
記住我
Humanism Rounds was accepted into the ACGME Back to the Bedside collaborative in October 2017. The project was conducted within the BCM Internal Medicine Residency, a large academic multi-center training program in Houston, Texas, with approval from the BCM Institutional Review Board.
Project ComponentsThe project consisted of three components: “Human Histories,” “Humanism Rounds,” and “Celebrations.” “Human Histories” focused on eliciting aspects of a patient’s history that are not directly related to his or her medical condition, such as hobbies and personal interests (see Fig. 1). Human Histories were conducted during Humanism Rounds in which a resident would select one patient to visit at the bedside for 10–20 min as a team or one-on-one. Patient care coverage was provided by attending physicians and chief medical residents to enable residents to have uninterrupted conversations during Humanism Rounds. Celebrations were monthly, hospital-wide gatherings when all residents were invited to share stories from their Humanism Rounds experiences during regularly scheduled didactic sessions.
Fig. 1 Project PhasesPilot Phase
Project PhasesPilot PhaseBetween January and March 2018, a pilot phase of the initiative was conducted to ensure that resident participation in Humanism Rounds did not detract from patient care or create excess resident burden. Thirty volunteers were recruited via email and surveyed using an institutional questionnaire which solicited feedback on burnout, meaning at work, and feasibility of integrating the intervention components into daily practice (see Fig. 2).
Fig. 2
Humanism Rounds Survey (institutionally created)
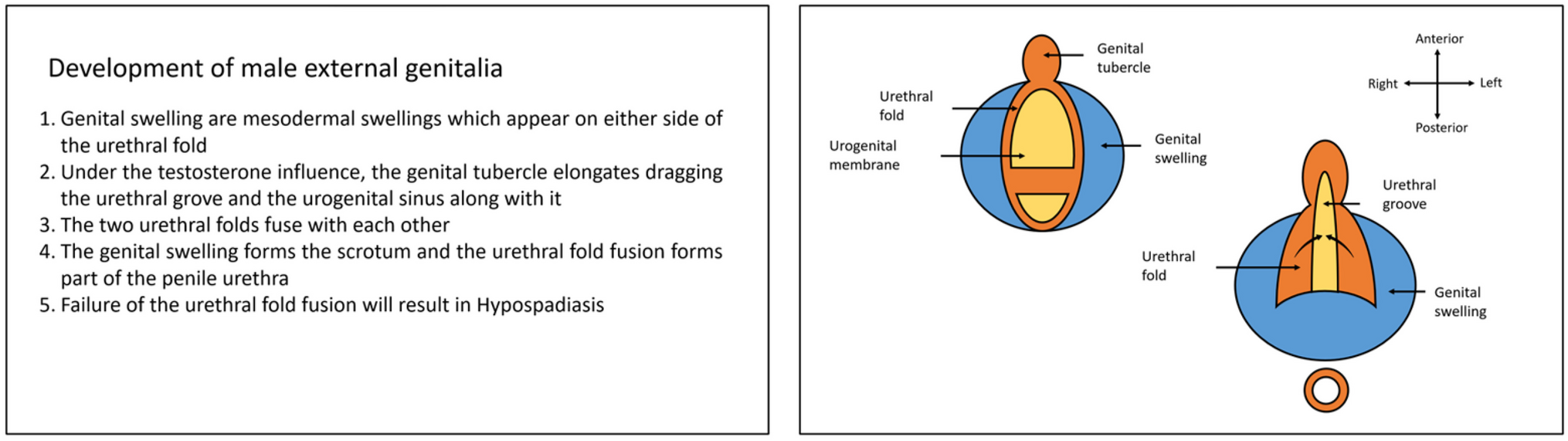
Intervention PhaseFollowing the pilot phase, the intervention was expanded to include all residents on inpatient rotations at any affiliated teaching hospital (including Ben Taub General Hospital, the Michael E. Debakey Veterans Affairs Medical Center, Baylor St. Luke’s Medical Center, or MD Anderson Cancer Center). All residents were introduced to the Humanism Rounds project components either during regular didactic sessions (upper level residents) or during orientation (interns). An instructional PowerPoint explained the background for the project and taught residents how to elicit a Human History using the PEOPLES mnemonic: P, place; E, environment; O, occupation; P, people; L, likes; E, entertainment; S, service (military, for veteran patients) (see Appendix A). Interns and residents were also provided with a pocket card with guidance for taking a Human History (see Fig. 1). Though participation was optional, residents were regularly encouraged to incorporate Human Histories and to participate in Humanism Rounds individually or with their teams. Celebrations were held at the end of each month, facilitated by chief residents or Back to Bedside resident ambassadors. Suggested discussion prompts were provided; the prompts encouraged residents to consider their experiences with a range of emotions, thus facilitating self-reflection [11] (see Table 1).
Table 1 Suggested discussion prompts during Humanism Rounds celebrationsData CollectionData were collected using institutionally created Humanism Rounds surveys (see Fig. 2) as well as a compilation “Back to Bedside Assessment Tool” curated by ACGME for use by all Back to Bedside initiatives. The institutionally created survey asked specific questions regarding the Humanism Rounds intervention, such as the extent to which a resident was incorporating Human Histories into their patient interviews, and whether the Humanism Rounds initiative impeded patient care or clinician learning. The survey also asked residents to rate their level of burnout and meaning in work. The Back to Bedside Assessment Tool provided by ACGME included validated assessments of burnout, meaning at work, and the learning environment, such as the Maslach Burnout Inventory [14], the Work and Meaning Inventory [15], the Subjective Vitality Scale [16], and the Learning Climate Questionnaire [17]. Due to copyright constraints, the compilation Back to Bedside Assessment Tool could not be included as part of this report.
To assess the effectiveness of the intervention, residents were asked to complete baseline surveys (both institutionally created and the ACGME Back to Bedside Assessment Tool) in July to August 2018, with follow-up surveys conducted in January and February of 2019 and 2020. Although residents were also surveyed in 2020, response rates were limited due to COVID-19-related interruptions in residency activities, and the data was thus omitted from analysis. Resident participation in the Humanism Rounds program, including survey completion, was voluntary.
Statistical AnalysisResident characteristics, survey responses, and survey scores were summarized by median with minimum and maximum values or by frequency with percentage. The Wilcoxon rank-sum, Fisher’s exact, or Chi-square test was used to make comparisons as appropriate. Since resident identification was unknown, we could not be sure the same residents completed surveys both pre- and post-interventions, so any analyses which compared between the two survey time points were done within each level of training for the assumption of independent observations to be satisfied. p < 0.05 was used for statistical significance.
留言 (0)