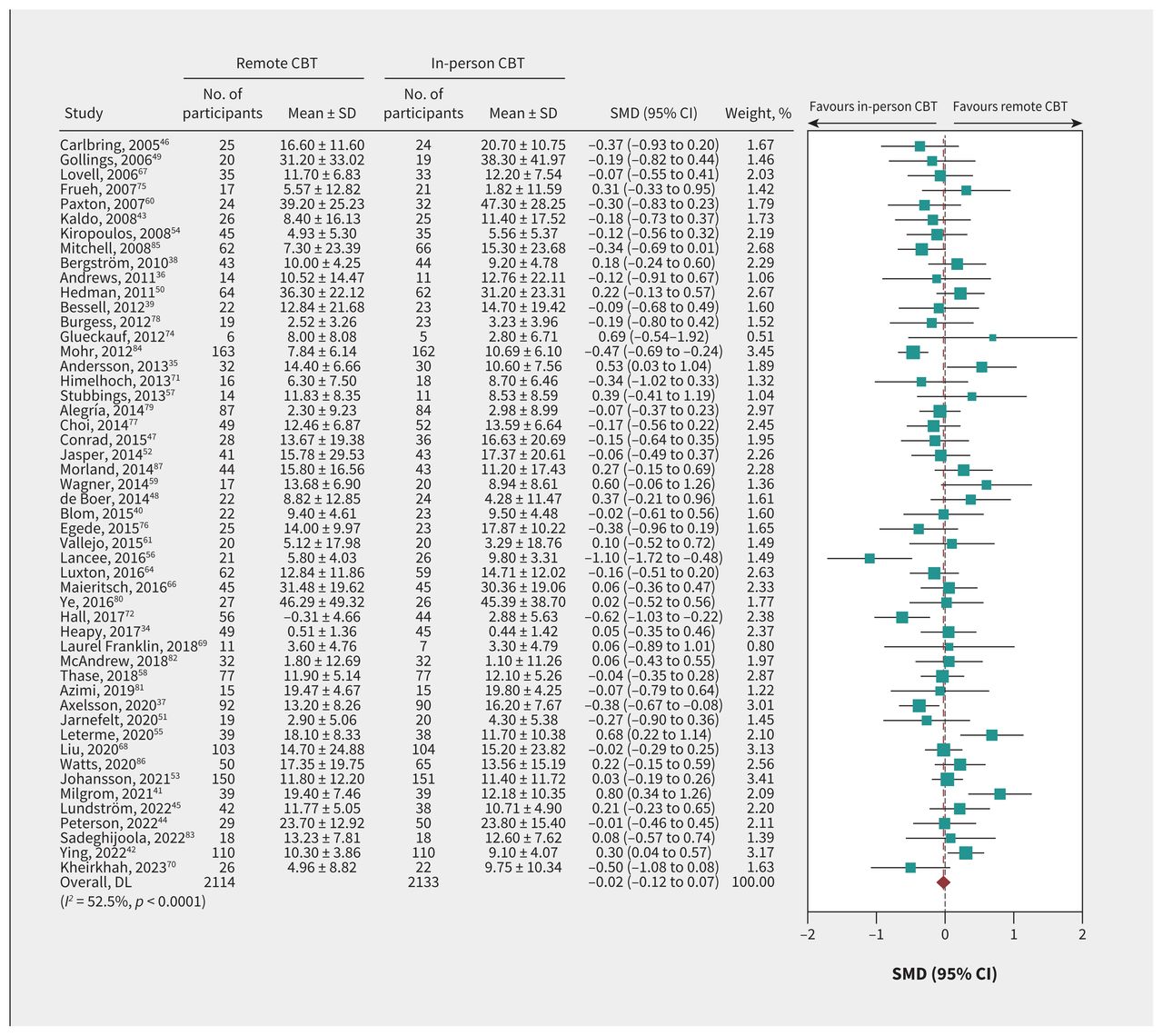 Figure 3:
Figure 3: Effect of remote versus in-person cognitive behavioural therapy (CBT) on patient compliance. Weights are from random-effects model; continuity correction applied to studies with 0 cells. Note: CI = confidence interval, DL = DerSimonian–Laird, SD = standard deviation, SMD = standardized mean difference.
Table 2:Grading of Recommendations, Assessment, Development and Evaluation (GRADE) evidence profile of in-person versus therapist-guided remote cognitive behavioural therapy (CBT) on primary outcomes reported in randomized controlled trials (RCTs) involving patients with psychological and somatic complaints
We found no credible subgroup effects based on clinical condition, (Appendix 1, eFigure 5 and eTable 3) individual or group therapy (Appendix 1, eFigure 6 and eTable 3), or risk of bias (Appendix 1, eFigures 7–11 and eTable 3). Meta-regression showed no significant association between length of follow-up and the difference in treatment effect between in-person and therapist-guided remote CBT (Appendix 1, eFigures 12–13 and eTable 3).
Three RCTs did not contribute to our meta-analysis because they did not report a patient-important outcome or reported data that were not possible to pool. One evaluated patient and provider perceptions of different forms of CBT for insomnia and found similar satisfaction with telemedicine and in-person delivery. 73 The second reported health services use and associated expenditures among caregivers with depressive symptoms who provided care for patients with dementia, and found no difference between in-person and telephone-based CBT.65 The third enrolled patients with panic disorder and reported a 3-way repeated-measures analysis of variance that found no difference in outcomes between in-person or therapist-supported, computer-delivered CBT.63
Sensitivity analysisWhen restricted to RCTs exploring the effectiveness of in-person and therapist-guided remote CBT for depression, the meta-analysis showed no difference in effect on the 63-point BDI-II (weighted mean difference 0.00, 95% CI −1.75 to 1.75) (Appendix 1, eFigure 14).
InterpretationOur systematic review found moderate-certainty evidence of little to no difference in effectiveness in CBT delivered either in person or remotely with therapist support. This finding was unaffected by type of clinical condition, length of follow-up, or whether CBT was provided individually or through group sessions.
Our findings update previous meta-analyses that compared in-person and remote CBT and concluded the need for additional research.10,14,88–92 The most recent review included 20 RCTs that compared Internet-delivered CBT with face-to-face CBT and concluded that both appeared similarly effective; however, the authors did not assess the overall certainty of evidence or the credibility of their subgroup analysis based on risk of bias.14 They suggested that effectiveness may differ based on clinical condition, length of follow-up, and whether CBT was provided individually or in groups.14 This review restricted the search to English-language RCTs and to a single electronic database, and included 6 RCTs that our experts concluded were not eligible for our review because the remote CBT was not guided by a therapist, 93,94 the intervention was not conventional CBT,95 the in-person and remote CBT were not similar in content,96,97 or the couple therapy intervention that was described as traditional sexual counselling was not comparable to standard individual- or group-delivered CBT.98 We addressed the methodologic limitations of this review and identified 40 additional RCTs that had not been included.
To address previous limitations in the evidence, we conducted a comprehensive search for eligible RCTs in any language and engaged clinical experts, blinded to treatment results, to assess the descriptions of all interventions to confirm eligibility. We used the GRADE approach to appraise the certainty of evidence, used predefined subgroup analyses to explore sources of heterogeneity, and assessed the credibility of all potential subgroup effects. Further, although RCTs eligible for our review provided the same intervention administered in person or remotely, we rated down our certainty of evidence for unblinding. This is a conservative approach as several studies have found that most patients are willing to receive psychotherapy in either format,99–101 and we found no evidence for differential compliance depending on whether CBT was provided in person or remotely, which we would anticipate if patients held strong preferences.
Cognitive behavioural therapy is effective for the treatment of several mental health disorders and somatic complaints;1–4 however, resource requirements are a barrier to in-person therapy. Our review provides moderate-certainty evidence that remote delivery of CBT with therapist guidance is probably similarly effective to in-person delivery. Remote CBT imposes fewer demands on patients’ time as travel for face-to-face sessions is unnecessary.102 Remote CBT may also be more cost-effective than in-person delivery, particularly when the intervention is supported by therapists, rather than being delivered remotely in real time.103–105
Our finding that remote CBT is an effective alternative to in-person delivery has potential policy implications. Only 2 Canadian provinces (Saskatchewan and Ontario) currently provide funding for remote CBT.12,13 Access to psychotherapy is an important barrier for many people in Canada, particularly those living in remote or rural areas, including military veterans and Indigenous populations, both of which are at high risk for chronic pain and mental health disorders.106–108
An August 2023 poll of 3189 adults in Canada, commissioned by Mental Health Research Canada, found that the proportion of participants who reported an inability to pay as a reason for not accessing mental health care had increased from 18% to 29% over the previous year.109 Canada’s provinces and territories should consider funding access to therapist-guided remote CBT to facilitate greater access to evidence-based care.
Several options for providing remote psychotherapy are available and use of this delivery method for CBT is likely to evolve rapidly. Recent advances in artificial intelligence tools may open further avenues for providing CBT with reduced involvement of human therapists. 110 Future studies should explore whether certain patients have strong preferences for in-person or therapist-guided remote CBT, the comparative effectiveness of different types of remote CBT (e.g., high or low involvement of therapist delivering CBT remotely v. in person), and the effectiveness of remote CBT compared with stepped care, whereby remote CBT is provided first, and then non-responders are offered in-person CBT.
LimitationsAlthough studies eligible for our review involved patients presenting with a wide range of clinical conditions, many conditions that are candidates for CBT were not represented in any studies or in only a single RCT (e.g., alcohol use disorder). Patients enrolled in RCTs eligible for review consented to be randomized to either in-person or remote CBT and likely were not people with strong preferences for 1 method of delivery over the other. Eligible RCTs were conducted in high-income countries, largely enrolled middle-aged participants, and followed patients for a median of 180 days. The generalizability of our findings to lower-income countries, older patients (who may be less comfortable with technology), and longer follow-up periods is uncertain.
Although we found no important difference in patient compliance between in-person and remote CBT, substantial unexplained heterogeneity was associated with the overall pooled estimate. We did not find evidence for differences in treatment effect based on clinical condition, but the small number of RCTs contributing to some subgroups may have obscured important subgroup effects. Finally, we pooled studies across a variety of outcome measures as the SMD, which limits interpretability and may be affected by baseline heterogeneity of participants.111 However, we did pool effects on RCTs of depression to demonstrate results in natural units for this condition and found no difference.
ConclusionIn this systematic review and meta-analysis of RCTs, moderate-certainty evidence found little to no difference in effectiveness between in-person and therapist-guided, remotely delivered CBT for a variety of mental health disorders and somatic conditions. Our findings suggest that therapist-guided remote CBT can be used to facilitate greater access to evidence-based care.
FootnotesCompeting interests: Behnam Sadeghirad reports funding from the Canadian Institutes of Health Research, the Michael G. DeGroote Institute for Pain Research and Care, and the Chronic Pain Centre of Excellence for Canadian Veterans. No other competing interests were declared.
This article has been peer reviewed.
Contributors: Jason Busse conceived and designed the study. Sara Zandieh, Maryam Abdollahzadeh, Liam Yao, Briar Inness, Annaya Pathak, Rachel Couban, Holly Crandon, and Kian Torabiardakani acquired the data. Sara Zandieh and Behnam Sadeghirad carried out the statistical analysis. Sara Zandieh, Behnam Sadeghirad, Li Wang, Randi McCabe, Peter Beiling, and Jason Busse interpreted the data. Sara Zandieh and Jason Busse drafted the manuscript. All of the authors revised the manuscript and contributed important intellectual content, gave final approval of the version to be published, and agreed to be accountable for all aspects of the work.
Funding: Jason Busse is supported, in part, by a Canadian Institutes of Health Research Canada Research Chair in the prevention and management of chronic pain.
Data sharing: The relevant data in this study are available from Sara Zandieh (zandiehsmcmaster.ca)
Accepted January 29, 2024.This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
留言 (0)