
記住我









The case report was conducted in accordance to the World Medical Association Declaration of Helsinki and approved by the Ethics Committee of Jiaxing First Hospital (2022-LY-411). The patient had signed informed consent forms.
An 18-year-old male patient was admitted to our hospital with a 1-month anorexia, accompanied by nausea, vomiting, and weight loss. The patient had been administered ceftriaxone and omeprazole for 15 days at a local hospital, without significant improvement.
Serum creatinine and urine protein levels increased within 3 months. Therefore, this patient was diagnosed with acute kidney disease. A detailed list of the paraclinical investigations is presented in Supplementary Appendix B. The kidney biopsy showed acute tubulointerstitial nephritis (Fig. 1).
Fig. 1
Results of renal biopsy. A Immunofluorescence: no immune complex deposit. B–D The electron microscope showed that the podocytes of the glomerulus were segmental fused, and there was no exact deposition of electronic dense matter in various parts of the glomerulus. (E) HE staining (×200). (F) PAS staining (×400). (G) PASM staining (×400). (H) Masson staining
The patient had no recent history of exposure to chemicals, drugs or foods that might cause acute renal injury. The patient reported redness and discomfort in his eyes during his preceding admission to a local hospital, which improved after 1 day. Accordingly, we consulted ophthalmologists and conducted slit-lamp examinations, which identified bilateral iridocyclitis (Fig. 2).
Fig. 2
Slit lamp inspection results. (A) Right eye. (B) Left eye. The green arrow indicates keratic precipitates (KP)
TINU syndrome was diagnosed, based on the renal pathology and the ocular lesions. Methylprednisolone (80 mg) was administered intravenously once a day for four consecutive days, and methylprednisolone tablets (48 mg) were administered once a day. All indicators improved after the treatment (Supplement Appendix B). During a follow-up period of > 5 months, the patient’s steroid therapy was discontinued, and there was no recurrence of renal damage or uveitis.
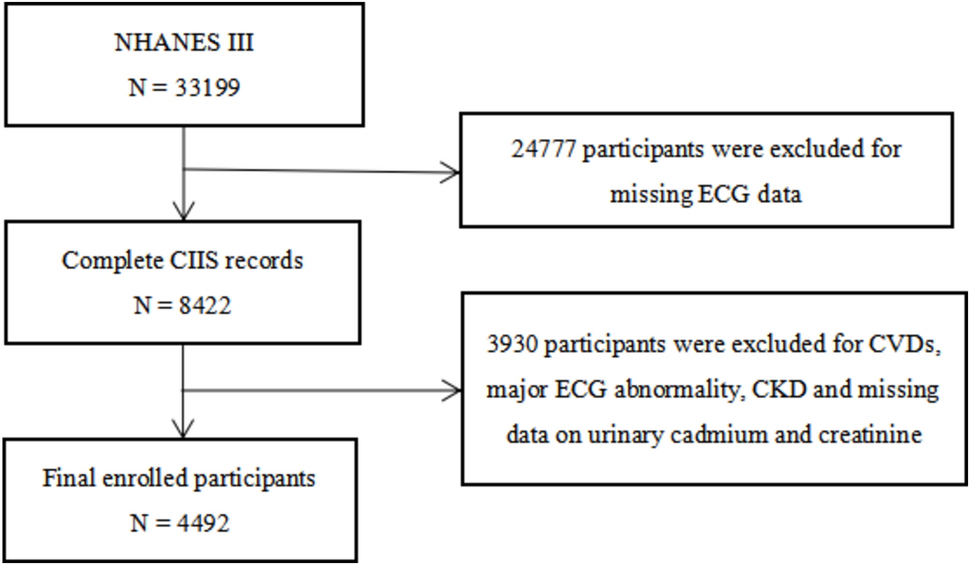
Systematic review search resultsA total of 115 relevant documents were retrieved; 57 duplicate documents were excluded, three documents were excluded because they are not related to the theme of this article after review of titles and abstracts, and 20 documents were excluded according to the exclusion criteria after visiting the full text (Fig. 3). Thirty-five publications met the inclusion criteria [10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44], comprising 34 case reports and one case series, totaling 70 cases. The characteristics of the included publications are summarized in Table 1.
Fig. 3
PRISMA study selection flowchart for systematic literature Review
Table 1 Characteristics of the included studiesDemographic informationA total of 71 cases were included in this article, of which 70 were from publications and 1 was from our hospital. 38 were from Beijing, but there was no evidence of regional ethnic distribution differences in TINU syndrome in China. In 39 cases mentioning the triggering factors of TINU syndrome was: unclear (69%), infections (28%), drugs (3%). 11 patients had infectious triggers before acute kidney injury, of which nine patients had upper respiratory tract infection, one had cholecystitis, and one had urinary tract infection. Only one patients used herbal medicine which was not elaborated in the case report for 2 weeks before his serum creatinine found to be elevated. Twenty-eight patients were male and 43 were female, with a male-to-female ratio of 1:1.5 (Table 2). For those aged ≥ 18 years, 67% were female, while males accounted for 59% of those under 18 years of age. TINU syndrome tends to occur in young men and middle-aged women in China.
Table 2 Data of patients with TINU syndromeClinical and laboratory dataThe patients had various symptoms, including fatigue, fever, and gastrointestinal manifestations such as nausea, vomiting, loss of appetite, and weight loss. Eleven patients urinate at least 2 times per night (Table 2). We conducted subgroup analysis according to sex and age. There were no statistically significant differences in clinical symptoms between men and women or in terms of age (Tables 3, 4).
Table 3 Comparison between male subgroup and female subgroupTable 4 Comparison between adolescent subgroup and adult subgroupAmong the 35 patients with renal function data, all showed non-oliguric acute renal injury; average values of serum creatinine, urea nitrogen and 24-h urine protein were was 317.8 μmol/L, 13.7 mmol/L, and 1.14 ± 0.7 g/24 h, respectively. Increased ESR was reported in 26/27 patients. Proteinuria was present in 34/37 (92%) patients and Urinary glucose abnormalities with normal blood glucose levels developed in 27/33 (82%) patients. The renal biopsy results in 67 patients were consistent with acute tubulointerstitial nephritis (ATIN). Four patients who did not undergo renal biopsy had abnormal renal function, abnormal urine test results, and systemic disease lasting for 2 weeks.
UveitisIn the 71 cases, anterior uveitis was found in 55%, intermediate uveitis in 13%, and panuveitis 10%. Bilateral uveitis was present in 53/71 cases. The patients exhibited various ocular symptoms, including redness, eye pain, blurred vision, and photophobia. The relationship between uveitis and ATIN remains unclear; 54% of the 70 patients had uveitis after ATIN, 30% had uveitis at the same time as ATIN, and 16% had uveitis before ATIN (Table 2). Subgroup analysis found that uveitis occurred after ATIN in 77% of those aged under 18 years, compared to 47% of adult patients (P < 0.05). There were not statistically significant differences in ocular symptoms between men and women (Tables 3, 4).
Treatments and outcomesGlucocorticoid therapy was the first-line treatment for TINU in China. 47 patients were treated with glucocorticoids alone and 22 cases were treated with glucocorticoids combined with immunosuppressive agents, including mycophenolate mofetil (n = 10), cyclophosphamide (n = 8), azathioprine (n = 3) and unspecified (n = 1). All patients under 18 years received glucocorticoid therapy alone.
The outcomes of 51 patients with a follow-up period of > 6 months were analyzed. The median follow-up period was 24 months (IQR 12–36). Recurrent uveitis means that the eye symptoms of patients disappear after treatment, and then the eye symptoms reappear 3 months later. Recurrent uveitis or the course over 3 months defined chronic uveitis was present in 24/51 (47%) patients, comprising 10 males and 14 females, 6 aged less than 18 years and 18 adults. Forty-two out of 51 patients with a follow-up period of > 6 months for whom there was follow-up data on renal function, of which twenty patients experienced kidney disease recurrence or progression to CKD, including seven males and thirteen females. The incidence was higher in adults (58%) than in young adults (18%) (P < 0.05).
留言 (0)