
記住我



Anal canal adenocarcinoma (AAC) is a rare histological subtype of anal carcinoma, accounting for 5% to 17% of all anal cancers.1–3 Compared with the most common subtype (squamous cell carcinoma), AAC seems to have more aggressive features and decreased survival.3,4 In one historic series of 21 patients with anal adenocarcinoma, both the crude 5- and 10-year survival rates were only 4.8%.1 Although some previous studies advocated for definitive chemoradiotherapy (CRT), similar to the treatment of anal squamous-cell carcinoma,5–7 the appropriate treatment for AAC, as advised by the current National Comprehensive Cancer Network (NCCN) guidelines, is management per the rectal adenocarcinoma treatment paradigm.8 In reality, many do not consider this an anal cancer and more a misclassified rectal cancer. The introduction of total neoadjuvant therapy (TNT) as a treatment approach to rectal adenocarcinoma has increased the rates of both clinical and pathologic complete response, resulting in excellent long-term oncologic outcomes. The recently published OPRA trial9 showed that organ preservation is achievable in half of the patients with rectal cancer treated with TNT and that CRT combined with consolidative chemotherapy or induction chemotherapy may be an appropriate strategy to maximize clinical complete response (cCR) rates.10 Controversy exists regarding the role of surgery in AAC, with a recent National Cancer Database analysis suggesting improved overall survival with the incorporation of surgery into the management of anal adenocarcinoma.11 Because AAC is such a rare occurrence, it is not feasible to conduct large-scale prospective randomized controlled trials to study the nature of this disease. We sought to analyze the patterns of care and the oncologic outcomes of AAC in the era of the TNT and watch-and-wait (W&W) approach to better define the optimal treatment strategy of this rare cancer.
PATIENTS AND METHODS Patient PopulationPatients with rectal cancer treated at Memorial Sloan Kettering (MSK) between 2004 and 2019 were extracted from a prospectively maintained institutional database. Two investigators individually reviewed each case and identified a study population of patients with biopsy-proven anal adenocarcinoma, defined as tumors with an epicenter located between the anal verge and ≤2 cm above the dentate line, and based on MSK Cancer Center’s treating surgeon’s review and assessment.1,12 Patients who were treated elsewhere (seen as a second opinion at our institution) and those returning with recurrence after 2004 were excluded. A comprehensive medical report review for clinical and tumor characteristics, including those related to preoperative imaging and endoscopy findings, was performed. The locoregional staging was based on endorectal ultrasound or MRI. Clinical T stage (cT) was classified as Tis, cT1 to 4, according to preoperative imaging, and as cTx when these data were missing or when the primary tumor was not visualized. The study was approved by the institutional review board of MSK, and a waiver of informed consent was obtained.
Neoadjuvant and Adjuvant Therapy RegimensCRT consisted of 25 to 28 fractions of 1.8 Gy radiation dose with administration of concurrent, continuous infusion of fluorouracil or oral capecitabine. Patients generally received a radiation dose of 45 Gy with a sequential or integrated boost of 5 to 11 Gy to the tumor. Patients treated with CRT were recommended to receive additional chemotherapy as adjuvant treatment for a total of 3 to 4 months in accordance with the guidelines of the NCCN.8 In the TNT group, induction chemotherapy,13,14 consisting of 8 cycles of folinic acid, fluorouracil, and oxaliplatin, was followed by long-course CRT as described above. An alternative regimen was long-course CRT followed by consolidation chemotherapy consisting of 8 cycles of folinic acid, fluorouracil, and oxaliplatin. The third and least common neoadjuvant regimen was chemotherapy or CRT only.
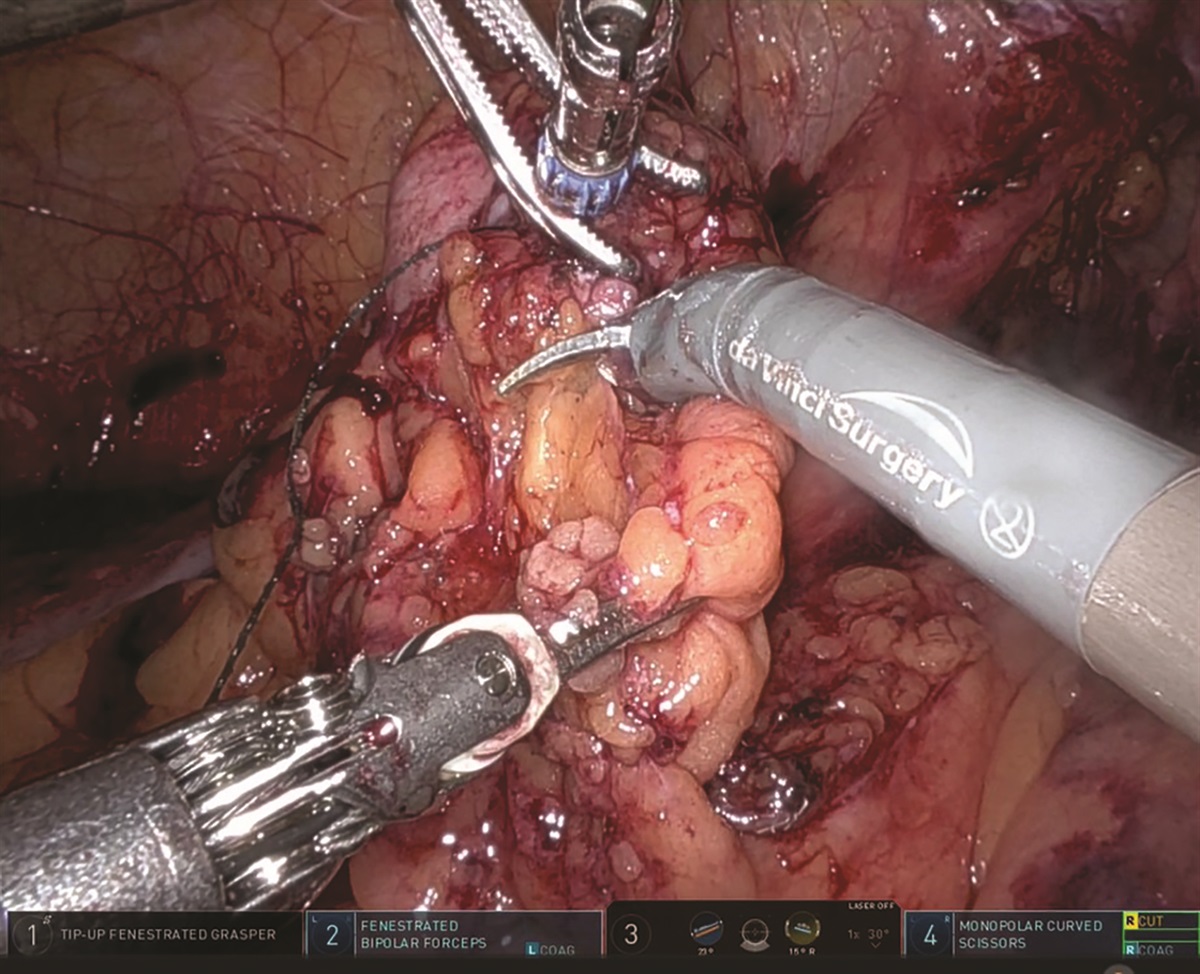
Surgical TechniquePatients with cCR at the completion of neoadjuvant therapy were given the option to enter a W&W protocol to preserve the rectum.15 Patients with cCR who chose surgery, patients without a cCR at restaging, and patients in whom the tumor regrew during W&W underwent total mesorectal excision surgery. Some of the patients underwent local excision or declined resection.
Pathologic AnalysisPathology data were collected from analyses of resection specimens performed shortly after surgery. The NCCN guidelines recommend treatment of anal adenocarcinoma according to the paradigm established for rectal adenocarcinoma, despite substantial differences in their staging paradigms. In anal adenocarcinoma, T stage was previously determined by either tumor diameter or by depth of invasion as per rectal adenocarcinoma. In our institution, each anal tumor was evaluated in accordance with standard protocols for rectal cancer pathology.16
Follow-upPatients were seen within 1 month after resection, then every 3 to 4 months for the first 2 years, every 6 months for the next 3 years, and annually thereafter. Clinical examination was generally performed at each follow-up visit; serum CEA was measured at each visit. CT scans were obtained on the basis of individual follow-up regimens (generally every 6–12 months). PET scans were selectively used when abnormalities on axial imaging raised the question of recurrence. Regrowth, the return of the tumor at the previous tumor site after achieving cCR, was possible in patients who underwent nonoperative management with W&W; for all other groups, local recurrence was defined as the first clinical, radiologic, and/or pathologic evidence of the return of cancer of the same histologic type within the same location. Distant recurrence was defined as clinical, radiologic, and/or pathologic evidence of systemic disease outside the pelvis at sites such as the liver, lungs, and para-aortic region. Local failure included an unresectable primary tumor after neoadjuvant treatment, local recurrence after a primary R0 to 1 resection, or positive margins in the primary tumor resection.
Statistical AnalysisWe performed baseline demographic comparisons using ANOVA for continuous factors and 2-sided χ2 tests for categorical variables. Overall survival estimates for the sample population and treatment subgroups were determined using the Kaplan-Meier method. Differences in survival across treatment subgroups were determined using the log-rank test. In all cases, a p value of <0.05 was considered statistically significant. Statistical analysis was performed using R software (version 4.2.1).
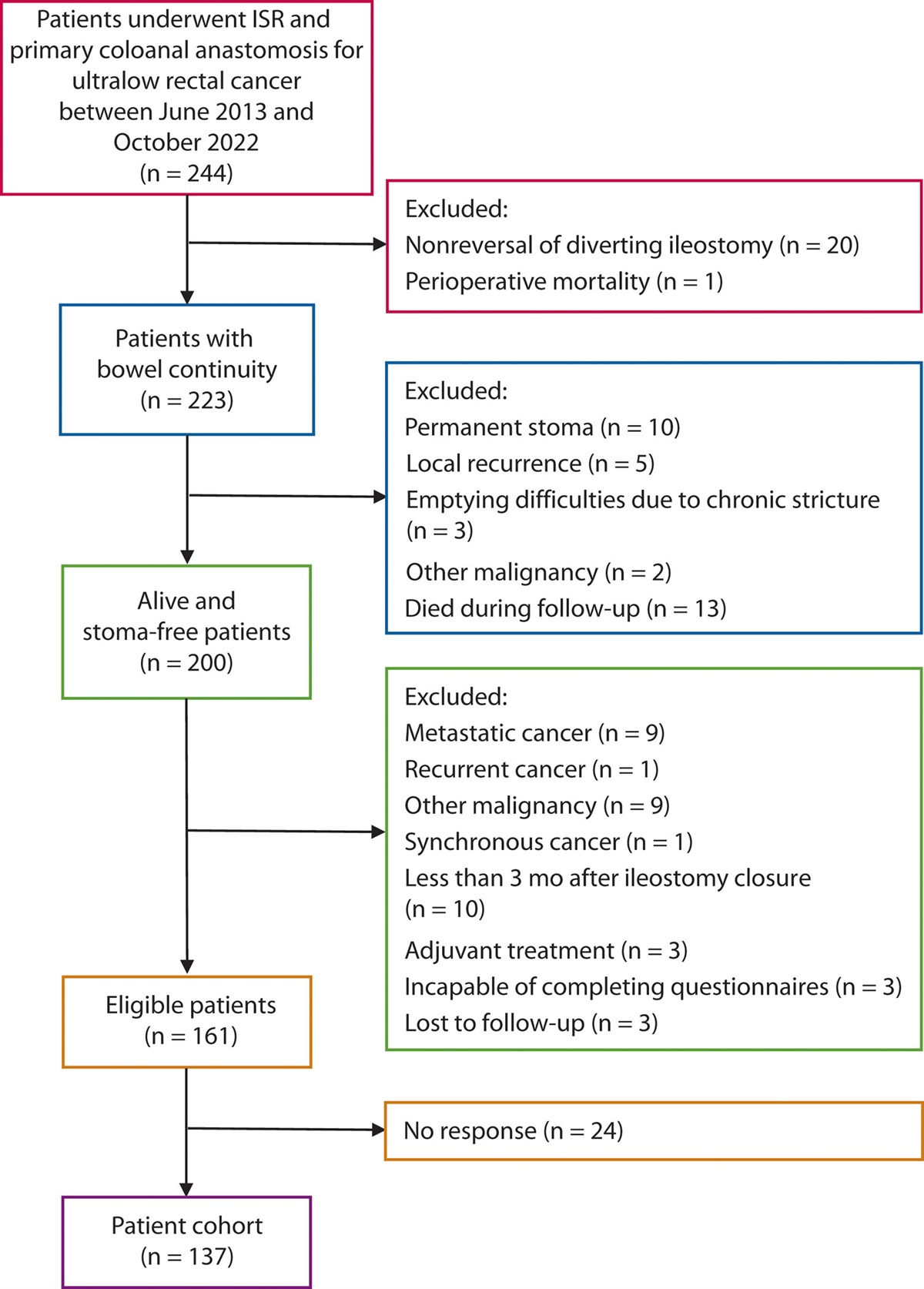
RESULTS Baseline Patient and Tumor CharacteristicsOf the 1446 patients with anal carcinoma treated at our institution between 2004 and 2019, 176 were diagnosed with anal adenocarcinoma. Patients with stage IV disease, a second primary cancer, and extramammary Paget disease at the time of diagnosis were excluded. Seventy patients were included in the final analysis (Fig. 1). Thirty-four of these patients were staged using MRI, whereas 35 underwent an endoscopic ultrasonography and 1 had unreported imaging modality. The median distance from the anal verge was 0 cm (interquartile range [IQR], 0–1.55). The anal tumor involved the anal sphincter complex in 39 patients, whereas 9 patients did not have sphincter involvement and 22 patients had unreported sphincter invasion.
 FIGURE 1.:
FIGURE 1.: Exclusion criteria and treatment groups. CRT = chemoradiotherapy; TNT = total neoadjuvant therapy; W&W = watch and wait.
Fifty-four patients (77%) who received neoadjuvant therapy were isolated and divided into 2 groups according to their treatment strategy: TNT (n = 30; 43%) and chemotherapy or CRT alone (single neoadjuvant modality [SNM] therapy, n = 24; 34%). Sixteen patients (23%) underwent upfront surgery. The distribution of clinical stages among the 3 cohorts was imbalanced (p = 0.010), namely a majority of patients (n = 11) who underwent upfront surgery had clinical stage I disease (69% vs 20% and 29% in the TNT and SNM groups). Conversely, both groups that received neoadjuvant therapy had a greater proportion of patients with stage III disease than the upfront surgery group (Table 1). For this reason, patients in the upfront surgery group were analyzed and described separately from those who had neoadjuvant therapy.
TABLE 1. - Patient demographics and baseline tumor characteristics TNT (N = 30) SNM (N = 24) Upfront surgery (N = 16) Baseline characteristics n % n % n % p Age, y, median/IQR 63 53–71 66 48–75 62 53–80 0.78 Sex 0.41 Male 15 50.0 16 66.7 8 50 Female 15 50.0 8 33.3 8 50 Race/ethnicity 0.57 White 26 86.7 17 70.8 12 75.0 Hispanic or Latino 3 10.0 2 8.3 1 6.3 Black 1 3.3 4 16.7 2 12.5 Race other or ethnicity not reported 0 0.0 1 4.2 1 6.3 History of IBD 4 13.3 6 25.0 0 0.0 0.085 RT for prostate cancer 0 0.0 1 4.2 1 6.3 0.45 RT for cervical cancer 0 0.0 1 4.2 0 0.0 0.37 HIV 1 3.3 0 0.0 2 12.5 0.15 CRC 1 3.3 0 0.0 0 0.0 0.51 Diagnosis Positive baseline inguinal nodes 8 26.7 6 25.0 1 6.3 0.24 Clinical stage 0.01 Stage I 6 20.0 7 29.2 11 68.8 Stage II 5 16.7 7 29.2 3 18.8 Stage III 17 56.7 10 41.7 1 6.3 Indeterminate 2 6.7 0 0.0 1 6.3 Differentiation 0.38 Well differentiated 1 3.3 3 12.5 0.0 0.0 Moderately differentiated 22 73.3 14 58.3 13 81.3 Poorly differentiated 7 23.3 6 25.0 2 12.5 Not reported 0 0.0 1 4.2 1 6.3 LVI 0.0015 Positive 6 20.0 2 8.3 8 50.0 Negative 10 33.3 15 62.5 8 50.0 Not reported 14 46.7 7 29.2 0 0.0 Signet ring morphology 0 0.0 5 20.8 0 0.0 0.0057 Mucinous histology 7 23.3 12 50.0 6 37.5 0.12 MMR 0.80 Proficient 12 40.0 8 33.3 5 31.3 Not reported 18 60.0 16 66.7 11 68.8CRC = colorectal cancer; IQR = interquartile range; LVI = lymphovascular invasion; MMR = mismatch repair; RT = radiotherapy; SNM = single neoadjuvant modality; TNT = total neoadjuvant therapy; W&W = watch and wait.
In the TNT group, 21 patients (70%) received induction chemotherapy followed by CRT, and 9 patients (30%) had CRT followed by consolidative chemotherapy. Most of the patients in the SNM group received neoadjuvant CRT alone (n = 21; 88%) rather than chemotherapy alone (n = 3; 13%). Those who received chemotherapy alone were either not candidates for CRT because of previous pelvic radiotherapy or refused CRT.
Ten patients had a history of IBD, including 7 patients who had fistula-associated AAC because of Crohn’s disease, and underwent neoadjuvant therapy. Half of these patients presented with clinical stage III disease, followed by 3 patients with stage II and 2 patients with stage I disease. Four patients underwent TNT and none of them were offered W&W. Two patients underwent TNT followed by pelvic exenteration. Six patients received neoadjuvant CRT (n = 5) or chemotherapy (n = 1) alone, followed by surgery. Five patients received adjuvant chemotherapy as well.
None of the patients with an available mismatch repair (MMR) status were MMR deficient (MSI-high). Intact MMR status (MSI-low) was identified in 12 (40%) TNT patients and 8 (33%) SNM patients. More patients in the SNM cohort expressed signet ring morphology in their tumors than in the other 2 groups, but mucinous histology was similarly observed in all 3 groups. An apparent difference in lymphovascular invasion existed among the 3 cohorts (p = 0.002), with the upfront surgery cohort having a greater proportion of patients with lymphovascular invasion positivity than the SNM cohort. Further details about the baseline disease characteristics are provided in Table 1.
Treatment OutcomesThe median length of follow-up was 58.1 months (IQR, 35.9–89.2 months) from the time of diagnosis. Eighteen patients (60%) in the TNT group achieved cCR and were able to enter W&W (Fig. 1). Four patients (22%) who continued to W&W after receiving TNT had completion abdominoperineal resection (APR) for tumor regrowth. Within the TNT group, 1 patient (3%) underwent multiple local excisions (LEs), and 11 (37%) underwent APR (Table 2). Two patients with clinical stage III disease attained pathologic complete response (pCR). Seven patients (23%) who underwent TNT and surgery received adjuvant chemotherapy for reasons including R1 resection, incomplete neoadjuvant treatment, or extensive disease at the time of surgery (usually before 2010).
TABLE 2. - Most definitive treatment outcomes Treatment outcome TNT (N = 30) SNM (N = 24) n % n % p Initial surgery 0.0088 LE 1 3.3 2 8.3 APR 9 30.0 17 70.8 Pelvic exenteration 2 6.7 0 0.0 Salvage surgery 0.51 LE 1 3.3 1 4.2 APR 4 13.3 1 4.2 Final pathologic stage 0.22 pCR 2 6.7 4 16.7 In situ 1 3.3 0 0.0 I 5 16.7 5 20.8 II 4 13.3 5 20.8 III 4 13.3 5 20.8 IV 0 0.0 1 4.2 Indeterminate or W&W 14 46.7 4 16.7 Tumor regression grade 0.18 <10% tumor remaining 5 16.7 8 33.3 10%–50% tumor remaining 5 16.7 4 16.7 >50% tumor remaining 3 10.0 5 20.8 W&W 14 46.7 4 16.7 Not reported 3 10.0 3 12.5 Oncologic events (total) 13 43.3 14 58.3 0.41 Local regrowth 4 13.3 1 4.2 0.50 Locoregional recurrence 5 16.7 5 20.8 0.70 Distant metastasis 6 20.0 11 45.8 0.083 Progression of disease 0 0.0 1 4.2 0.91APR = abdominoperineal resection; LE = local excision; pCR = pathologic complete response; SNM = single neoadjuvant modality; TNT = total neoadjuvant therapy; W&W = watch and wait.
The SNM group included 5 patients who achieved cCR after CRT (n = 4) or chemotherapy (n = 1) alone and continued to W&W. One (20%) of these patients had tumor regrowth and underwent LE. Nineteen patients in the SNM cohort underwent either LE (n = 2; 11%) or APR (n = 17; 89%). Four patients (17%) presented with clinical stage I (n = 2) or stage II (n = 2) tumors with APRs with pCR on final pathology. One LE patient further developed local recurrence and required a completion APR. Fourteen patients (58%) continued to receive adjuvant CRT (n = 1) or chemotherapy (n = 13).
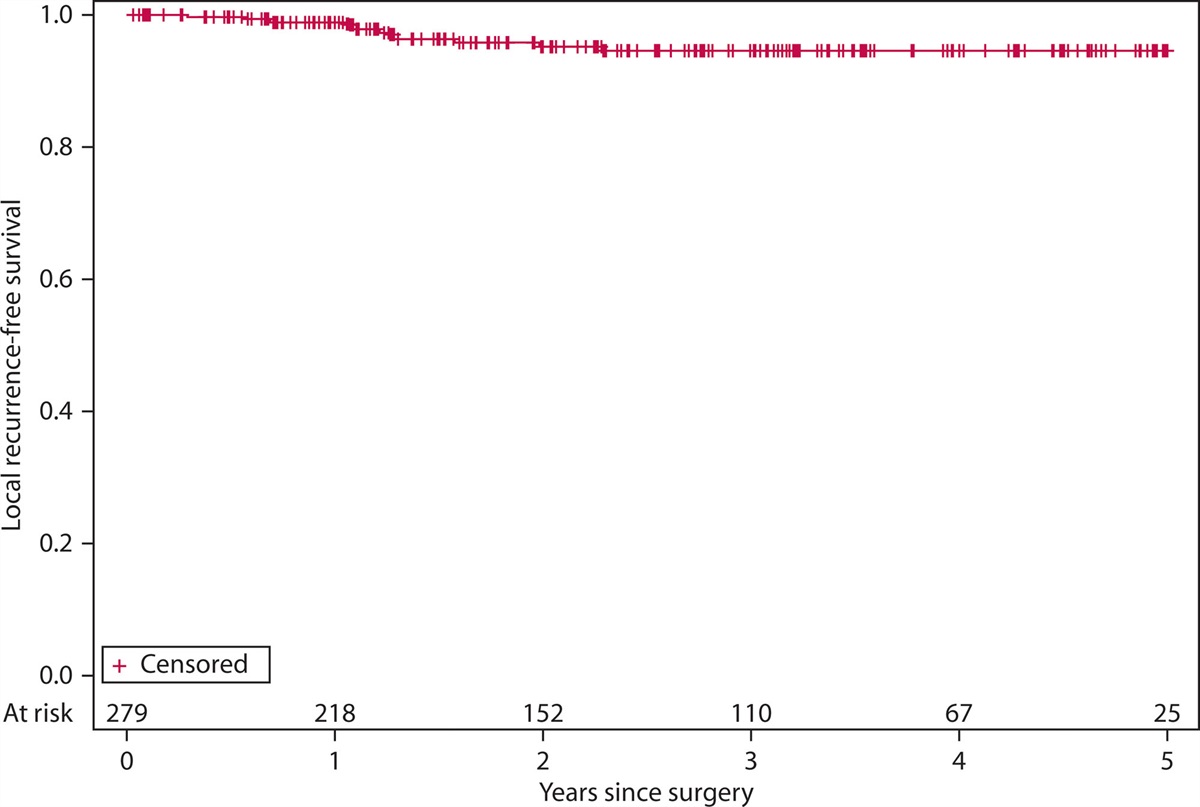
When evaluating the total number of patients who were managed by W&W (n = 23; 33%) in the 70-patient cohort, 19 of them avoided an APR, yielding an organ preservation rate of 83%. Furthermore, the local regrowth and local failure rates in all the patients who ultimately proceeded to W&W were 22% (n = 5) and 13% (n = 3).
The 10 patients with a history of IBD did not achieve cCR and underwent either LE (n = 1) or APR (n = 9). On final pathology, 3 patients obtained a pCR, 1 of whom received TNT. Of note, half of the patients with IBD were treated before the era of W&W; therefore, the time between neoadjuvant therapy and restaging was shortened and they proceeded to surgery. Half (n = 5) of the patients with IBD developed a local (n = 3) or distant (n = 3) recurrence, with 1 patient experiencing both.
Oncologic OutcomesCompared with the SNM cohort, patients who underwent TNT were more likely to be managed by W&W (p = 0.009). The patients who received TNT had a higher rate of organ preservation (n = 15; 50%) than those who underwent SNM (n = 6; 25%), although the difference was not statistically significant (p = 0.11). The local failure rates in the TNT and SNM cohort were similar, at 17% (n = 5) and 29% (n = 7).
The 5-year survival rate for the overall population was 71% (95% CI, 60%–83%), including 61% (95% CI, 42%–88%) for TNT patients and 65% (95% CI, 48%–88%) for SNM patients (Fig. 2). The TNT group showed no significant difference in overall and recurrence-free survival when compared with the SNM group (Fig. 3). The patients who underwent TNT had a 5-year recurrence-free survival of 55% (95% CI, 39%–79%) compared with 30% (95% CI, 15%–58%) in the SNM group. There was no significant difference in time to recurrence (p = 0.200). Distant metastasis occurred in 20% of TNT patients (n = 6) and 49% of SNM patients (n = 11), whereas distant-metastasis–free survival at 5 years was 51% (95% CI, 33%–79%) and 40% (95% CI, 24%–68%; Fig. 4). The total sample of patients who entered W&W (n = 23), had a 5-year recurrence-free survival of 52% (95% CI, 32%–84%) and a 5-year distant-metastasis–free survival of 71% (95% CI, 54%–94%).
 FIGURE 2.:
FIGURE 2.: Overall survival of patients who underwent TNT versus SNM therapy. CRT = chemoradiotherapy; SNM = single neoadjuvant modality; TNT = total neoadjuvant therapy; W&W = watch and wait.
 FIGURE 3.:
FIGURE 3.: Recurrence-free survival in patients who received TNT versus SNM therapy. SNM = single neoadjuvant modality; TNT = total neoadjuvant therapy.
 FIGURE 4.:
FIGURE 4.: Distant-metastasis–free survival of patients who received TNT versus SNM therapy. SNM = single neoadjuvant modality; TNT = total neoadjuvant therapy.
Upfront Surgery PatientsA subset of 16 (23%) patients within the total cohort underwent surgery before receiving chemotherapy or radiation. Three patients (19%) initially had APRs, whereas 13 (81%) had LEs, 6 of whom required completion APR. Five patients (31%) had local recurrences and 2 (13%) developed distant metastases. The 5-year recurrence-free survival was 56% (95% CI, 37%–87%), whereas distant-metastasis–free survival was 83% (95% CI, 65%–100%). The overall survival for the upfront surgery patients was 88% (95% CI, 73%–100%) at 5 years.
DISCUSSIONIn this retrospective series, almost a third of patients with anal adenocarcinoma treated with neoadjuvant therapy achieved a cCR. The proportion of cCR was higher after receiving TNT (60%) compared with single-neoadjuvant modality therapy (20%). All patients with IBD-associated anal adenocarcinoma required surgery. Tumor regrowth in patients who achieved a cCR was 22%, comparable to historical figures for rectal adenocarcinoma.
Anal adenocarcinoma is rare and experience from previous series is limited. Although practice-pattern heterogeneity exists as the treatment of anal adenocarcinoma evolves, most data support an aggressive treatment approach, including trimodal therapy.1 Nonoperative management is well established for rectal adenocarcinoma, and by extrapolation, the same treatment goal is often implemented at our institution for patients with AAC who have a cCR after TNT. This study examined the oncologic outcomes of a cohort of patients with AAC who received different treatment modalities, including nonoperative management, over a 15-year period. The results of this study suggest that TNT and nonoperative management, like in rectal cancer, can be considered in AAC patients, with acceptable regrowth rates, organ preservation rates, overall survival, and recurrence-free survival.
Most patients in this study were treated with neoadjuvant therapy. The proportion of patients who were able to continue to W&W was significantly higher after receiving TNT compared to CRT or chemotherapy alone. Patients treated with the contemporary TNT protocol who achieved cCR and were managed with W&W yielded a regrowth rate (22%) consistent with the tumor regrowth rate of 27% to 40% in patients with rectal cancer who were treated nonoperatively in the OPRA trial.9 Differences in 5-year overall and recurrence-free survival rates between the TNT and SNM approaches, were not statistically significant; however, an APR was avoided in 50% of patients who received TNT and 83% of the total number of patients who continued to W&W. Although earlier studies described local failure rates approaching 50% in patients with AAC who received multimodal therapy, including CRT and either APR or LE,3,5,17–20 our cohort rendered a lower rate of local failure. These results may suggest the oncological safety of the W&W protocol in patients with AAC.
Surgery has been considered imperative in the management of AAC, leading to an improvement in median survival from 42 to 45 months to 79 to 87 months, as published by 2 National Cancer Database studies in 2019.11,21 However, information pertaining to the intent of treatment, salvage therapy outcomes, or specific treatment regimens in these studies was lacking. The disease-free survival reported in recent studies varied from 21% to 58% according to the treatment modality.2 Moreover, Lukovic et al12 previously reported a 5-year cumulative incidence of distant metastasis reaching 30% in patients treated with multimodal treatment. Although metastasis is common in this subtype of anal cancer, our results included acceptable 5-year distant-metastasis–free and recurrence-free survival among the TNT cohort and patients who entered W&W.
Examples of nonoperative management of patients with IBD-associated AAC are almost nonexistent. In the current study, half of the patients with IBD-associated AAC were treated in the era of TNT. However, none of them
留言 (0)