
記住我




Integrins are transmembrane proteins that are essential in various cellular processes, such as cell adhesion, proliferation, and migration [1]. There are 24 known integrins which differ in their alpha and beta subunit composition [1,2]. Angiogenesis, the formation of new blood vessels from pre-existing ones, is one of the most well-known natural biological processes regulated by integrins. In adults, angiogenesis occurs during wound healing, muscle growth, and in diseases such as arthritis, endometriosis, and neoplasia [1–3]. One of the most extensively studied integrins involved in angiogenesis is αvβ3. αvβ3 integrin expression is a valuable molecular target since it is upregulated in diseased states but relatively quiescent in healthy tissues. Thus, detecting αvβ3 holds potential for diagnostic advances, monitoring therapeutic responses to therapeutic agents, and advancing our understanding of disease mechanisms [4–7].
Maraciclatide (previously known as NC100692) is a synthetic molecule that specifically binds via the Arginine-Glycine-Aspartic (RGD) amino-acid motif to αvβ3/5 integrin receptors (Fig. 1). The molecule includes a chelator for radiolabelling with the readily available imaging radionuclide, technetium [99mTc], enabling visualisation of distribution and accumulation of the tracer after intravenous injection by gamma scintigraphy or SPECT-CT. The diagnostic application of 99mTc-maraciclatide has been applied to human and animal research in detecting bone metastasis, malignant breast tumours, atherosclerotic plaques, rheumatoid arthritis, and peripheral vascular disease [5–10]. 99mTc-maraciclatide has shown particular promise in detecting synovitis in rheumatoid arthritis, resulting in further studies in this and other areas, such as endometriosis, which share similar molecular and cellular processes and genetic associations [7,11–13]. As such, it is essential to understand the radiopharmaceutical safety and biodistribution through human dosimetry studies.
 Fig. 1:
Fig. 1: Diagram of αvβ3 integrin in the active conformation, bound to 99mTc-maraciclatide via the RGD component (created on Biorender).
Materials and methodsIn 2003, a phase 1, placebo-controlled, observer-blinded, randomised, single ascending-dose study was performed. The study aimed to assess the safety of three intravenous levels of maraciclatide and the biodistribution and radiation dosimetry of 99mTc-maraciclatide in healthy volunteers, assessing the potential of 99mTc-maraciclatide as a radiopharmaceutical for diagnostic imaging.
Radiopharmaceutical preparationMaraciclatide is a chelate-peptide conjugate containing an Arginine-Glycine-Aspartic (RGD) amino-acid motif in such a configuration that it specifically binds with nanomolar affinity to the integrin receptor αvβ3. Radiolabelling of the product was performed under aseptic conditions in a phase 1 unit. Maraciclatide (lot FFA082/072-205-2) was originally supplied as lyophilised kits (GE Healthcare, Oslo, Norway). Each vial contained approximately 44 nmol maraciclatide (molecular weight 1697). The lyophilised kits were stored at −20°C. 99mTc labelling was performed by reconstitution with 99mTc-sodium pertechnetate with incubation at room temperature for 20 min. The radiolabelled product could be used for up to 3 h post-reconstitution. The radiochemical purity of the product was tested using HPLC and instant thin-layer chromatography, showing the kit could maintain stable radiochemical purity above 85% for over 4 h (Table 1). All the preparations used in the study had a radiochemical purity ≥85% and reduced hydrolysed technetium (RHT) content below 4%.
Table 1 - Radiochemical stability data from freeze-dried kits (lot FFA082/072-205-2) stored for 3 months at 2–8 °C Storage time (months) Radiochemical purityIn-vivo stability of maraciclatide has previously been demonstrated from urine samples taken from participants in this study using reversed-phase liquid chromatography coupled with an ion-trap mass spectrometer (LC-MS) in order to estimate the amount of intact maraciclatide and any metabolites excreted in the highest dose group (150 micrograms maraciclatide) [14]. Only intact maraciclatide was observed in the urine samples, and no metabolites were detected.
Three chemical dose levels (the chemical amount of maraciclatide administered) were studied, and the way this was achieved for each group is presented in Table 2. The relevant factor increased the other components of the formulation.
Table 2 - The chemical amount of maraciclatide administered to each group, expressed in terms of equivalent vials administered Chemical dose group Reconstitution volume per vial (ml) Number of vials used Total bulk volume (ml) Injection volume (ml) Maraciclatide administered (μg) Maraciclatide as % of 1 kit vial 1 8 1 vial 8 1.6 15 20% 2 2 2 vials 4 2.0 75 100% 3 2 3 vials 6 4.0 150 200%The upper limit of 99mTc activity administered to healthy participants in the present study was 200 MBq (5.4 mCi) to minimise the radioactive dose. In subsequent clinical imaging studies, 740–1100 MBq (20.0–29.7 mCi) has been routinely used.
ParticipantsApproval for this study was obtained from the Quorn Research Review Committee (Independent Ethics Committee (IEC)) according to UK regulations, and informed consent was received from all participants.
Thirty-one participants (19 males and 12 females) were recruited for this study (Table 3), aged 22–64. There were no significant differences in baseline characteristics between groups. The inclusion criteria included ages 18–65 with a normal medical history, physical exam, vital signs, laboratory tests, ECG, and drug screen. The females included in the study were post-menopausal or surgically sterilised with a negative urine pregnancy test. The exclusion criteria included those who were pregnant, lactating or had received another investigational product within 3 months.
Table 3 - Summary of subject numbers recruited, administered and evaluated Subjects recruited Subjects receiving 99mTc-maraciclatide Subjects receiving 99mTc-maraciclatide evaluated for biodistribution and dosimetry Subjects receiving 99mTc-maraciclatide evaluated for safety Subjects receiving placebo and evaluated for safety N = 31 N = 25The study planned to recruit thirty participants divided into three dose groups. Two of the 10 participants were randomly assigned to receive a saline placebo in each dose group. The saline placebo was administered in the same manner as the 99mTc-maraciclatide, including using a lead-shielded syringe and receiving a scintigraphic scan at the same time intervals. The safety assessors were also blinded to administering a placebo or 99mTc-maraciclatide. The scintigraphic camera monitor was shielded to prevent images from being seen, and local radioactivity monitors were switched off to remove any audio signal. Within each group, at least two females and two males in each dose group received 99mTc-maraciclatide.
Administration99mTc-Maraciclatide at the three different maraciclatide chemical dose levels was administered to 25 subjects as a single intravenous administration (Tables 2 and 3). A non-radioactive placebo (saline) was administered to 6 subjects as a single intravenous administration as an equivalent volume to each dose group.
Subjects received 99mTc-maraciclatide under the direct supervision of study personnel. An intravenous line was established, with an intravenous catheter placed into an appropriate vein. Subjects received an intravenous administration of 99mTc-maraciclatide at 2–4 ml per second. After administration, the line was flushed with 5 ml of Sodium Chloride (0.9% w/v). The administration site was evaluated pre- and post-administration for any reaction or extravasation.
One participant in the maraciclatide 75 μg group received a lower chemical dose than intended (47 μg), so an additional participant was enrolled. Data for the participant who received the incorrect chemical dose were excluded from the safety and pharmacokinetics analysis but included in the biodistribution and dosimetry calculations (Table 3).
SafetySafety data on vital signs (heart rate, blood pressure, temperature, and oxygen saturation), electrocardiograms (ECG), laboratory parameters and physical examinations (general appearance, lung, abdominal, cardiovascular, and neurological exam by a qualified clinician) were measured prior to administration, and at multiple time points up to 7 days following administration. Based on clinical assessment, new abnormal or worsening clinical findings were defined as a change from the participant’s normal baseline to abnormal. All abnormal changes were recorded as adverse events (AEs).
Safety assessments were performed by an observer blinded to the administration of the placebo and 99mTc-maraciclatide. A thorough review of safety data was performed before the decision was made to escalate to the higher dose in participants.
Image acquisition and in-vivo activity measurementOn the day of administration before the administration of 99mTc-maraciclatide, a transmission scan was obtained. The counts acquired from a flood or line source with and without the participant on the imaging couch were utilised to calculate body attenuation. Following intravenous administration of 99mTc-maraciclatide, whole-body gamma scintigraphy was performed at 5 min post-administration up to 24 h as described below (section 2.6). Additional anterior and posterior planar images of the chest (45 min and 1 h 45 min, post-administration) and the pelvis (1 h 15 min and 2 h post-administration) were obtained for each participant.
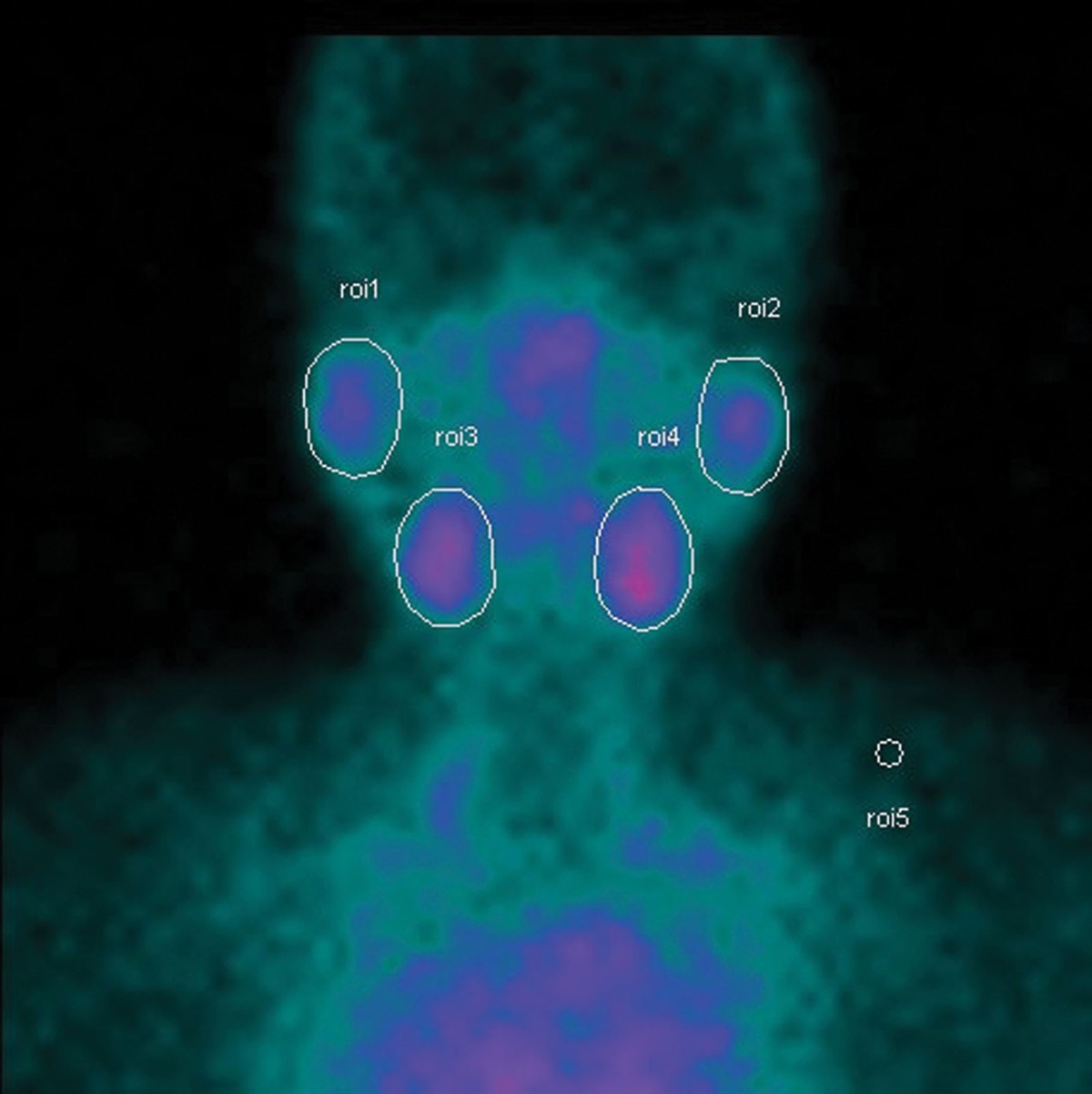
Regions of interest (ROIs) were selected from organs and tissues on the whole-body scintigraphic images showing significant activity uptake. 99mTc activity in ROIs was calculated using the methodology described in Medical Internal Radiation Dose (MIRD) Pamphlet No. 16 [15].
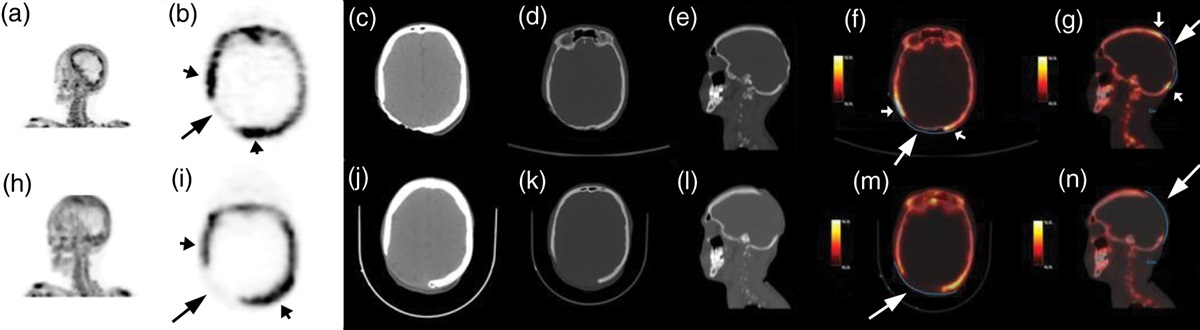
Whole body, chest and pelvic scintigraphic images were assessed by recording distinct areas of focal uptake of radioactivity to determine whether images from healthy volunteers contain foci that could be mistaken as lesions. Focal uptake included any local accumulation of radioactivity seen in the images, excluding expected organ uptake. In contrast, the radiation dosimetry report presented whole organ uptake data. Whole-body scans were assessed by recording the number of distinct areas with focal uptake (with ‘0’ recorded if none were seen).
Measurement of ex-vivo activityTo calculate 99mTc-maraciclatide ex-vivo activity, blood, plasma, urine, and faeces were collected at various time points after administration. Blood and plasma samples were collected at 10 min, 30 min, 1 h, 2 h, 4 h, 8 h, 24 h, 48 h, 72 h, and 7 days post-administration. Concentrations of maraciclatide in plasma were assayed using the LC-MS method [14] (LOQ was 0.5 ng/ml). Urine was also collected at the same time points (if possible) up to 24 h post-administration. Faecal samples were collected as voided for up to 24 h post-administration. Assayed samples for 99mTc-maraciclatide content were then measured using a gamma counter.
Biodistribution and radiation dosimetryThe biodistribution of 99mTc was determined by whole-body conjugate view imaging in conjunction with extracorporeal activity measurements in whole blood, plasma, voided urine, and faeces, as described above. Simultaneous anterior and posterior whole-body images were acquired beginning nominally at 5 min, 15 min, 30 min, 60 min, 90 min, 3 h, 6 h and 12 h post-administration. A final anterior and posterior image pair was acquired at a ninth time-point between 21 and 24 h post-administration. Quantitative analysis of the incorporated data at multiple time points yielded biodistribution data consisting of activity in 10 specified organs or tissues [brain, salivary glands, thyroid gland, lungs, heart, spleen, liver, gallbladder, gastrointestinal (GI) tract and urinary bladder]. The remaining 99mTc activity in other tissues was grouped within a ‘remaining tissues’ category. For each organ or tissue of interest, the 99mTc activity was decay-corrected to the administration time and normalised to the injected activity. The temporal variation of this normalised and decay-corrected activity was then fit by one of several analytical functions, which was then integrated to yield the cumulated activity for that organ normalised to the injected activity.
The mean absorbed doses per unit injected activity to 24 target organs were evaluated from this matrix of normalised cumulated activity values, using the MIRD schema [15], for a 70-kg adult human. The cumulated activity in the urinary bladder contents and voided urine was calculated using a dynamic urinary bladder model for a 3.5-h voiding interval. Cumulative activities in the GI tract were calculated using a dynamic model that assumed that activity enters the GI tract solely through hepatobiliary drainage. At early times (up to 90 min) post-administration, the GI tract exhibited a diffuse uptake of 99mTc. At later times, it was possible to identify the 99mTc associated with the GI tract as predominantly that in the luminal contents. The overall time course of 99mTc activity in a ROI set over the GI tract was typically that of an initial rapid decrease which then slowed to approach the amount present in the luminal contents. This observation was considered to be due to an initial rapid uptake and subsequent tissue clearance of 99mTc from the GI tract walls combined with the slow introduction of 99mTc into the GI contents via hepatobiliary transport. The activity in the luminal contents was isolated by first modelling the GI tract wall tissue clearance by the renormalised time course of activity measured in a ROI set over a region of soft tissue (the quadriceps femoris in one leg). This modelled GI tract wall tissue clearance was then subtracted from the measured activity in the GI tract wall and contents to yield the activity in the luminal contents, which displayed the expected asymptotic increase. The ED per unit injected activity was subsequently calculated from the ensemble of organ-absorbed dose values.
ResultsUnless otherwise specified, all values presented are the mean with uncertainties given as one SD. All activities have been decay-corrected to the time of administration and are normalised to the injected activity.
ParticipantsAll enrolled participants completed the study (24 received the protocol-stipulated quantity of maraciclatide, 1 received an incorrect amount of maraciclatide, and 6 received a placebo), and their data were analysed (Tables 3–5). Female participants were enrolled into all dose groups and into the placebo groups. No significant differences were seen between the dose groups/placebo except for the mean age of the participants in the 150 μg dose group. This was due to the inclusion of more male participants, who were generally younger than the females in the study.
Table 4 - Participant characteristics recorded at baseline Characteristic Maraciclatide 15 μgN = 6
Age Mean (SD) 49.6 (12.1) 49.0 (8.4) 34.3 (11.7) 47.8 (12.6) Range 29–64 43–64 22–56 25–61 Height Mean (SD) 169.8 (6.5) 168.1 (7.7) 169.8 (9.7) 170.2 (9.4) Range 157–177 156–177 152–180 153–180 Weight Mean (SD) 71.9 (9.1) 73.6 (7.7) 75.9 (11.4) 69.7 (9.4) Range 69–90 66–85 58–91 58–85 BMI Mean (SD) 24.9 (2.7) 26.0 (1.5) 26.3 (3.2) 24.1 (3.0) Range 21–29 24–28 21–33 20–28 Gender Male 4 5 6 4 Female 4 3 2 2 Race Black 1 0 0 0 Caucasian 7 8 8 6N = 6
N (%)
The radiochemical purity was above 92%, and the RHT was not above 1.7% (Table 6) for all subjects.
Table 6 - Summary of the radiochemical purity of 99mTc-maraciclatide, quantity of RHT, the injected activity and the volume administered Dosing parameter Maraciclatide 15 μgThe injected radioactivity was similar across all dose groups, the mean injected activity being 183 ± 8 MBq (range: 169–198 MBq). One female participant received 1.25 ml (47 μg) of 99mTc-maraciclatide instead of 2 ml (75 μg dose). As the radioactive dose was within the expected clinical range, data for this participant was included in the biodistribution and internal radiation assessment.
Safety99mTc-maraciclatide was safe and well tolerated. There were no deaths, and no serious AEs (SAEs) were reported in the study (Table 7). Among the 24 participants receiving a protocol-stipulated dose of 99mTc-maraciclatide, 17 (71%) participants experienced 31 non-serious AEs. However, only 7 (23%) were deemed by investigators to be related to maraciclatide, the majority of which were mild in intensity, and none resulted in participant withdrawal. Of the remaining AEs not attributed to maraciclatide, 10 were attributed to procedural complications, 5 were due to a pre-existing medical condition, and 6 were due to ‘other causes’ (including sleep deprivation and the effect of multiple blood draws). In the placebo group, 3 (38%) of the AEs were attributed to the placebo, 3 due to a procedural complication, 1 due to a pre-existing medical condition and 1 due to ‘other cause’ (lack of bowel movement).
Table 7 - Recorded adverse events MedDRA body system
留言 (0)