
記住我









Participants were recruited between March 2022 and June 2022 through online advertisements, such as paid social media campaigns promoted in Facebook groups dedicated to parents, as well as through the project’s website, where we had provided information about the study and an easy online sign-up option for interested participants.
Inclusion criteria: (1) be the parent of a child/ adolescent aged between 6 and 14 years old, (2) be able to read and write in Romanian, (3) report elevated child symptoms of anxiety and/or depression symptoms, and (4) have access to the Internet.
Exclusion criteria: child currently undergoing concurrent treatment (psychotherapy sessions, pharmacological treatment).
The required number of participants was calculated a priori using G*Power [34] which indicated that the minimum required sample size was 42 participants based on a medium effect (repeated measures between factors, f = 0.50, α = 0.05, power 0.95, correlation between repeated measures = 0.50).
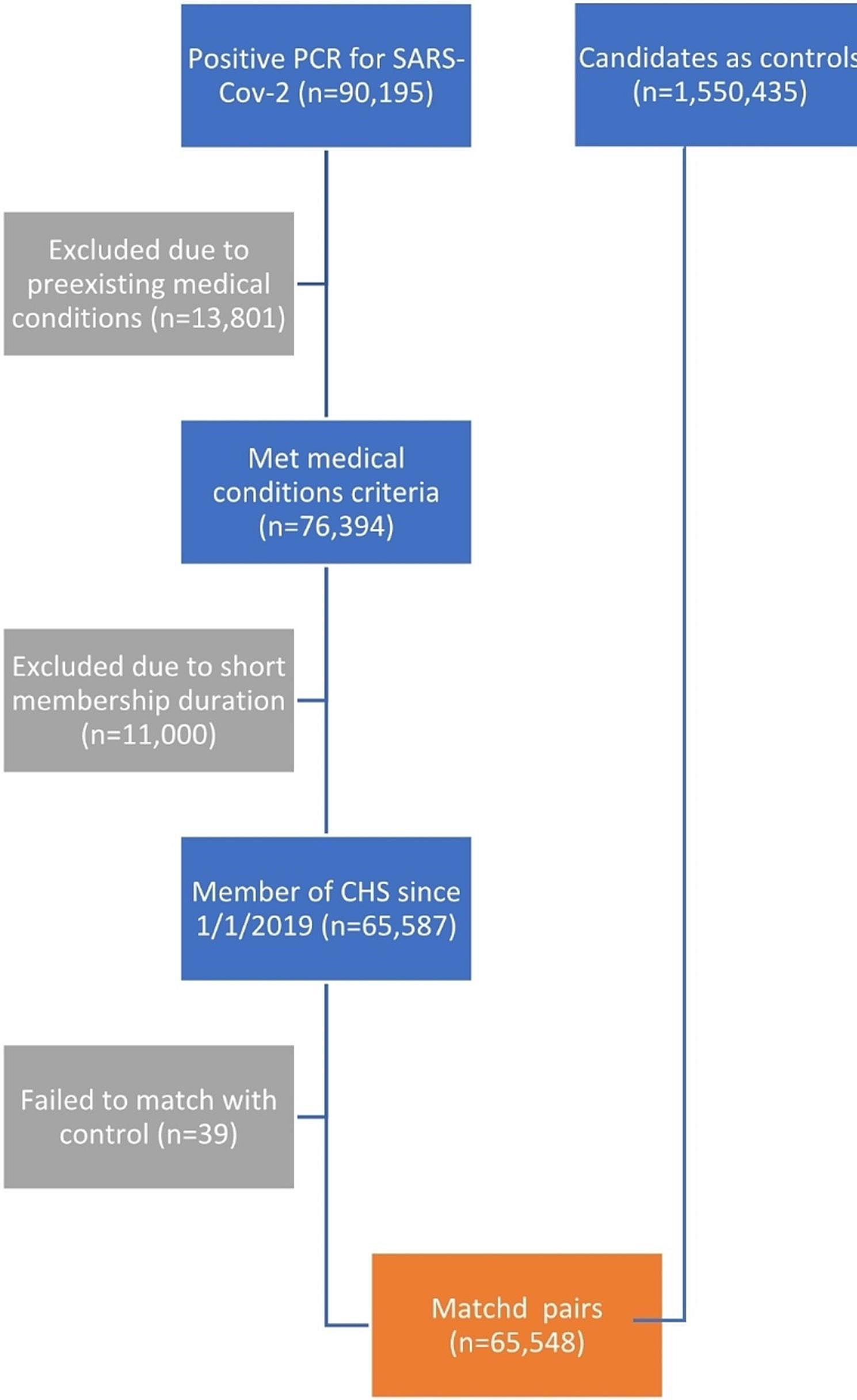
A total of one hundred eleven parents expressed interest in taking part in the study. Forty-two parents (Mage = 39.79, SD = 2.81, 78.6% mothers, MChild age = 10.33, SD = 2.59), whose children exhibited anxiety and depressive symptoms, met the eligibility criteria for the study. Figure 1 depicts the CONSORT diagram outlining the flow of participants throughout the study.
Fig. 1
CONSORT diagram of the pilot randomized controlled trial
ProcedureThe study received approval from the Ethics Committee of the Babeș-Bolyai University. The recruitment of participants took place through online channels, with parents consenting to participate by signing an informed consent form and undergoing a preliminary screening assessment. Eligible participants were randomly assigned in a 1:1 ratio using a random number generator (random.org) in one of the two groups: ParentKIT (n = 21) and the waitlist control group (n = 21), using a computer generated allocation sequence. The randomization procedure was performed by an independent researcher not involved in the study.
Participants assigned to the experimental group received additional support, as a research assistant contacted them by phone to assist in establishing an account on a secure Iterapi platform [35]. After a three-week intervention period, participants were invited to partake in post-intervention evaluations. Participants were not compensated for their participation.
MeasuresDemographic informationA demographic questionnaire was used to collect information about participants, including age, gender, occupational status, marital status, as well as the age and gender of their child.
Primary outcomeChild’s emotional problemsThe parent version of the Strengths and Difficulties Questionnaire for ages 4–17 (SDQ) [36] was used to measure children’s anxiety and depressive symptoms, as reported by parents. It consists of 25 items rated on a three-point Likert scale (0 - Never true, 2 - Very true or very often true). Sample items are: “Often unhappy, depressed or tearful”, “Many fears, easily scared”. Scores can be computed on a scale of total mental health problems or on five subscales (Emotional problems, Conduct problems, Hyperactivity, Peer problems, and Prosocial behaviors). In the current study, we used the emotional problems subscale. The scores for this subscale range from 0 to 10, and higher scores indicate greater emotional problems. Cronbach’s Alpha in the present study was 0.87 for the Emotional problems scale. The psychometric properties of this scale are satisfactory as indicated in a review in which it showed convergent validity and adequate internal consistency for the total scale [37]; it was also previously used with Romanian parents [38].
Secondary outcomesParental distressWe utilized the Patient Health Questionnaire-4 [39] to assess parental anxiety and depressive symptoms. This scale comprises four items, each rated on a 5-point Likert scale ranging from 0 (Never) to 3 (Always). Parents must rate their answers to the next question: “Over the last two weeks, how often have you been bothered by the following problems?”, sample items: “Feeling nervous, anxious or on edge”, “Feeling down, depressed, or hopeless”. Scores can range from 0 to 12, and higher scores indicate greater distress. Previous studies reported excellent psychometric properties. This is supported by a systematic review that analyzes the psychometric properties of PHQ-4, which showed adequate reliability for distress and both anxiety and depression, acceptable stability over time, and demonstrated convergent validity [40]. Cronbach’s alpha in the present study was 0.92.
Parental self-efficacyThe Parental Self-Efficacy Scale (PSES) [41] was employed to evaluate parental self-efficacy concerning parenting practices aimed at reducing anxiety and depression risks among children and adolescents. The scale was obtained from the original author, following which it was translated and adapted into Romanian by the primary author for the purpose of this study. It comprises nine items, each rated on a 4-point Likert scale (1 = Not at all confident, 4 = Very confident). Sample items: “How confident do you feel about your ability to find a balance between being involved in your teenager’s life and encouraging age-appropriate independence?”, “If you noticed a persistent change in your teenager’s mood or behavior, how confident do you feel about your ability to help your teenager seek appropriate professional help?”. Good internal consistency has been reported (McDonald’s omega = 0.91), as well as convergent and concurrent validity [41]. Scores can range between 9 and 36, higher scores indicate a higher self-efficacy. Cronbach’s alpha in the present study was 0.96.
Satisfaction with the programWe assessed satisfaction with the program by administering the Client Satisfaction Scale (CSQ-8) [42]. Responses are rated on a four-point Likert scale, ranging from 1 (Not at all satisfied) to 9 (Very satisfied). Sample items: “How would you rate the quality of the treatment you have received?”, “If a friend were in need of similar help, would you recommend this treatment?”. The answers are rated on a four-point Likert scale. Total scores can range from 8 to 32, higher scores indicating higher treatment satisfaction. This scale showed adequate reliability in other clinical trials investigating the efficacy of Internet-delivered CBT [43]. Cronbach’s alpha in the present study was 0.90.
InterventionParentKIT, an Internet-delivered Intervention, was created based on the fundamental principles of Rational Emotive Behavior Therapy (REBT) [44]. REBT is one of the important tenets of CBT, considered one of the earliest approaches within this treatment orientation [45]. It is considered a transdiagnostic approach [46] and its core mechanisms, namely irrational beliefs, are positively related to both internalizing (e.g., anxiety, depression) and externalizing (e.g., anger) problems, as indicated by the results of a meta-analysis [47].
ParentKIT consists of nine modules delivered over three weeks (see Table 1 for the key aspects covered in each module). The content of the nine modules was developed based on REBT theory and treatment techniques. In REBT, a main concept is irrational beliefs, which are involved in dysfunctional emotions and maladaptive behaviors as proximal causes. Through REBT, parents learn to identify irrational beliefs such as demandingness (“I must comfort my child when he is anxious”), catastrophic thinking (“It’s terrible that my child is anxious”), low frustration tolerance (“I cannot stand that he is so worried all the time”) and global evaluation of human worth (“I’m a bad parent”). In the program, parents learn to support their child with anxiety and depression, not participate in family accommodations, and cope with the child’s distress responses by practicing a rational thinking style. Parents discover ways to assist their children by helping them identify thinking errors (irrational thinking) (see Fig. 2 for a screenshot of the platform, which shows an example exercise designed for parents and children to collaboratively identify irrational beliefs), disputing these cognitions and changing them with their rational counterparts such as preferential, flexible thinking (“I would like my child not to be so anxious, but this does not mean it must happen exactly as I want”), non-catastrophic thinking (“It’s not the worst thing that could happen to me”), frustration tolerance (“I dislike this aspect”), unconditional acceptance of self, others and life (“I am a valuable human being”) instead of rigid thinking.
Fig. 2
Screenshot of an exercise from Module 7 from ParentKIT
In addition to the cognitive restructuring module, parents are provided with strategies to manage anxiety and depressive symptoms (e.g., exposure, behavioral activation, problem solving, relaxation) and techniques to manage their own psychological distress. Parents were instructed to provide assistance and autonomy, create a supportive environment, recognize and validate their child’s feelings, be consistent in providing feedback, identify and prevent obstacles in applying techniques, remove accommodations related to anxiety and depressive symptoms.
Each module adhered to a well-defined structure consisting of various specific sections in each session: module objectives, the central focus of this module, summary, and homework assignment. To enhance the user experience, each module incorporated text and video resources. The video materials included either experts explaining the concepts, rationale for applying a certain technique, and strategies involved in the treatment process or depicting parent-child interactions as they applied the techniques. Furthermore, participants had access to brochures that they could download and print, providing them with additional information and support. Finally, parents could download a diploma for participating in this program.
ParentKIT was facilitated by two psychotherapists undergoing supervision training in Cognitive Behavioral Therapy, who were trained by the first author on the treatment protocol. Therapists provided valuable feedback on the modules and homework worksheets, while also providing support and addressing any queries parents had. The intervention program was designed to be flexible. Parents were given the autonomy to choose when to engage with the content, and each set of modules remained accessible for a period of seven days, allowing parents time to engage with the content before new modules became accessible. During the seven days, parents could read the assigned modules, practice the skills, and complete homework. They could also address their allocated therapist questions regarding clarification using the chat available on the platform. Access to previous modules was not removed, and parents could review previous modules at any time.
Control groupParticipants allocated to the control group had access to the online platform where they completed the assessments. This was a delayed treatment group (waitlist control, WL), with participants accessing the treatment modules after three weeks. Participants were informed that they were in this group and would have access to the intervention after three weeks.
Statistical analysisData were analyzed using RStudio [48]. Hypotheses were tested using a linear mixed model, while missing data was dealt with using multiple imputation by chained equations (MICE), which is the state of the art method to manage missing values [49]. MICE uses chained equations to generate plausible values for missing data based on available data [49]. To incorporate in the estimates the inherent uncertainty of the missing values, the estimates are aggregated across multiple sets of complete data [49]. In our case, the estimates were aggregated across 100 sets of imputed data using Rubin’s rule [50]. The confidence intervals for each estimate were computed based on the aggregated estimate values and their aggregated standard error using the formula: estimate +/- standard error of the estimate multiplied by 1.96 (z-value corresponding to p = .05, two tailed). Mixed models analysis with multiple imputation was performed in RStudio using the R-package “mitml” [51].
For effect size data, we used Cohen’s d [52] where effect sizes are classified into three categories, namely small (d = 0.20), moderate (d = 0.50), large effect size (d = 0.80).
留言 (0)