
記住我




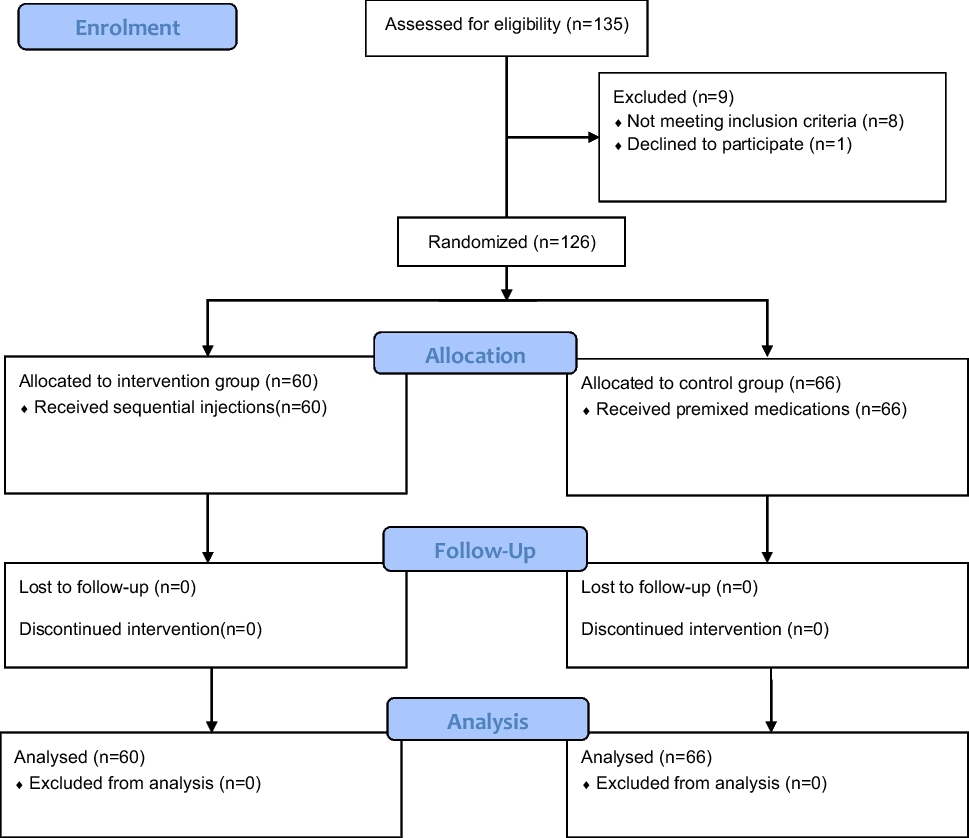
Six extra tutorials were offered over a seven-week period, and the attendance rate was 54% across the three clinical sites. The majority of the students who went through the remediation program subsequently went on to pass their second LCA (88%) (Fig. 1).
Fig. 1
88% of students who failed their first LCA passed the second LCA
Of those who failed the final year exam overall, 50% had been in the remediation program. Despite 88% of students in the remediation group obtaining a passing grade in their second LCA, 25% of this group did not reach a passing grade overall. This was due to failure in other components of the overall exam. For example, those who failed the second LCA had a significantly lower score in their surgical MCQ examination (54.62 vs 44.28, p = 0.046).
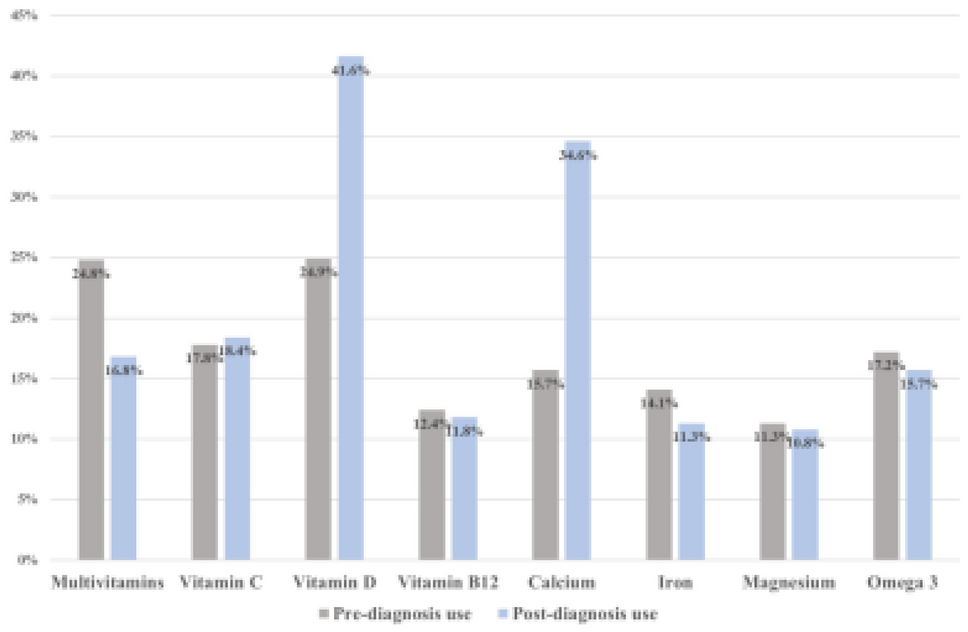
Neither the total number of extra tutorials offered to students, nor their percentage attendance at these tutorials had a statistically significant effect on their second LCA results (p = 0.624). Percent attendance at tutorials was not found to statistically impact second LCA scores (Fig. 2).
Fig. 2
Correlation between second LCA score and attendance (%) at extra tutorials in male and female students
Factors such as sex and examination site were not found to have a statistically significant effect on second LCA result or score in the remediation cohort.
Picking the right people for remediation: comparison with the overall classIn phase 2, we combined the non-remediation students with the remediation students to assess whether the results obtained in phase 1 were applicable to the entire year group. We found that students in the non-remediation group scored significantly higher in second LCA (59.71% vs 52.07%, p < 0.001). However, 83% of students who failed LCA2 were in the non-remediation group.
The non-remediation group was found to have consistently performed better in assessments throughout the academic year when compared to the remediation group (Table 1).
Table 1 Raw assessment scores in remediation vs non-remediation groups across different assessment modalities. Data by long case assessment 2 results (pass [≥ 50]/fail [< 50])Females performed significantly better in both first LCA (60.16% vs 57.91%, p = 0.009) and second LCA (61.21% vs 59.21%, p = 0.039), as well as other forms of in-person assessment, such as Surgical TOSBAs 1 and 2, Medicine Case Presentation 2, and Surgical Case Presentations 1 and 2.
Female sex had no statistically significant impact on other forms of in-person and written assessment, including the Medicine Mock Long Case, Medicine Case Presentation 1, Medicine TOSBAs 1 and 2, Medicine MCQ, Surgery MCQ, or SUBI Assessment. The reasons for these gender differences are unclear.
Students who failed the second LCA but passed the first LCALooking specifically at the cohort of students who passed the first LCA and subsequently failed the second LCA; they were significantly weaker compared to the overall class across practically all summative assessments throughout the year (Table 2).
Table 2 Summative assessment scores of students who passed first long case and failed second long case compared to rest of the classOverall failing grade6.25% of the class failed the year overall. Failing students were also more likely to have failed their penultimate year (SC1). A statistically significant proportion had failed their medical mock long case compared with the rest of the class, whilst Surgical TOSBA results were significantly lower between the failing and passing groups. These characteristics are summarised in Table 3 below.
Table 3 Academic characteristics of students who failed the year overall
留言 (0)