
記住我

Pancreaticoduodenectomy is one of the most challenging abdominal surgeries and remains the standard treatment for pancreatic and periampullary tumors.1 Conventionally, the procedure has been performed using the open technique [open pancreaticoduodenectomy (OPD)]. Since the first description of laparoscopic pancreaticoduodenectomy (LPD) by Gagner in 1994, interest in LPD has progressively increased2; however, large-scale case series describing this technique were conducted only in a few highly specialized centers.3–8 LPD has been shown to be feasible and safe, and has several potential advantages, including lower blood loss, transfusion requirements, intensive care unit stay, and total hospital stay, compared with OPD. However, whether potential advantages such as shorter hospital stay and quicker recovery can translate to better long-term survival remains unclear.
Long-term survival is the gold standard endpoint for evaluating the oncological efficacy of any anticancer intervention provided to cancer patients. In the setting of pancreaticoduodenectomy, several studies have compared the oncological outcomes and long-term survival of patients who underwent LPD or OPD,9,10 and its oncological safety remains controversial.11,12 Short-term outcomes, such as length of stay can be affected by country-specific sociocultural factors and health care policies. In addition, other in-hospital outcomes can be influenced by discharge criteria, disease pathologic types, surgeon’s preference, and patients’ level of self-comfort. Thus, the measure can be fairly subjective. Besides, the early termination of LEOPARD-2 study, due to the unexpected and worrisome short-term safety concerns, also raised questions about the feasibility of LPD.5 Together with these concerns, postoperative long-term survival and quality of life may be more valuable indicators than in-hospital or short-term outcomes when evaluating the oncological efficacy of a surgical technique.
The TJDBPS01 trial was designed with short-term length of stay as its primary endpoint, and it was also powered to determine its effects on overall survival (OS). At the time of the primary analysis of in-hospital length of stay, the outcomes of long-term follow-up were immature; the long-term outcomes of this study were updated after a minimum follow-up of 3 years, at the end of 2022. Herein, we report the data on the 3-year OS, quality of life, and effects of LPD among patients with benign, premalignant, or malignant lesions, especially the malignant tumors and causes of death in the per-protocol population.
METHODS Study Design and ParticipantsTJDBPS01 was a noninferiority, open-label, randomized clinical trial (RCT) conducted in 14 hospitals in China. The patients were enrolled from May 18, 2018, to December 19, 2019. All patients were followed up after surgery. The final follow-up was on December 31, 2022. Patients aged 18 to 75 years with benign, premalignant, or malignant resectable pancreatic or periampullary tumors who were eligible to undergo pancreaticoduodenectomy were enrolled in this study. Patients who (1) had distant metastases; (2) underwent left, central, or total pancreatectomy or palliative surgery other than pancreaticoduodenectomy; (3) had an American Society of Anesthesiologists score of at least 413; (4) had synchronous malignancy in other organs or second cancer requiring resection during the time of surgery; (5) were pregnant; and (6) underwent or required neoadjuvant chemoradiotherapy were excluded. The detailed exclusion criteria can be seen in Supplemental Digital Content 1 (https://links.lww.com/SLA/E939). A complete overview of the study protocol has been published.14 The study was also reported in accordance with the CONSORT checklist (Supplemental Digital Content 2, https://links.lww.com/SLA/E939).
Each participating center obtained institutional review board approval according to the local regulations. Written informed consent was obtained from all the patients. In addition, experienced surgeons who (1) had performed at least 104 LPDs and OPDs,15 (2) had completed the Minimally Invasive Treatment Group in the Pancreatic Disease Branch of China’s International Exchange and Promotion Association for Medicine and Healthcare (MITG-P-CPAM) LPD training program, and (3) had unedited videos of them performing LPD and OPD evaluated by independent experts and whose performance was considered a PASS were included in this study. Finally, 14 surgeons and their surgical teams from MITG-P-CPAM were selected for this trial.
The participants were randomly assigned in a 1:1 ratio to groups that underwent either LPD or OPD. A detailed description of the main results has been published along with the clinical and demographic baseline characteristics.16 OS was calculated from the date of surgery until the date of death from any cause (event). Patients who were lost to follow-up were censored at the last date they were known to be alive, and patients who remained alive were censored at the time of data cutoff. The reasons for deaths were also recorded during the follow-up. Other endpoints included 3-year OS, defined as the proportion of patients that survived at 3 years. Other follow-up outcomes included long-term safety, health-related quality of life, and depression incidence. Since no standard schedule exists for the collection of patient-reported outcomes after surgery, timepoints for health-related quality of life and depression assessments were chosen on the basis of the patient follow-up schedule in this study.14
Quality of Life AssessmentThe health-related quality of life was assessed using the 3-level version of the European Quality of Life—5 Dimensions (EQ-5D-3L), which included both a health description system (EQ-5D index) and a Visual Analog Scale (VAS).17,18 The first section recorded the self-assessed health status based on the following 5 dimensions: mobility, self-care, daily activities, pain/discomfort, and anxiety/depression. Each dimension consisted of 3 levels: no problems, some problems, and extreme problems.19,20 The second component was used to assess the level of self-perceived health, which ranged from 0 to 100, with 0 representing the worst conceivable state of health and 100 representing the best state of health. VAS can be used as a quantitative measure of a participant’s self-judged health outcomes.
Depression AssessmentThe symptoms of depression were assessed using the Chinese version of the 10-item Center for Epidemiology Studies Depression (CESD-10) scale. The CESD-10 scale is based on the CES-D scale, a widely used standardized tool for measuring depression and can be more time-efficient than the CES-D, thus easing participants’ response burden; it is more applicable for the nonclinical, general population than for clinically depressed patients. The participants were asked to answer 10 items to assess for depressive symptoms, including depressed mood, restless sleep, decreased energy, decreased enjoyment, and decreased hope in life, as well as feelings of fear, loneliness, and despair experienced in the past week. The scores for each item were summed to obtain the total score, which ranged from 0 to 30, with higher scores indicating worse depression. The symptoms of depression were dichotomized into nonsignificant (CES-D <10) and significant (CES-D ≥10) symptoms, in line with the recommendations.21,22
Statistical AnalysisAll analyses conducted herein were exploratory. Prespecified subgroup analyses were conducted based on histopathology types, which encompassed malignancies and other categories. Malignancies included pancreatic ductal adenocarcinoma (PDAC), duodenal adenocarcinoma, ampullary adenocarcinoma, and cholangiocarcinoma. Benign lesions included intraductal papillary mucous neoplasm, serous cystic neoplasm, mucous cystic neoplasm, and other noninvasive lesions. Borderline lesions included solid pseudopapillary tumor, pancreatic neuroendocrine tumor, and gastrointestinal stromal tumor. In our analysis, benign and borderline lesions were combined as “Other” to facilitate data analysis and interpretation.
The OS analysis was specifically conducted on malignancies, whereas the analysis of other follow-up outcomes encompassed the entire patients. The Kaplan-Meier curves and log-rank test were used to estimate the difference in OS between the groups. Patients who were lost to follow-up or were still alive at the last contact were considered as censored. Cox proportional hazards regression analysis was used to determine the impact of covariates on OS, yielding hazard ratios (HRs) as measures of effect. The median follow-up time was determined by reverse censoring at the time of death. Instead of using the median survival time, the restricted mean survival time (RMST), which represents the area under the Kaplan-Meier curve within a specific time window, was used as a reasonable summary to quantify the survival time. In addition, a competing risk regression analysis was conducted to account for different causes of death, with the Gray test being used to assess the differences between the LPD and OPD groups, as a sensitivity analysis. All analyses were performed on an intention-to-treat basis. All the statistical tests for secondary end points had a 2-sided significance level of 0.05. Because of the potential for type I error due to multiple comparisons, findings for analyses of secondary end points should be interpreted as exploratory. All statistical analyses were performed using SAS, version 9.4 (SAS Institute Inc.). The detailed statistical analysis plan can be seen in Supplemental Digital Content 3 (https://links.lww.com/SLA/E939).
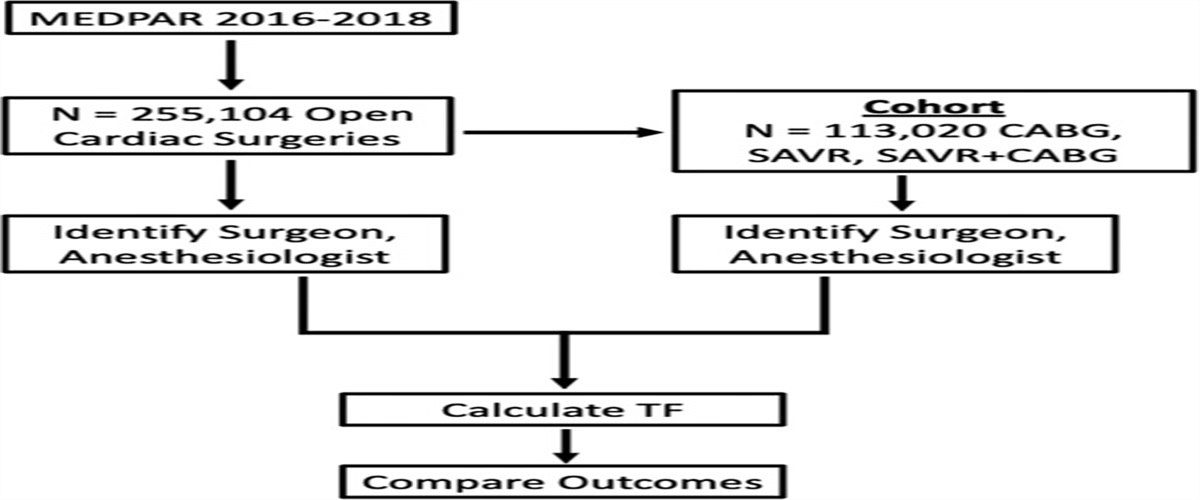
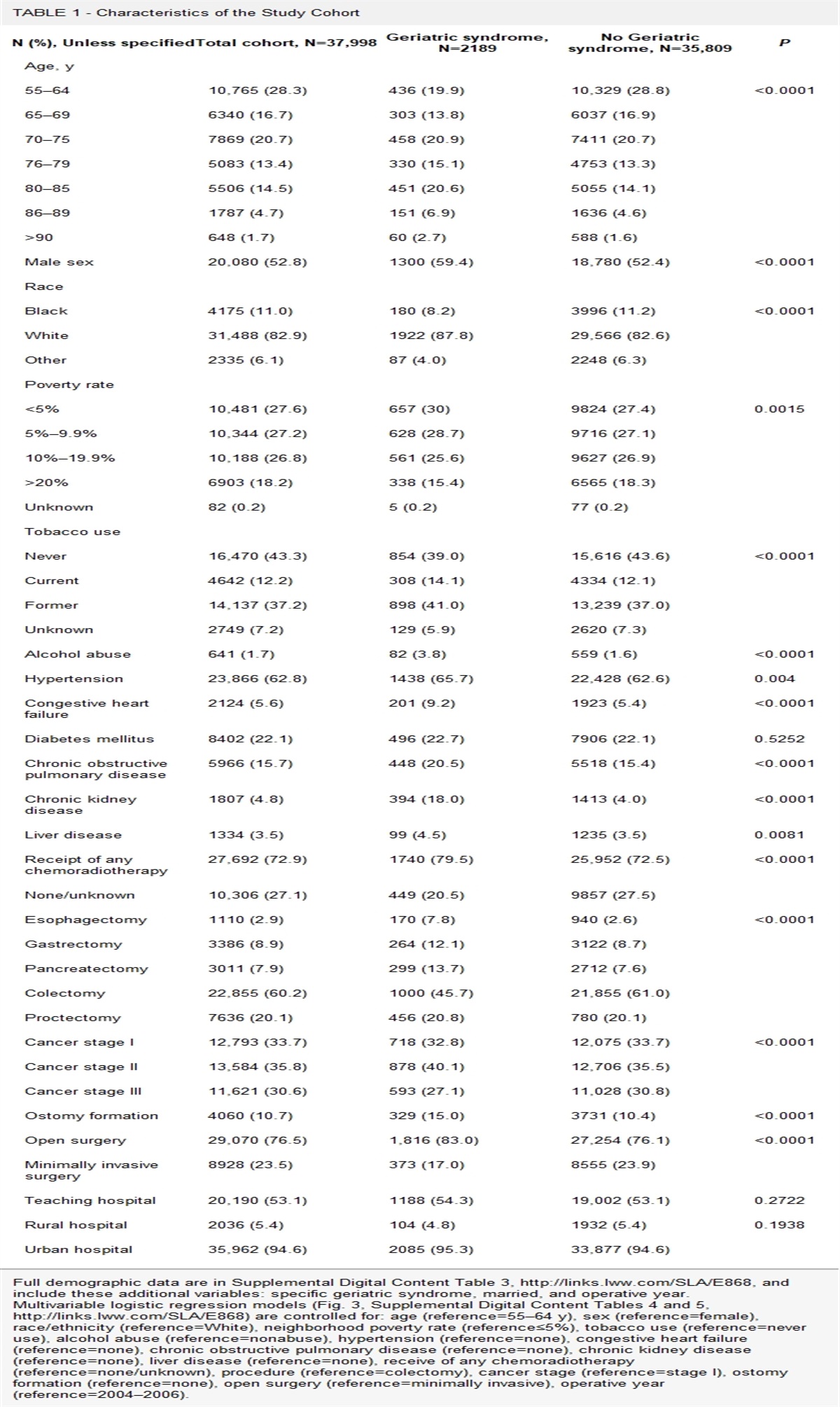
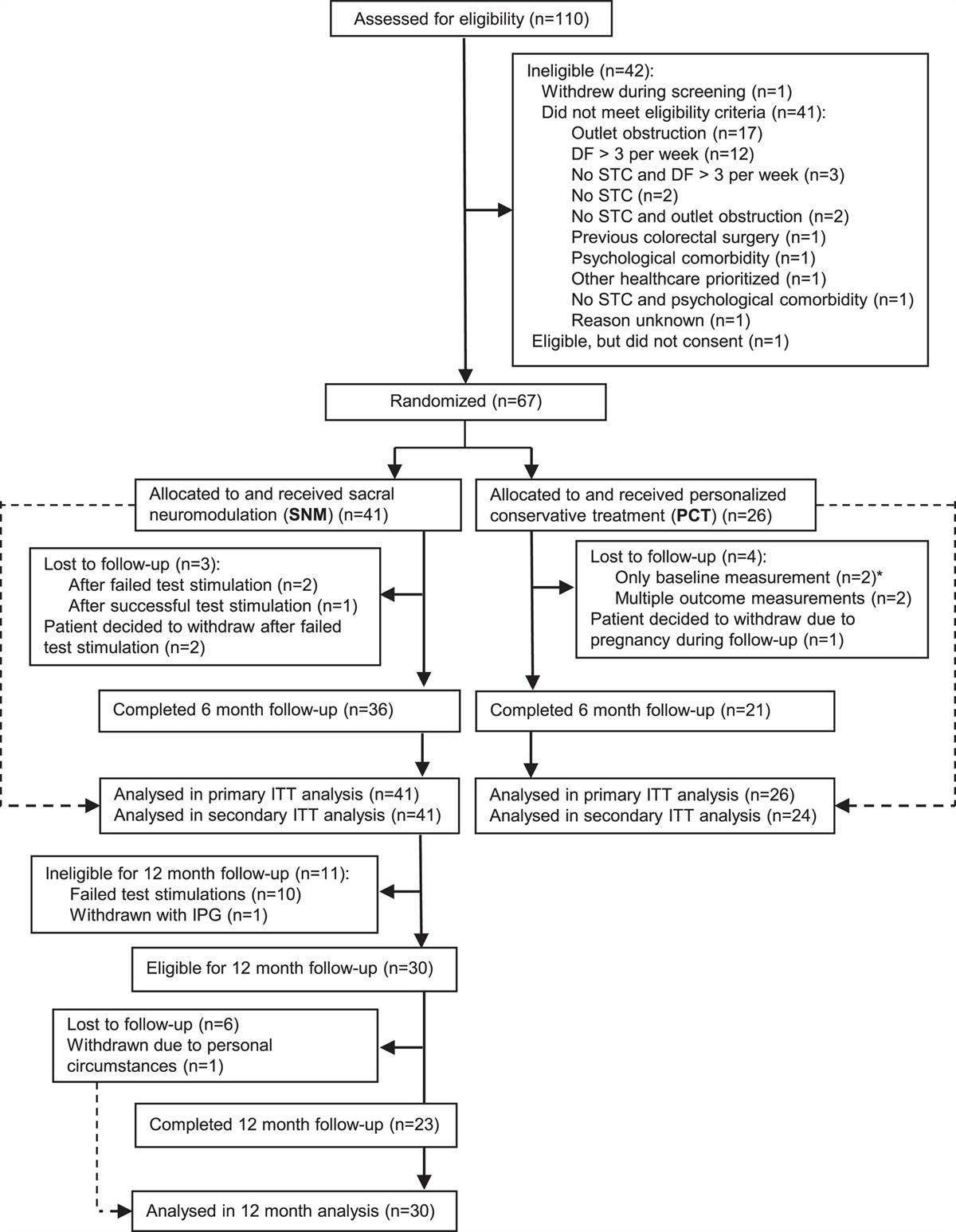
RESULTS Study PopulationFrom May 18, 2018, to December 19, 2019, 328 patients were randomly assigned to the LPD group and 328 to the OPD group (Fig. 1). The primary analysis set comprised of 594 patients (297 in the LPD group and 297 in the OPD group). The median follow-up period was 49 months (interquartile range: 44–52 months), with 67 patients (10.9%) lost to follow-up. Finally, 529 patients were included in this analysis, including 268 patients in the LPD group and 261 in the OPD group. A detailed description of the study protocol and the main results have been published previously with clinical and demographic baseline characteristics.16 Detailed information regarding the patients’ characteristics and operative data are presented in Table 1, and the pathologic and postoperative results are presented in Table 2.
 FIGURE 1:
FIGURE 1: Study flowchart. PD indicates pancreaticoduodenectomy.
TABLE 1 - Patients‘ Characteristics and Operative Data Surgery [n (%)] Characteristics Laparoscopic surgery (N=268) Open surgery (N=261) P Baseline characteristics Age [mean (SD)] (yr) 59.2 (10.2) 57.8 (10.8) 0.12 Male 155 (57.8) 167 (64.0) 0.15 BMI [mean (SD)] (kg/m2) 22.4 (2.9) 22.0 (3.0) 0.16 ASA classification I 47 (17.5) 44 (16.9) 0.36 II 158 (59.0) 168 (64.4) III 63 (23.5) 49 (18.8) Wirsung duct diameter <3 mm 161 (60.1) 150 (57.5) 0.54 Firm or hard consistency of pancreas 106 (39.6) 110 (42.2) 0.53 Preoperative biliary drainage 63 (23.5) 68 (26.1) 0.50 Tumor location Pancreas 140 (52.2) 130 (49.8) 0.93 Bile duct 42 (15.7) 44 (16.7) Duodenum 55 (20.5) 58 (22.2) Ampullary 31 (11.6) 29 (11.1) Pathologic properties Malignant 201 (75.0) 197 (75.5) 0.84 Benign 44 (16.4) 45 (17.2) Borderline 23 (8.6) 19 (7.3) AJCC staging* I 52 (19.4) 47 (18.0) 0.64 II 106 (39.6) 116 (44.4) III 44 (16.4) 35 (13.4) Operative results Operative time [median (IQR)] (min) 320.0 (280.0–390.0) 300.0 (250.0–360.0) <0.001† EIBL [median (IQR)] (mL) 200.0 (100.0–375.0) 300.0 (200.0–440.0) <0.001† Intraoperative blood transfusion 60 (22.4) 79 (30.3) 0.04 Pancreatic reconstruction Duct to mucosa 147 (54.9) 132 (50.6) 0.35 Other 121 (45.2) 129 (49.4) Vascular resection 7 (2.6) 7 (2.7) 0.96 Conversion 9 (3.4) 0 (0.0) NA Positive resection margin 7 (2.6) 8 (3.1) 0.75‡ Stent 50 (18.7) 42 (16.1) 0.44*For pathologic stage of malignancy.
†Wilcoxon rank-sum test.
‡Fisher’s exact test.
AJCC indicates American Joint Committee of Cancer; ASA, American Society of Anesthesiologists; EIBL, estimated intraoperative blood loss; IQR, interquartile range; NA, not available.
*Other included intraductal papillary mucous neoplasm, pancreatic neuroendocrine tumor, serous cystic neoplasm, mucous cystic neoplasm, solid pseudopapillary tumor, gastrointestinal stromal tumor, and other cancer types.
†Wilcoxon rank-sum test.
‡Fisher exact test.
ICU indicates intensive care unit; IQR, interquartile range; POPF, postoperative pancreatic fistula.
At the time of the analysis, 213 patients (40.3%) had died [104 (38.8%) in the LPD group and 109 (41.8%) in the OPD group]. Among patients with malignant tumors, the 3-year OS rates were 59.1% and 54.3% in the LPD and OPD groups, respectively (HR: 1.16, 95% CI: 0.86–1.56, P=0.33) (Fig. 2). The HR for OPD versus LPD was 1.11 (95% CI: 0.81–1.51, P=0.53) after adjusting for age, sex, body mass index (BMI), American Society of Anesthesiologists status, comorbidity, tumor size, histologic features, TNM stage, and chemotherapy. The 3-year OS rates of the LPD and OPD groups were 51.8% and 48.9% in patients with PDAC, 59.7% and 69.0% in patients with duodenal adenocarcinoma, 68.2% and 76.2% in patients with ampullary adenocarcinoma, and 63.6% and 40.5% in patients with cholangiocarcinoma, respectively. After adjusting for covariates, the adjusted HRs for the 3-year OS of the LPD and OPD were 0.99 (95% CI: 0.61–1.59) in patients with PDAC, 0.97 (95% CI: 0.43–2.18) in patients with duodenal adenocarcinoma, 1.36 (95% CI: 0.21–8.61) in patients with ampullary adenocarcinoma, and 2.74 (95% CI: 1.19–6.30) in patients with cholangiocarcinoma (Supplemental Digital Content 4, Figs. S1–S4, https://links.lww.com/SLA/E939).
 FIGURE 2:
FIGURE 2: A, Survival curves between LPD and OPD among patients with malignancies. B, Survival curves between LPD and OPD among patients with other histopathologic types.
Truncation was set at 36 months to evaluate the RMST for malignant tumors. In the LPD group, the RMST was 27.3 months (95% CI: 25.6–29.1), and the corresponding restricted mean times lost were 8.7 months (95% CI: 7.0–10.5). In the OPD group, the RMST was 26.6 months (95% CI: 24.8–28.4), and the corresponding restricted mean times lost were 9.4 months (95% CI: 7.6–11.2). The RMST ratio for OPD to LPD was 0.974 (95% CI: 0.89–1.07), indicating that the LPD group had a median survival time that was 2.6% less than that of the OPD group (P=0.583) (Supplemental Digital Content 4, Table S1, https://links.lww.com/SLA/E939).
The univariate analysis of OS among patients with malignancies found no differences in the outcomes of OPD versus LPD in terms of age, sex, BMI, pathologic properties, and American Joint Committee on Cancer (AJCC) stage (Fig. 3). The causes of death were analyzed for all patients as a sensitivity analysis. The distribution is presented in Supplemental Digital Content 4, Table S2 (https://links.lww.com/SLA/E939). After controlling for all other competing risk events, the cancer-related deaths and deaths from other causes did not differ significantly between the LPD and OPD groups. In the sensitivity analysis, the subdistribution hazard model for cancer-related deaths and deaths from other causes also did not significantly differ between the LPD and OPD groups (Supplemental Digital Content 4, Figure S5, Table S3, https://links.lww.com/SLA/E939).
 FIGURE 3:
FIGURE 3: The forest plot of the OS among patients with malignancy at 3 years of follow-up. AJCC indicates American Joint Committee of Cancer; ASA, American Society of Anesthesiologists.
Follow-up OutcomesAmong patients with malignant tumors, the relapse rates were 35.6% and 40.4% in the LPD and OPD groups, respectively (P=0.49), during follow-up. A total of 59 (48.8%) patients with malignant tumors in the LPD group and 72 (58.1%) in the OPD group (P=0.14) received adjuvant chemotherapy. In addition, the mean times to the initiation of adjuvant chemotherapy were 2.8 and 3.1 months in the LPD and OPD groups, respectively (P=0.83). The median numbers of postoperative chemotherapy cycles were 6 and 3 cycles in the LPD and OPD groups, respectively (P=0.02).
A total of 200 patients participated in the EQ-5D-3L questionnaire survey; the mean EQ-5D-3L health utility scores were 0.9 (SD: 0.1) in the LPD group and 0.9 (SD: 0.2) in the OPD group, with no significant difference between the 2 groups (P=0.42). The median VAS scores were 85 and 80 in the LPD and OPD groups, respectively (P=0.71). The median depression scores were 15 and 16 in the LPD and OPD groups, respectively (P=0.29), and the median IDL score was 10 in both groups (P=0.77). Detailed follow-up information of the LPD and OPD groups according to malignancy and other data is presented in Table 3 and the Appendix (Supplemental Digital Content 4, Table S4, https://links.lww.com/SLA/E939).
TABLE 3 - Follow-up Information of the LPD and OPD Groups Malignancies* Other† LPD (N=201) OPD (N=197) P LPD (N=67) OPD (N=64) P Cause of death Cancer-related death [n (%)] 84 (92.3) 90 (90.9) 0.73 10 (76.9) 8 (80.0) >0.99 Other causes‡ [n (%)] 7 (7.7) 9 (9.1) 3 (23.1) 2 (20.0) Relapse [n (%)] 36 (35.6) 38 (40.4) 0.49 NA NA Adjuvant chemotherapy [n (%)] 59 (48.8) 72 (58.1) 0.14 NA NA Time to initiation of adjuvant chemotherapy [mean (SD)] (mo) 2.8 (3.0) 3.1 (7.4) 0.83 NA NA Chemotherapy cycles [median (IQR)] 6.0 (3.0–6.0) 3.0 (2.0–5.0) 0.02 NA NA EQ-5D-3L Health utility score [mean (SD)] 0.9 (0.1) 0.9 (0.2) 0.96 0.9 (0.1) 0.9 (0.1) 0.02 VAS [median (IQR)] 85.0 (70.0–90.0) 80.0 (70.0–90.0) 0.73 82.5 (77.5–92.5) 82.5 (75.0–90.0) 0.98 Depression [median (IQR)] 16.0 (10.0–16.0) 16.0 (11.0–17.0) 0.28 13.5 (10.0–16.5) 16.0 (11.0–17.0) 0.27*Malignancies included PDAC, duodenal adenocarcinoma, ampullary adenocarcinoma, and cholangiocarcinoma.
†Other included intraductal papillary mucous neoplasm, pancreatic neuroendocrine tumor, serous cystic neoplasm, mucous cystic neoplasm, solid pseudopapillary tumor, gastrointestinal stromal tumor, and other cancer types.
‡Includes other cancers, diseases other than cancer, and unknown causes.
IQR indicates interquartile range; NA, not available.
The univariate and multivariate analysis of the risk factors for OS identified that being female was an independent protective factor of OS (HR: 0.65, 95% CI: 0.47–0.89, P=0.009) (Supplemental Digital Content 4, Table S5, https://links.lww.com/SLA/E939). The surgical method, whether it is LPD or OPD, has no significant impact on the long-term survival of patients with malignancies (HR: 1.16, 95% CI: 0.86–1.57, P=0.33). Postoperative factors influencing the quality of life were also analyzed. Longer postoperative LOS (β=−0.002; P=0.03) and receive chemotherapy were associated with a lower quality of life (Supplemental Digital Content 4, Table S6, https://links.lww.com/SLA/E939).
DISCUSSIONLPD is a technically challenging operation primarily performed at high-volume tertiary centers. In our multicenter RCT comparing the effects of LPD and OPD in patients with pancreatic or periampullary tumors, the 3-year OS did not significantly differ between patients who underwent LPD and OPD performed by experienced surgeons at high-volume specialized centers, regardless of the tumor histopathologic type. Moreover, LPD was equivalent to OPD in providing statistically identical rates of margin-positive resection and lymph node clearance, time to adjuvant chemotherapy, and lengths of risk-adjusted OS. To our knowledge, this is the first RCT to report the long-term survival outcomes of LPD and OPD. These findings provide further evidence supporting the oncological safety and efficacy of LPD in the treatment of pancreatic or periampullary tumors.
Evaluating whether the potential short-term advantages of LPD could allow patients to achieve better long-term survival compared with OPD is of clinical relevance to promote a new technology and future trial designs. While, no other relevant RCTs have reported the long-term outcomes of LPD compared with OPD. Until now, 2 single-center RCTs (PLOT and PADULAP) and 1 multicenter RCTs (LEOPARD-2) comparing LPD with OPD have been published to date.5–7 Two of them (PLOT and PADULAP) found that LPD was associated with a shorter hospitalization time than OPD.6,7 While the other (LEOPARD2) was prematurely stopped because of safety concerns, as 90-day mortality was higher in the LPD group than in the OPD group.5 All these RCTs were focused on the short-term efficacy and safety, and did not conduct the long-term follow up. Thus, no RCTs have reported the long-term survival of LPD comparing with OPD. We were interested in the long-term survival of LPD comparing with OPD. Therefore, the TJDBPS01 trial have made the initial try. The primary analysis of the TJDBPS01 study identified clear short-term advantages typical of LPD, including reduced blood loss, shorter hospital stay, and faster recovery.16 The similar long-term survival outcomes between LPD and OPD showed that LPD shared similar long-term efficacy and safety compared with OPD. Besides, the RMST, a robust and clinically interpretable summary measure that is an alternative to HRs and median survival time, as it directly quantifies the information of the entire observed survival curve,23,24 showed that the mean survival time was only 0.3% lower in the LPD group than that in the OPD group. In addition, the short-term outcomes, such as the number of harvested lymph nodes, the rate of positive margins, and short-term survival, which are commonly used as surrogates of oncological outcomes,25 were also comparable between the LPD and OPD groups. These results suggest that LPD is oncologically noninferior to OPD, indicating that technically similar oncological resections can be achieved irrespective of the surgical approach used.
From the technical point of view, laparoscopic approaches have the benefits over open surgeries through visual magnification, better exposure, and more delicate maneuvers of organs, vessels, and nerves. Although the short-term safety is now established, the oncological efficacy of LPD is still under exploring. Numerous studies have reported comparable OS outcomes between LPD and OPD. For example, a meta-analysis of 10,554 pancreaticoduodenectomies that compared the effects of LPD and OPD in PDAC patients demonstrated no significant difference in the OS between the 2 approaches with moderate heterogeneity (HR: 0.97, 95% CI: 0.82–1.15).26 And similar OS rates have also been reported in elderly PDAC patients or in general PDAC patients.11,27 While, Zhu et al28 demonstrated that LPD was associated with improved OS compared with OPD in patients with resectable cholangiocarcinoma. Our findings are aligned with these findings. Besides, other characteristics, such as different BMI levels or AJCC stages, were also presented to have different long-term survival between LPD and OPD, as the HR showed opposite trends. Although these findings were not significant, they highlight the importance of considering patient-specific conditions and tumor characteristics when choosing surgical approach; therefore, further research is needed to explore the domain further.
In addition to the OS outcomes, other important oncological findings in this study included the earlier initiation of chemotherapy (mean: 2.8 vs 3.1 mo) and a higher number of adjuvant chemotherapy cycles (6 vs 3; P=0.02) among patients who underwent LPD compared with those who underwent OPD. The timely administration of adjuvant chemotherapy has been associated with improved OS in PDAC patients.29 The reduced immunologic and physiologic impact of the minimally invasive approach used in LPD may have contributed to the higher adherence to adjuvant chemotherapy, including the improved ability to receive adjuvant treatment promptly and completely.30 In addition, faster postoperative recovery, evidenced by faster postoperative nasogastric tube removal, earlier initiation of oral food intake, and shorter hospital stay, were protective predictors associated with higher postoperative quality of life and improved long-term survival among LPD patients. Although no independent predictors were observed in the multivariate analysis, the univariate analysis suggested that the potential advantage of faster recovery after laparoscopic surgery might allow patients to achieve better long-term survival. These findings still require confirmation using large-scale trials and underscore the potential advantages of LPD in facilitating faste
留言 (0)