
記住我
Glutamate decarboxylase 2 (GAD2), also termed GAD65, is 1 out of 2 glutamate decarboxylases that are required for the decarboxylation of glutamate to gamma-aminobutyric acid (GABA).1 GABA is the most important inhibitory neurotransmitter in the central nervous system where it reduces neuronal excitability at nerve terminals and synapses (summarized in the study by Lee et al2). In the pancreas, GAD2 plays a role in insulin-producing β cells of pancreatic islets.3 GAD2 alterations play a critical role in several disease types. Downregulation of cerebral GAD2 expression has, for example, been described in autism4 and Alzheimer disease.5 GAD2 autoantibodies are found in up to 80% of patients with type 1 diabetes and have therefore been considered a possible cause of this disease.6 GAD2 autoantibodies are also associated with several rare neurological disorders, such as stiff-person syndrome, cerebellar ataxia, epilepsy, and limbic encephalitis (summarized in the study by Tsiortou et al7).
According to RNA expression data, GAD2 expression is strictly limited to the brain and the pancreas (https://www.proteinatlas.org/ENSG00000136750-GAD2/summary/rna8–11). GAD2 immunohistochemistry (IHC) might therefore be of use for identifying tumors originating from the pancreas. Only a few authors have examined GAD2 expression in cancer and proposed a role for tumor progression in gastric and gallbladder cancer. Song et al12 reported a significantly higher GAD65 expression in 313 gastric cancers than in 60 adjacent nontumor tissues and found a link between high expression and the depth of tumor invasion, high TNM stage, and poor prognosis. For gallbladder adenocarcinoma, Deng and Pei13 found increased levels of GAD65 immunostaining as compared with peritumoral tissues and a significant link between high GAD65 expression and reduced patient survival. Other cancer entities have so far not been systematically analyzed for GAD2 protein expression, but Huang et al14 described GAD2 protein expression in 1 out of 3 cancers in patients with GAD2 autoantibodies and associated neurological disorders.
To comprehensively determine the prevalence of GAD2 protein expression in cancer and to assess the potential diagnostic utility of GAD2 IHC, we analyzed a pre-existing set of tissue microarrays (TMA) containing more than 19,000 tumor tissue samples from 152 different tumor types and subtypes as well as 76 non-neoplastic tissue categories for GAD2 expression by IHC in this study.
MATERIALS AND METHODS Patient SamplesTwo types of TMAs were included in our study. Our normal TMA was composed of 8 samples from 8 different donors from each of 76 different normal tissue types (608 samples on 1 slide). The tumor TMAs included a total of 19,202 primary tumors from 152 different tumor types and subtypes. The composition of normal and tumor TMAs is described in the Results section. All samples were from the archives of the Institutes of Pathology, University Hospital of Hamburg, Germany, the Institute of Pathology, Clinical Center Osnabrueck, Germany, and the Department of Pathology, Academic Hospital Fuerth, Germany. Tissues were fixed in 4% buffered formalin and then embedded in paraffin. The TMA manufacturing process was described earlier in detail.15,16 In brief, tissue spots (diameter: 0.6 mm) were transmitted from tumor-containing donor blocks to empty recipient paraffin blocks. Immunohistochemical data on progesterone receptor (PR) expression were available from a previous study.17 Conventional whole sections were taken from liver metastases of 15 cases of pancreatic neuroendocrine tumors (NETs) for the purpose of data validation. The use of archived remnants of diagnostic tissues for TMA manufacturing, their analysis for research purposes, and the use of patient data were according to local laws (HmbKHG, §12), and the analysis had been approved by the local ethics committee (Ethics Commission Hamburg, WF-049/09). All work has been carried out in compliance with the Helsinki Declaration.
ImmunohistochemistryFreshly prepared TMA sections were immunostained on one day in one experiment. Slides were deparaffinized with xylol, rehydrated through a graded alcohol series and exposed to heat-induced antigen retrieval for 5 minutes in an autoclave at 121°C in pH 9.0 DakoTarget Retrieval Solution (Agilent; #S2367). Endogenous peroxidase activity was blocked with Dako Peroxidase Blocking Solution (Agilent; #52023) for 10 minutes. Primary antibody specific for GAD2 (mouse monoclonal, MSVA-602M, MS Validated Antibodies, GmbH; #4975-602M) was applied at 37°C for 60 minutes at a dilution of 1:150. Only the TMA slides containing pancreatic neuroendocrine neoplasms were also stained by antibodies against insulin (recombinant rabbit monoclonal, HMV-308, MS Validated Antibodies, GmbH; cat#6515-308, dilution 1:150), glucagon (polyclonal rabbit, BioGenex, San Ramon; PU039-UP ) dilution 1:150, c-peptide (recombinant rabbit monoclonal, HMV-363, MS Validated Antibodies, GmbH; cat#6402-363, dilution 1:150), and pancreatic polypeptide (Abcam #ab272732, clone EPR-23320-10, dilution 1:450). For the purpose of antibody validation, the normal tissue TMA and the subset of our tumors were also analyzed by the rabbit monoclonal GAD2 antibody EPR22952-70 (cat. # ab239372, Abcam) at a dilution of 1:50,000 and an otherwise identical protocol. For the purpose of data validation, EPR22952-70 was also applied to 4 TMA sections containing 19 of our 29 tumors that had shown an unexpected GAD2 staining. Bound antibody was visualized using the EnVision Kit (Agilent; #K5007) according to the manufacturer’s directions. The sections were counterstained with hemalaun. For tumor tissues, the percentage of positive neoplastic cells was estimated, and the staining intensity was semiquantitatively recorded (0, 1+, 2+, 3+). For statistical analyses, the staining results were categorized into 4 groups. Tumors without any staining were considered negative. Tumors with 1+ staining intensity in ≤70% of tumor cells and 2+ intensity in ≤30% of tumor cells were considered weakly positive. Tumors with 1+ staining intensity in >70% of tumor cells, 2+ intensity in 31% to 70%, or 3+ intensity in ≤30% of tumor cells were regarded moderately positive. Tumors with 2+ intensity in >70% or 3+ intensity in >30% of tumor cells were considered strongly positive.
StatisticsSensitivity and specificity for the detection of pancreatic neuroendocrine neoplasia and lung neuroendocrine neoplasia were calculated according to the following formulas: sensitivity = number of true positives divided by the number of true positives plus number of false negatives; specificity = number of true negatives divided by the number of true negatives plus number of false positives. The positive predictive value (PPV) was calculated using the formula PPV = (sensitivity × prevalence)/(sensitivity × prevalence + [1-specificity] × [1-prevalence]).
RESULTS Technical IssuesA total of 17,507 (91.2%) of 19,202 tumor samples were interpretable in our tumor TMA analysis. Noninterpretable samples demonstrated a lack of unequivocal tumor cells or lack of the entire tissue spot. Sufficient numbers of samples (≥4) of each normal tissue type were evaluable.
GAD2 in Normal TissueA strong cytoplasmic GAD2 staining was seen in a large subset of cells of islets of Langerhans in the pancreas. A strong GAD2 staining also occurred in nerve fibers of the cerebrum and the cerebellum. All these findings were obtained by using the monoclonal mouse antibody MSVA-602M and the rabbit monoclonal antibody EPR22952-70 and therefore considered to be specific. Using MSVA-602M, GAD2 immunostaining was not seen in any other normal tissues including squamous epithelium, sebaceous glands, gastrointestinal epithelium, Brunner glands, gallbladder, exocrine pancreas, salivary glands, breast, endocervical glands, endometrium, fallopian tube, ovary, placenta, chorion cells, amnion cells, respiratory epithelium, lung, kidney, urothelium, prostate, seminal vesicles, testis, epididymis, thyroid (including C-cells), parathyroid, hypophysis, and the brain. There was, however, a staining of pigments (probably lipofuscin) in several organs including heart, adrenal gland, and the liver. Representative images of normal tissues are shown in Figure 1. EPR22952-70 did not show any pigment staining but resulted in significant nuclear staining in a broad range of different tissues. Pigment staining by MSVA-602M and nuclear staining by EPR22952-70 were considered antibody-specific cross-reactivities (Supplementary Fig. 1, Supplemental Digital Content 1, https://links.lww.com/PAS/B757).
 FIGURE 1:
FIGURE 1: Glutamate decarboxylase 2 (GAD2) immunostaining of normal tissues. The panels show a strong fibrillar GAD2 staining of the gray matter of the cerebrum (while cell bodies of neurons are GAD2 negative; A) and a strong cytoplasmic GAD2 staining of pancreatic islet cells (B). GAD2 also labels pigment (probably lipofuscin) in samples of normal liver (C), adrenal gland (D), and the heart (E). GAD2 immunostaining is absent in colorectal epithelium (F).
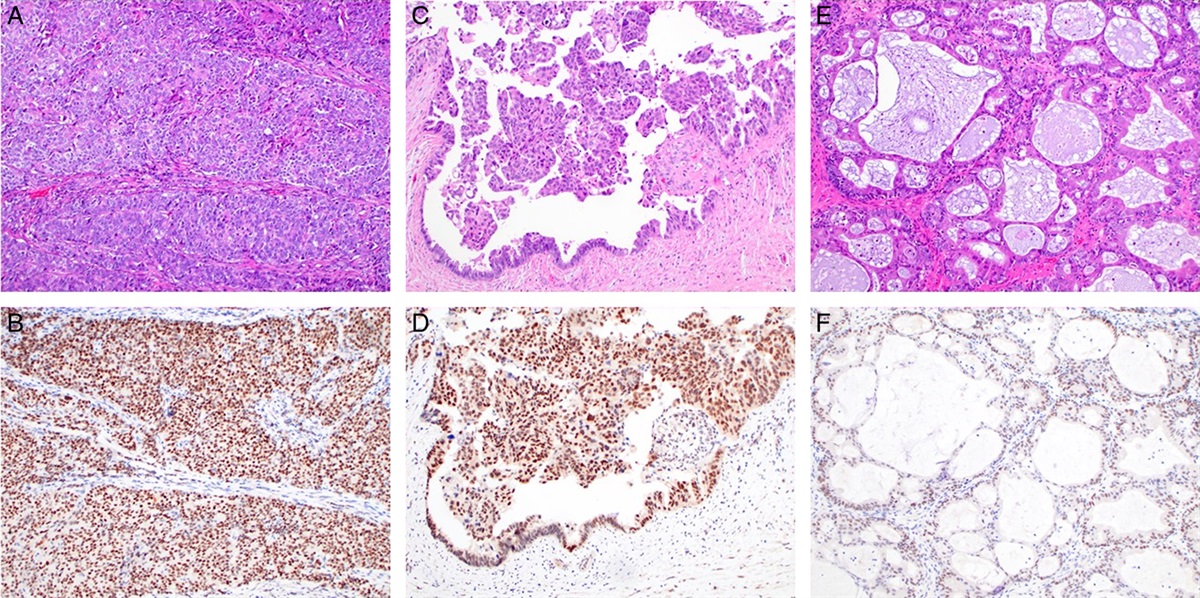
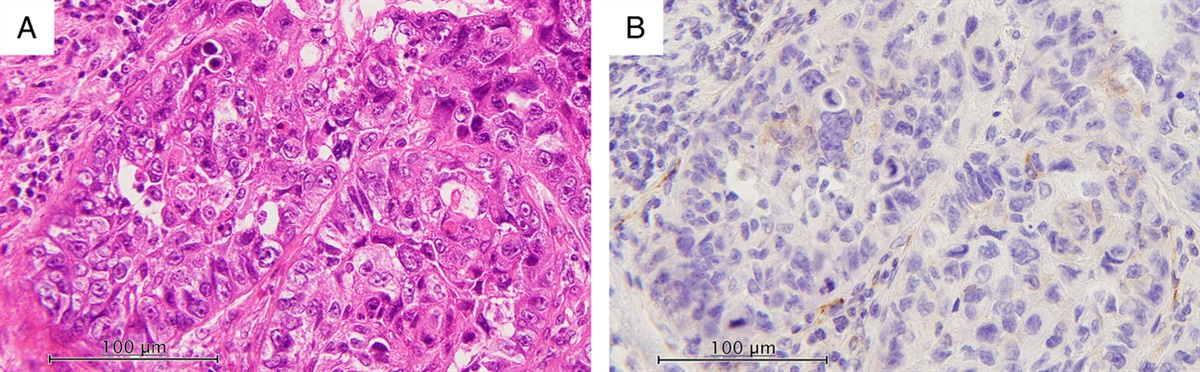
GAD2 in CancerGAD2 immunostaining in tumors was always cytoplasmic. It was detectable in 114 (0.7%) of the 17,507 analyzable tumors, including 54 (0.3%) with weak, 29 (0.2%) with moderate, and 31 (0.2%) with strong immunostaining. Overall, 20 (13%) of 152 tumor categories showed detectable GAD2 expression, with 5 (3.3%) tumor categories including at least 1 case with strong positivity (Table 1). Representative images of GAD2-positive tumors are shown in Figure 2. GAD2 immunostaining was most commonly seen in neuroendocrine carcinomas (NECs) (58.3% of 12) and NETs (63.2% of 87) of the pancreas, followed by granular cell tumors (37.0%) and NETs of the lung (11.1%). GAD2 was only occasionally (<10% of cases) seen in 16 other tumor entities including paraganglioma, medullary thyroid carcinoma, ganglioneuroma, small cell NEC of the bladder, Ewing sarcoma, pancreatic/ampullary adenocarcinoma, ductal adenocarcinoma of the pancreas, gallbladder adenocarcinoma, gastric adenocarcinoma, adenocarcinoma of the prostate, serous carcinoma of the ovary, follicular thyroid carcinoma, anaplastic thyroid carcinoma, adrenal cortical adenoma, squamous cell carcinoma of the vulva, and Warthin tumor of the parotid gland. A graphical representation of a ranking order of GAD2-positive and strongly positive tumors is given in Fig. 3. For all 19 cases from tumor types with only occasional GAD2 positivity, the findings were confirmed by the rabbit monoclonal antibody EPR22952-70 (Supplementary Fig. 2, Supplemental Digital Content 2, https://links.lww.com/PAS/B758). These tumors included follicular thyroid carcinoma (n=1), medullary thyroid carcinoma (n=8), anaplastic thyroid carcinoma (n=1), pancreatic ampullary adenocarcinoma (n=2), ductal adenocarcinoma of the pancreas (n=2), paraganglioma (n=4), and ganglioneuroma (n=1). Whole-section analysis of liver metastases from pancreatic NETs revealed positive GAD2 staining in 10 of 15 cases (66.7%). Examples are shown in Supplementary Fig. 3, Supplemental Digital Content 3, https://links.lww.com/PAS/B759.
TABLE 1 - GAD2 Immunostaining in Human Tumors GAD2 immunostaining Tumor entity On TMA (n) Analyzable (n) Negative (%) Weak (%) Moderate (%) Strong (%) Tumors of the skin Pilomatricoma 35 28 100.0 0.0 0.0 0.0 Basal cell carcinoma of the skin 89 81 100.0 0.0 0.0 0.0 Benign nevus 29 27 100.0 0.0 0.0 0.0 Squamous cell carcinoma of the skin 145 129 100.0 0.0 0.0 0.0 Malignant melanoma 65 61 100.0 0.0 0.0 0.0 Malignant melanoma lymph node metastasis 86 73 100.0 0.0 0.0 0.0 Merkel cell carcinoma 48 38 100.0 0.0 0.0 0.0 Tumors of the head and neck Squamous cell carcinoma of the larynx 109 97 100.0 0.0 0.0 0.0 Squamous cell carcinoma of the pharynx 60 50 100.0 0.0 0.0 0.0 Oral squamous cell carcinoma (floor of the mouth) 130 115 100.0 0.0 0.0 0.0 Pleomorphic adenoma of the parotid gland 50 44 100.0 0.0 0.0 0.0 Warthin tumor of the parotid gland 104 100 99.0 1.0 0.0 0.0 Adenocarcinoma, NOS (papillary cystadenocarcinoma) 14 12 100.0 0.0 0.0 0.0 Salivary duct carcinoma 15 12 100.0 0.0 0.0 0.0 Acinic cell carcinoma of the salivary gland 181 149 100.0 0.0 0.0 0.0 Adenocarcinoma NOS of the salivary gland 109 95 100.0 0.0 0.0 0.0 Adenoid cystic carcinoma of the salivary gland 180 140 100.0 0.0 0.0 0.0 Basal cell adenocarcinoma of the salivary gland 25 23 100.0 0.0 0.0 0.0 Basal cell adenoma of the salivary gland 101 88 100.0 0.0 0.0 0.0 Epithelial-myoepithelial carcinoma of the salivary gland 53 52 100.0 0.0 0.0 0.0 Mucoepidermoid carcinoma of the salivary gland 343 299 100.0 0.0 0.0 0.0 Myoepithelial carcinoma of the salivary gland 21 20 100.0 0.0 0.0 0.0 Myoepithelioma of the salivary gland 11 9 100.0 0.0 0.0 0.0 Oncocytic carcinoma of the salivary gland 12 12 100.0 0.0 0.0 0.0 Polymorphous adenocarcinoma, low grade of the salivary gland 41 36 100.0 0.0 0.0 0.0 Pleomorphic adenoma of the salivary gland 53 38 100.0 0.0 0.0 0.0 Tumors of the lung, pleura, and thymus Adenocarcinoma of the lung 196 190 100.0 0.0 0.0 0.0 Squamous cell carcinoma of the lung 80 73 100.0 0.0 0.0 0.0 Small cell carcinoma of the lung 16 15 100.0 0.0 0.0 0.0 Mesothelioma, epithelioid 40 36 100.0 0.0 0.0 0.0 Mesothelioma, biphasic 77 67 100.0 0.0 0.0 0.0 Thymoma 29 28 100.0 0.0 0.0 0.0 Lung, neuroendocrine tumor (NET) 29 27 88.9 11.1 0.0 0.0 Tumors of the female genital tract Squamous cell carcinoma of the vagina 78 64 100.0 0.0 0.0 0.0 Squamous cell carcinoma of the vulva 157 144 99.3 0.7 0.0 0.0 Squamous cell carcinoma of the cervix 136 127 100.0 0.0 0.0 0.0 Adenocarcinoma of the cervix 23 22 100.0 0.0 0.0 0.0 Endometrioid endometrial carcinoma 338 297 100.0 0.0 0.0 0.0 Endometrial serous carcinoma 86 64 100.0 0.0 0.0 0.0 Carcinosarcoma of the uterus 57 52 100.0 0.0 0.0 0.0 Endometrial carcinoma, high grade, G3 13 10 100.0 0.0 0.0 0.0 Endometrial clear cell carcinoma 9 8 100.0 0.0 0.0 0.0 Endometrioid carcinoma of the ovary 130 120 100.0 0.0 0.0 0.0 Serous carcinoma of the ovary 580 551 99.8 0.0 0.2 0.0 Mucinous carcinoma of the ovary 101 89 100.0 0.0 0.0 0.0 Clear cell carcinoma of the ovary 51 48 100.0 0.0 0.0 0.0 Carcinosarcoma of the ovary 47 47 100.0 0.0 0.0 0.0 Granulosa cell tumor of the ovary 44 38 100.0 0.0 0.0 0.0 Leydig cell tumor of the ovary 4 4 100.0 0.0 0.0 0.0 Sertoli cell tumor of the ovary 1 1 100.0 0.0 0.0 0.0 Sertoli Leydig cell tumor of the ovary 3 3 100.0 0.0 0.0 0.0 Steroid cell tumor of the ovary 3 3 100.0 0.0 0.0 0.0 Brenner tumor 41 41 100.0 0.0 0.0 0.0 Tumors of the breast Invasive breast carcinoma of no special type 1764 1663 100.0 0.0 0.0 0.0 Lobular carcinoma of the breast 363 336 100.0 0.0 0.0 0.0 Medullary carcinoma of the breast 34 32 100.0 0.0 0.0 0.0 Tubular carcinoma of the breast 29 25 100.0 0.0 0.0 0.0 Mucinous carcinoma of the breast 65 56 100.0 0.0 0.0 0.0 Phyllodes tumor of the breast 50 44 100.0 0.0 0.0 0.0 Tumors of the digestive system Adenomatous polyp, low-grade dysplasia 50 50 100.0 0.0 0.0 0.0 Adenomatous polyp, high-grade dysplasia 50 50 100.0 0.0 0.0 0.0 Adenocarcinoma of the colon 2483 2306 100.0 0.0 0.0 0.0 Gastric adenocarcinoma, diffuse type 215 202 100.0 0.0 0.0 0.0 Gastric adenocarcinoma, intestinal type 215 204 100.0 0.0 0.0 0.0 Gastric adenocarcinoma, mixed type 62 61 98.4 1.6 0.0 0.0 Adenocarcinoma of the esophagus 83 71 100.0 0.0 0.0 0.0 Squamous cell carcinoma of the esophagus 76 61 100.0 0.0 0.0 0.0 Squamous cell carcinoma of the anal canal 91 83 100.0 0.0 0.0 0.0 Cholangiocarcinoma 58 54 100.0 0.0 0.0 0.0 Gallbladder adenocarcinoma 51 49 98.0 2.0 0.0 0.0 Klatskin tumor
留言 (0)