
記住我


See Article, page 728
So, what really is more dangerous: anemia or transfusion? This thought-provoking question was raised over 10 years ago by Shander et al,1 and is just as relevant today as it was back then. Red cell transfusions are independently associated with a wide range of unfavorable outcomes.2 Preoperative anemia is also independently associated with a wide range of unfavorable outcomes.3 In addition, the 2 are highly intertwined, with patients admitted with preoperative anemia up to 4 times more likely to receive a red cell transfusion when compared to patients not anemic, and some data demonstrating the 2 are synergistic, having an additive effect on outcomes.4,5
In attempts to better understand which is worse, researchers have applied a variety of statistical methods, including multivariable regression models (with preoperative anemia and red cell transfusion included as variables), propensity score matching, and linear mixed effect models, while accounting for confounding and interactions (effect modification).
The research by Warner et al6 published in this journal attempts to tease out the answer to this important question in the cardiac surgery setting. They wanted to know how much of the association of preoperative anemia and adverse outcomes is mediated through intraoperative red cell transfusion in cardiac surgery patients. To do this, they applied a statistical technique known as mediation analysis.
WHAT IS MEDIATION ANALYSIS?Mediation analysis is a commonly used statistical technique applied to medical research. Mediation analysis is used to study whether the relationship between an exposure (independent variable) and outcome (dependent variable) is to some extent explained by another factor (mediator). For example, in their study, Warner et al6 investigated whether preoperative anemia’s (independent variable) relationship with outcomes (dependent variable) was mediated through intraoperative red cell transfusion (mediator), after adjusting for potential confounders.
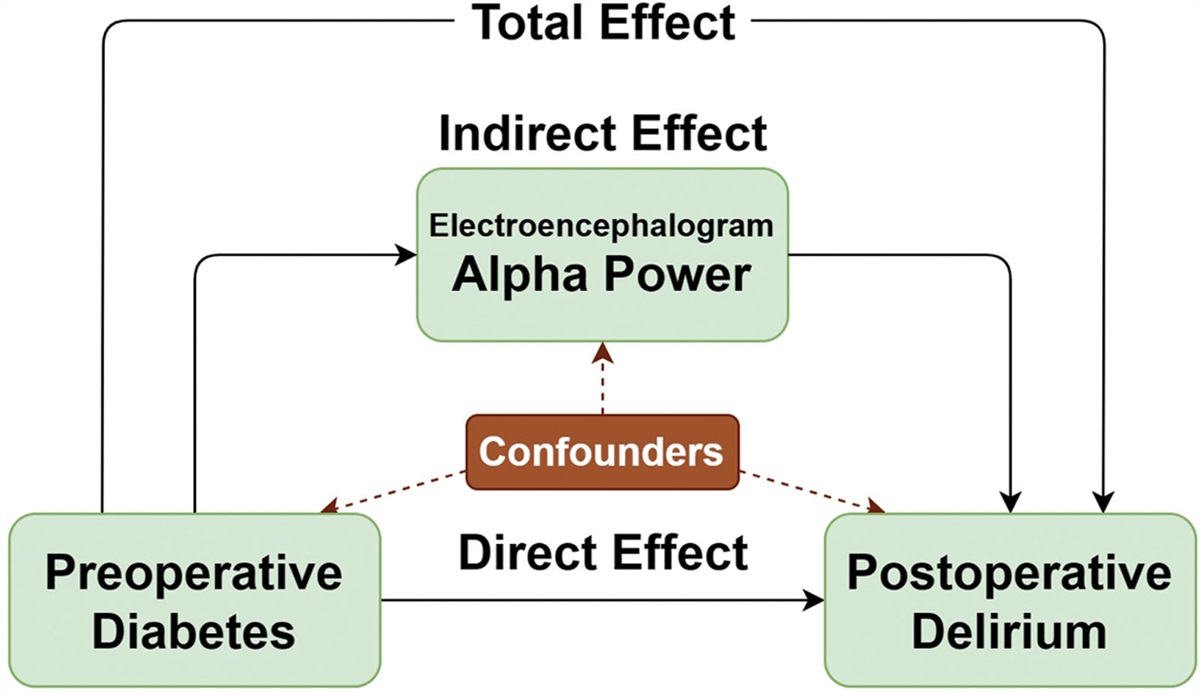
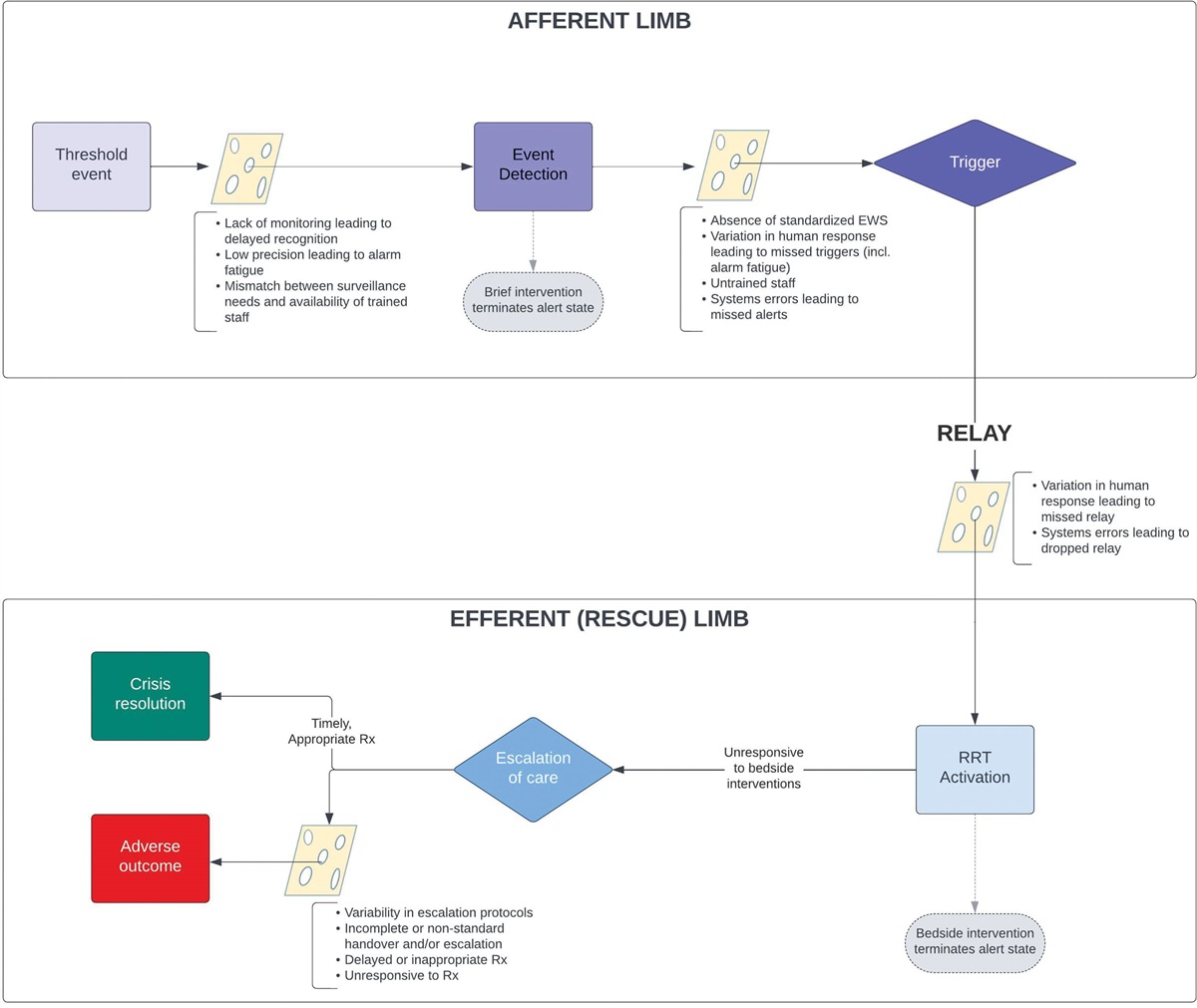
Continuing the example used by the study authors, to successfully perform a mediation analysis, we apply the following steps: (1) investigate if there is a relationship between anemia and outcomes; (2) assess whether there is a relationship between anemia and transfusion; (3) check if there is a relationship between transfusion and outcomes (Figure). If we find anemia has an impact on both transfusion and outcome, and transfusion also has an impact on outcome, we may conclude that transfusion is playing a role in the relationship between anemia and outcomes. In other words, the relationship between anemia and outcomes is mediated through transfusion.
 Figure.:
Figure.: Mediation analysis model applied to assess red cell transfusion’s role in mediating the relationship between preoperative anemia and outcome.
An essential detail when applying mediation analysis is the sequence of events and the timing of the relationships (temporality). In this specific example, it means the preoperative anemia must precede the intraoperative red cell transfusion. In turn, the intraoperative red cell transfusion must precede the outcome. This is referred to as the mediation pathway and is the reason why the study authors excluded postoperative red cell transfusions from the analysis.
HOW DOES MEDIATION ANALYSIS DIFFER FROM EFFECT MODIFICATION?The difference between mediation analysis and effect modification may appear subtle; however, their primary aim is different. Mediation analysis aims to understand if and to what extent a mediator is explaining the relationship between the exposure and outcome. In very simple terms, it can be used to investigate questions like, “Why is preoperative anemia associated with adverse outcomes, and is the relationship explained by intraoperative transfusion?” In contrast, effect modification can be applied to investigate if and how the relationship between the exposure and outcome changes based on the presence of a third variable—in other words, how the exposure and a third variable interact with each other. In very simple terms, it can be applied to investigate how much the relationship between red blood cell transfusion and the outcome differs across different levels of nadir hemoglobin.7,8
IS MEDIATION ANALYSIS COMMONLY USED?Although mediation analysis is common in the medical literature, it is not frequently applied to patient blood management–related research.9 To our knowledge, this is the first example where it has been applied to patient blood management research in the cardiac surgery setting. The authors are to be applauded for their efforts.
WHAT DID THE MEDIATION ANALYSIS REVEAL?The authors analyzed over 4000 adults admitted for coronary artery bypass grafting or valve surgery on cardiopulmonary bypass over a 10-year period. Many of the findings were consistent with what is commonly reported in the medical literature. For example, 30% of patients in their cohort had preoperative anemia,10 and both preoperative anemia and intraoperative red cell transfusion were associated with each other and with adverse postoperative outcomes.4,11
The results of their mediation analysis suggest something interesting: the role preoperative anemia plays in postcardiac surgery outcomes is likely to differ depending on the outcome. The authors found the relationship between preoperative anemia and postoperative acute kidney injury was mainly due to the direct effects of preoperative anemia (P < .001) rather than being mediated through intraoperative red cell transfusion (P = .22).6 A note of caution: the finding that anemia and acute kidney injury were not mediated through intraoperative transfusion does not imply transfusing anemic patients intraoperatively is the solution.
For example, in contrast to preoperative anemia’s relationship with acute kidney injury, the authors report that a significant proportion of its relationship with increased length of stay was mediated through intraoperative red cell transfusion (38%; 95% confidence interval, 22%–62%; P < .001).6 Furthermore, there are some important limitations that need to be considered before jumping to conclusions.
WHAT WERE SOME OF THE LIMITATIONS?Among the limitations discussed by the study authors, 1 significant limitation is the exclusion of postoperative red cell transfusions. The reason for the decision to exclude is valid, given the authors could not determine whether the postoperative transfusion occurred after the postoperative acute kidney injury. Nonetheless, this remains a significant limitation and should not be ignored. Most red cell transfusions in the cardiac surgery setting occur postoperatively. The results of 1 clinical trial demonstrated as many as 75% of all red cell units were transfused following surgery.12,13 Given that the research by Warner et al6 and others4 indicates there is an independent relationship between red cell transfusion and acute kidney injury, any interpretation of the results will need to carefully consider this important detail.
CONCLUSIONSSo, what really is more dangerous: preoperative anemia or transfusion in cardiac surgery patients? This research suggests that the answer is the same as the answer to many other questions: “It depends.” That is, it may depend on what outcome is being investigated. Whatever the case, whether preoperative anemia is worse than red cell transfusion or red cell transfusion is worse than anemia, the take-home message from 10 years ago is just as relevant today: “Anemia should never be regarded as an innocent bystander.”1 Patients at risk of preoperative or postoperative anemia should be screened as early as possible, and, where possible, the cause should be identified and managed appropriately.
DISCLOSURESName: Kevin M. Trentino, PhD.
Contribution: This author was invited to submit the editorial, conceived the work, and designed, developed, and refined the manuscript with contributions from all authors. This author also drafted the manuscript, critically revised the draft, and approved the final version to be published.
Name: Kevin Murray, PhD.
Contribution: This author was invited to submit the editorial, conceived the work, and designed, developed, and refined the manuscript. This author also critically revised the draft and approved the final version to be published.
Name: Aryeh Shander, MD.
Contribution: This author was invited to submit the editorial, conceived the work, and designed, developed, and refined the manuscript. This author also critically revised the draft and approved the final version to be published.
This manuscript was handled by: Shannon L. Farmer, DHSc.
REFERENCES 1. Shander A, Javidroozi M, Ozawa S, Hare GM. What is really dangerous: anaemia or transfusion? Br J Anaesth. 2011;107(suppl 1):i41–i59. 2. Hopewell S, Omar O, Hyde C, Yu LM, Doree C, Murphy MF. A systematic review of the effect of red blood cell transfusion on mortality: evidence from large-scale observational studies published between 2006 and 2010. BMJ Open. 2013;3:e002154. 3. Fowler AJ, Ahmad T, Phull MK, Allard S, Gillies MA, Pearse RM. Meta-analysis of the association between preoperative anaemia and mortality after surgery. Br J Surg. 2015;102:1314–1324. 4. LaPar DJ, Hawkins RB, McMurry TL, et al.; Investigators for the Virginia Cardiac Services Quality Initiative. Preoperative anemia versus blood transfusion: which is the culprit for worse outcomes in cardiac surgery? J Thorac Cardiovasc Surg. 2018;156:66–74.e2. 5. von Heymann C, Kaufner L, Sander M, et al. Does the severity of preoperative anemia or blood transfusion have a stronger impact on long-term survival after cardiac surgery? J Thorac Cardiovasc Surg. 2016;152:1412–1420. 6. Warner MA, Hanson AC, Shulte PJ, et al. Preoperative anemia & postoperative outcomes in cardiac surgery: a mediation analysis evaluating intraoperative transfusion exposures. Anesth Analg. 2024;138:728–737. 7. Kougias P, Orcutt S, Pak T, et al. Impact of postoperative nadir hemoglobin and blood transfusion on outcomes after operations for atherosclerotic vascular disease. J Vasc Surg. 2013;57:1331–1337. 8. Trentino KM, Leahy MF, Sanfilippo FM, et al. Associations of nadir haemoglobin level and red blood cell transfusion with mortality and length of stay in surgical specialties: a retrospective cohort study. Anaesthesia. 2019;74:726–734. 9. Saager L, Turan A, Reynolds LF, Dalton JE, Mascha EJ, Kurz A. The association between preoperative anemia and 30-day mortality and morbidity in noncardiac surgical patients. Anesth Analg. 2013;117:909–915. 10. Gomez-Ramirez S, Jerico C, Munoz M. Perioperative anemia: prevalence, consequences and pathophysiology. Transfus Apher Sci. 2019;58:369–374. 11. Karkouti K, Grocott HP, Hall R, et al. Interrelationship of preoperative anemia, intraoperative anemia, and red blood cell transfusion as potentially modifiable risk factors for acute kidney injury in cardiac surgery: a historical multicentre cohort study. Can J Anaesth. 2015;62:377–384. 12. Stokes EA, Wordsworth S, Bargo D, et al.; TITRe2 Investigators. Are lower levels of red blood cell transfusion more cost-effective than liberal levels after cardiac surgery? Findings from the TITRe2 randomised controlled trial. BMJ Open. 2016;6:e011311. 13. Murphy GJ, Pike K, Rogers CA, et al.; TITRe2 Investigators. Liberal or restrictive transfusion after cardiac surgery. N Engl J Med. 2015;372:997–1008.
留言 (0)