
記住我



Enhanced recovery protocols (ERP) are well supported in the literature and result in faster GI recovery, decreased length of stay (LOS), and fewer postoperative complications after colorectal surgery.1 Same-day discharge (SDD) pathways represent the evolution of ERPs by optimizing the elements of perioperative care that keep patients hospitalized after colorectal surgery.2,3 After an initial series from France, studies from Canada and the United States have demonstrated its feasibility in different settings and with different modalities of postdischarge care.4–6
The implementation of SDD protocols after colectomy requires a multifaceted approach, including advanced surgical techniques, opioid-sparing analgesia to promote return of bowel function, early remote follow-up methods, and patient-related factors. The objective of SDD is for patients to be discharged on the same calendar day as their surgery with an uneventful early postoperative course. The apprehension regarding SDD is that patients may develop a complication at home that could have been identified early in the postoperative period were they admitted to the hospital. However, most studies have demonstrated similar postoperative morbidity and mortality rates to those observed with standardized ERPs.4,5,7 Nevertheless, a proportion of intended SDD patients are unable to be discharged on the day of surgery or require an early postdischarge emergency department (ED) visit.3 Many of the barriers to SDD implementation focus on the potential for SDD failure and/or early readmission, which may result in negative clinical and economic outcomes.2 Identification of factors predictive of SDD success or failure may provide early “warning signs” for providers to keep patients hospitalized instead of discharged on the day of surgery, thus decreasing several of the barriers to SDD implementation by increasing the chances of success. Therefore, the primary objective of this study was to identify patient-related or perioperative factors that impact SDD success and failure.
MATERIALS AND METHODS SettingThis prospective study was performed at a single university–affiliated colorectal specialty referral center from January 2020 to March 2023. Approval was obtained by the McGill University Health center institutional research ethics board.
PatientsAll adult patients undergoing elective minimally invasive colectomy or loop colostomy/ileostomy closure by a fellowship-trained colorectal surgeon at our institution were eligible for recruitment. Patients undergoing stoma creation, open procedures, multivisceral resection, or anorectal procedures without an abdominal component were not eligible. Patients were excluded if they had significant comorbidities including insulin-dependent diabetes, had chronic renal failure precluding nonsteroidal anti-inflammatory drug (NSAID) usage, needed dialysis, or had respiratory or cardiac comorbidities that required prolonged postoperative monitoring. Individuals were also excluded if they had chronic pain requiring daily opioid consumption. Patients were considered eligible if they had adequate home support during the immediate postoperative period, defined as live-in support for at least 72 hours. Individuals who lived >50-km drive from the Montreal General Hospital were not eligible. All patients were required to understand verbal and written English or French, own a smartphone, and be comfortable downloading and using mobile applications. Patients meeting all inclusion criteria were approached in the colorectal surgery clinic for participation in the SDD program. For those eligible, SDD was offered from Monday to Friday, and patients were discharged directly home from the postanesthesia care unit (PACU).
InterventionAt the time of study enrollment, participants were offered a digital health smartphone application (Caresense, MedTrak Inc., Conshohocken, PA) as a method of postdischarge follow-up—a commercially available customizable smartphone application compliant with the Health Insurance Portability and Accountability Act of 1996. The application included educational material, daily health check questionnaires, and postdischarge direct communication with the health care team. Health check questionnaires occurred until postoperative day (POD) 7, and any concerning answers would be brought to the direct attention of the treating surgical team. Patients were able to communicate with the surgical team through a chat function monitored from 7 am to 5 pm, 7 days/week, by a surgical team member (either the treating colorectal surgeon or a resident physician). Communications sent outside of these hours were addressed the following day through the chat function, a telephone call, or a requested in-person clinic visit. Patients were instructed to present to the ED if worrisome symptoms arose or they were unable to contact the surgical team.
Patients who qualified as SDD candidates were approached during their preoperative clinic visit. Patients received information regarding the program, including discharge criteria, preference for opioid-sparing analgesia as first-line pain control, and postoperative monitoring through the Caresense application. Those enrolled in the program were scheduled as the first case of the day. The anesthetic regimen used followed a standardized institutional protocol and ERP guidelines. Surgical procedures were performed according to each surgeon’s technique. All ileocolic anastomoses were performed intracorporeally. The distal transection was performed intracorporeally for colorectal anastomosis, and a small Pfannenstiel incision was made (to extract the specimen and insert the anvil), pneumoperitoneum was reestablished, and the anastomosis was done under laparoscopic guidance. A bilateral transversus abdominis block with 40 mL of 0.25% bupivacaine and 10 mg of dexamethasone was administered by the surgical (nonimage guided) or anesthesia team (ultrasound-guided technique) to all patients undergoing colectomy. Patients were monitored postoperatively in the PACU until discharge. Patients were discharged from the PACU, directly home, if they tolerated a clear-fluid diet, had pain controlled with oral analgesia, and had the ability to ambulate and urinate independently. Patients who had more extensive surgery than anticipated and those with intraoperative/postoperative complications were admitted and no longer eligible for the SDD program. All patients were evaluated by the colorectal team (colorectal surgeon or resident physician) to ensure they satisfied the aforementioned discharge criteria.
OutcomesOur primary outcome measure was successful or failed SDD. Failed SDD occurred when patients were not discharged from PACU on the day of their surgery, or if they presented to the ED or had unplanned clinic visits within the first 3 PODs. Three days were selected because it is the targeted LOS according to ERPs used at our center and because previous research has demonstrated early GI dysfunction occurs between POD1 and POD2.8 Early postoperative complications were defined as those that were experienced in the PACU before SDD. We excluded patients who experienced intraoperative complications (unplanned stoma, conversion to open, greater extent of surgery, multivisceral resection, etc) from the SDD cohort because these “SDD failures” were not attributable to patient-dependent factors. Secondary outcomes included differences in baseline patient characteristics, complications, reoperations, readmission, and 30-day ED visits. The Clavien-Dindo Classification and the Comprehensive Complication Index (CCI) were used to classify postoperative complications.9,10
Statistical AnalysisData were analyzed using Stata version 17.1 (StataCorp, College Station, TX), and statistical significance was defined as a p value of <0.05. Categorical variables were reported as frequency and percentage, whereas continuous variables were expressed as mean and SD. When indicated, univariate analysis of categorical variables was performed using the χ2 test or Fisher exact probability test, and the Student t test or the Kruskal-Wallis test was used for continuous variables. A multiple logistic regression was performed to identify predictive factors of successful SDD after controlling for important confounders (age, comorbidities, sex, and procedure). No subgroup analyses were performed.
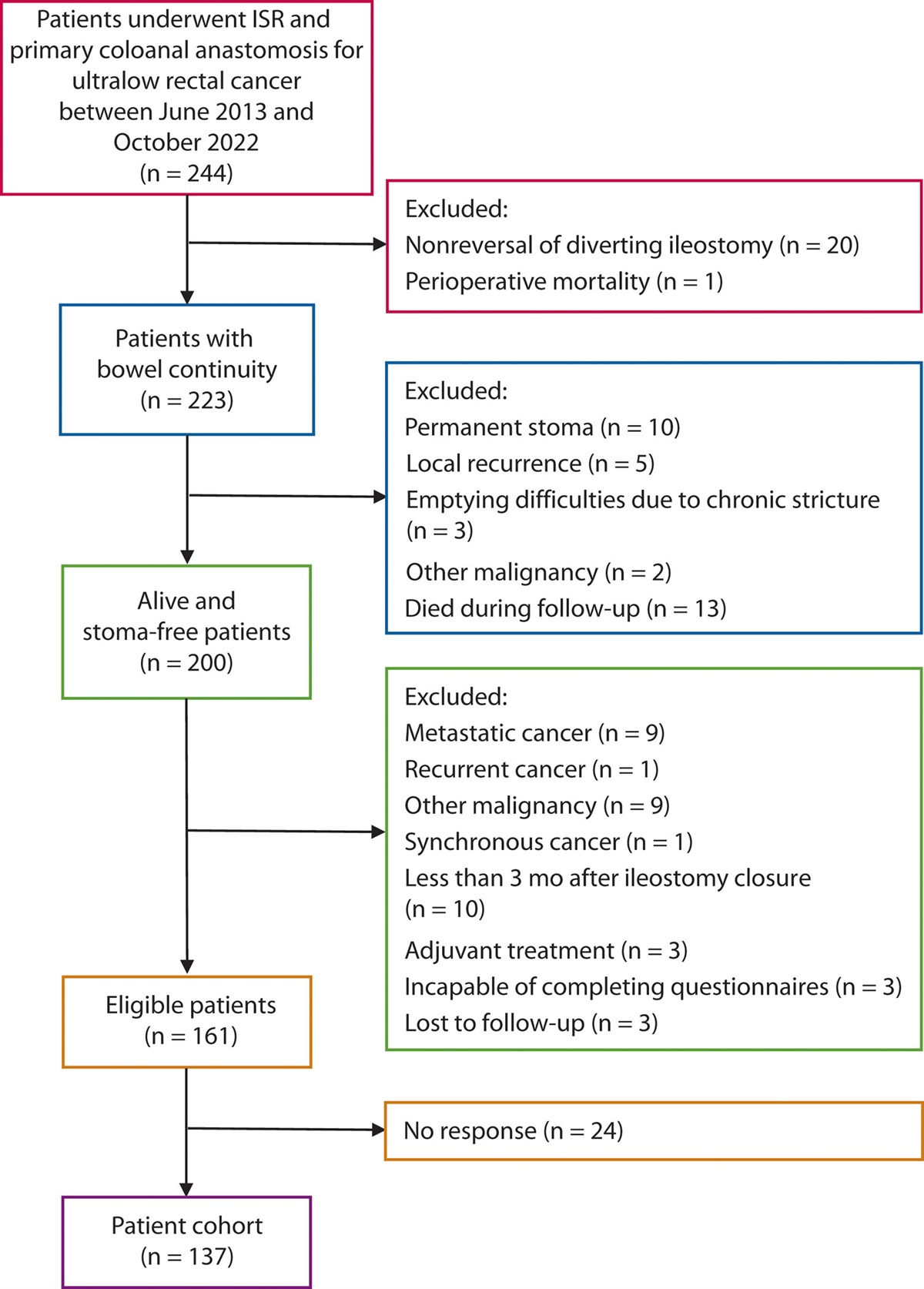
RESULTSA total of 670 elective colorectal resections were performed during the study period. Four hundred fifty-six patients were not eligible for SDD because they did not fit the aforementioned inclusion criteria, underwent a planned open procedure or new stoma, or refused to participate. A total of 214 patients were recruited for SDD, 9 of whom were excluded because of intraoperative complications, extensive surgical intervention, or unplanned stoma creation (Fig. 1). Among the 205 patients included in the final cohort, 13 (6.3%) experienced early postoperative complications and 17 (8.3%) failed SDD criteria for a total of 30 patients (14.6%) requiring an unplanned admission (Fig. 1). The most common reasons for SDD failure from PACU were inadequate pain control and patient/caregiver refusal (Fig. 1). A total of 175 patients (85.3%) were discharged on the same day as their surgery with 14 (8.0%) presenting to the ED within 3 PODs (Fig. 1). Therefore, a total of 161 patients (78.5%) were categorized as SDD success and 44 (21.5%) as SDD failure.
 FIGURE 1.:
FIGURE 1.: Flow diagram of patients enrolled in same-day discharge (SDD). ED = emergency department; PACU = postoperative anesthesia care unit.
A comparison of the patient and operative characteristics of the SDD successes and failures is shown in Table 1. SDD failure patients were more likely to have increased comorbidities than the SDD success cohort. There were no differences in baseline characteristics, procedures performed, or indications for surgical intervention between groups (Table 1). There was no difference in overall operative time between both groups; however, time spent in PACU was significantly longer for the SDD failure group. Mean morphine milliequivalents in the PACU were also similar between groups, with a small subset of patients requiring no opioids in the PACU (Table 1). Almost all patients received NSAIDs intraoperatively or in the PACU, with no difference between groups (Table 1). A proportion of patients (26%; 55/205) did not receive a transversus abdominis plane (TAP) block, including those undergoing colectomy (14/55) and stoma reversal (41/55).
TABLE 1. - Cohort characteristics Patient characteristics and outcomes Successful SDDCCI = Charlson Comorbidity Index; ED = emergency department; NSAID = nonsteroidal anti-inflammatory drug; PACU = postanesthesia care unit; SDD = same-day discharge; TAP = transversus abdominis plane.
aClinically significant findings (p < 0.05).
bLow anterior resection is defined by extraperitoneal colorectal anastomosis.
Thirty-day ED visits, complication rates, readmissions, and mean LOS were significantly higher in the SDD failure group (Table 1). The most common cause of SDD failure from the PACU was inadequate pain control or patient refusal (Table 2). Patients who failed SDD from the PACU spent on average 2 days in the hospital. Patients who were discharged on POD 0, however, failed SDD secondary to ED visits within 72 hours primarily for anastomotic bleeding, GI dysfunction, and urinary retention (Table 2). All patients presenting with GI dysfunction required readmission (n = 4), with 2 of those patients having undergone stoma reversal surgery. Among the patients they readmitted, 1 required surgical intervention because of wound dehiscence and 1 patient died secondary to cardiac complications.
TABLE 2. - Reasons for SDD failure Reasons for failure to discharge on POD 0 N = 30 Early postoperative complications Anastomotic bleed 3 Rectus sheath hematoma 1 Traumatic Foley insertion 1 Cardiac monitoring/workup 2 Hemodynamic instability 3 Oxygen requirements 1 Urinary retention 1 Delirium 1 Recommended prolonged PACU stay 4 Spinal anesthesia complication 1 Inadequate pain control 6 Patient/caregiver refusal 5 Significant postoperative nausea 1 Reasons for failure of SDD secondary to ED within 72 h N = 14 Anastomotic bleeding 4 Anastomotic leak 1 Small-bowel obstruction (anastomotic hematoma) 1 Urinary retention 3 GI dysfunction 4 Fever without cause 1ED = emergency department; PACU = postanesthesia care unit; POD = postoperative day; SDD = same-day discharge.
On multiple regression analysis, after controlling for important covariates (age, comorbidities, sex, and procedure), SDD failure was associated with a higher Charlson Comorbidity Index (OR 0.79; 95% CI, 0.66–0.95) and prolonged PACU stay (OR 0.99; 95% CI, 0.99–0.99). Individuals who received a TAP block (OR 4.1; 95% CI, 1.2–14) and those who did not consume opioids (OR 4.6; 95% CI, 1–21) in the PACU were more likely to have SDD success.
DISCUSSIONThere is increasing evidence to support the feasibility and safety of SDD for elective colorectal surgery. SDD has demonstrated similar postoperative complications, readmissions, and reoperation rates as standardized ERPs.3 The benefit of SDD is not solely patient-related—shorter hospital stays have the dual advantage of reduced cost and carbon footprint through decreased resource consumption.11,12 With this incentive, we sought to determine factors that may impact successful SDD as an area of potential intervention.
Our results show that comorbidity status, duration of time in the PACU, TAP block administration, and use of early opioids for pain control were predictive of success or failure of SDD. This is not surprising considering that significant comorbidities have been associated with prolonged LOS above the average 3-day target for ERPs after colorectal surgery.13,14 The success of SDD depends on many factors, with opioid-sparing postoperative pain control as a major pillar to its success. The literature has shown that routine TAP block and minimal postoperative opioid consumption in patients undergoing abdominal surgery result in adequate pain control and reduced postoperative ileus.15–17 Our study supports these findings as patients who received TAP blocks and those who did not require postoperative opioids in the PACU were more likely to have successful SDD. Although the majority of patients who did not receive a TAP block underwent stoma closures, a proportion of patients undergoing colectomy did not receive a TAP block. However, when controlling for both the procedure and TAP block in our multivariate analysis, only the TAP block was found to be significant in predicting successful SDD.
In addition to the importance of postoperative pain control, our results show that time spent in the PACU may also impact SDD success—patients with prolonged PACU time after surgery were more likely to fail SDD. It is unlikely that the prolonged PACU time was solely related to patients being enrolled in our SDD program, given that a previous study comparing SDD to ERP demonstrated similar PACU times.4 However, the negative impacts of prolonged PACU time are documented in the literature as being associated with clinical deterioration and longer LOS after surgery.18 Although prolonged PACU time may be related to a variety of factors, including reduced hospital capacity, in certain circumstances, it may also be considered a surrogate for time to achieve discharge criteria among SDD patients. Therefore, it is likely that patients with prolonged PACU stay either took longer to meet discharge criteria or eventually failed and required admission. There is likely a PACU stay cutoff at which patients are unlikely to meet discharge criteria and require admission. This would be an interesting future targeted area of research as it is likely influenced by each center’s unique institutional recovery process.19 These results suggest that minimal comorbidities, opioid-sparing analgesia, use of regional nerve blocks, and reduced PACU stay are associated with SDD success. Therefore, it is recommended that these factors be considered when selecting SDD candidates.
Although select patients required admission from PACU secondary to unavoidable early postoperative complications, a proportion of individuals fail SDD for potentially preventable causes. Among the 17 patients (8.2%) who failed SDD from the PACU, most were for inadequate pain control. This is unexpected as there were no differences in the amount of postoperative morphine equivalents or NSAIDs between failed and SDD success groups. Because pain is subjective, not all patients respond to acute postoperative pain uniformly, which may explain these findings. However, our results are limited as we did not use a multimodal approach to better classify postoperative pain.20 In keeping with the current literature, our findings indicate that the second leading cause for SDD failure from the PACU was patient or caregiver refusal.6,7
Our experience suggests that there is a myriad of factors that can potentially lead to SDD refusal, including fear of adverse outcomes, anxiety, suboptimal preoperative education, and/or preparation. This occurred despite our use of a smartphone application that included a patient–physician communication feature, which in previous studies was shown to enhance patients’ sense of security and relieve anxiety postdischarge.4 Future studies should investigate how patient/caregiver personality characteristics, baseline anxiety, health literacy, and engagement levels interact with willingness to undergo SDD.
The literature has demonstrated that patient-related outcomes are similar between SDD and ERPs; however, there are no reports comparing successful and failed SDD cohorts. Our data suggest that patients who failed SDD had a higher 30-day complication rate, ED visits, and readmissions. It is important to note that among patients who failed SDD because of postoperative complications, only 2 patients required reoperation with only 1 anastomotic leak (Table 2). Moreover, only 1 patient failed SDD secondary to an unplanned clinic visit for a blocked Foley catheter (Table 2). These findings may be related to the fact that our SDD failure group had more comorbidities than those undergoing successful SDD. This is in keeping with other studies that have shown an association between increased postdischarge unplanned visits and increased comorbidities.21 While malignancy may contribute to increased CCI score for a subset of our cohort, many patients underwent surgery for diverticulitis, IBD, or stoma reversal. Therefore, it is likely that select patients have an elevated CCI because of other underlying comorbidities. Currently, little is published in terms of why those with SDD failure have worse postoperative outcomes, and it remains an area of potential investigation. In particular, there may be a potential role for preoperative prehabilitation programs to “convert” patients into SDD candidates and broaden the inclusion criteria. In other studies, prehabilitation interventions have significantly increased functional capacity and decreased postoperative complications for patients undergoing colorectal surgery.22 However, no patients were included in the present study. These findings were originally presented at the annual meeting of the American Society of Colon and Rectal Surgeons.23
The findings of this study should be interpreted in the setting of other limitations. Patient activation (PA) was not measured in this study. The literature has demonstrated that low PA, a patient’s ability to manage their own health, is associated with increased postoperative complications and unplanned health care utilization after major abdominal surgery.24 Therefore, the higher complication rates and ED visits in our SDD failed cohort may be related to PA. Another potential limitation is that we did not actively collect information in terms of patient interaction with the Caresense application. However, our previous study describing the initial implementation of SDD at our center reported a 76% usage rate with an average of 21 direct messages from patients during their recovery process.4 In addition, our study included patients who were highly selected, which may affect generalizability. All patients required a smartphone device and familiarity with its utilization to download the follow-up application. Older patients may not have access to a smartphone or be as familiar with technology as younger patients. However, smartphone technology is increasing among the older population and colorectal cancer is also increasing among younger patients; therefore, it is likely that access and utilization of the application will level out to a certain degree.25,26 Finally, we did not use pain scores or recovery metrics, making it difficult to classify the degree of pain control in patients who failed SDD secondary to inadequate analgesia.
CONCLUSIONOur study suggests that significant comorbidities and prolonged PACU time were associated with SDD failure. In addition, TAP blocks and no postoperative opioids in the PACU were associated with SDD success. Our findings also suggest that discharge on POD 0 was associated with lower overall complications, ED visits, and readmissions in the first 30 days after surgery compared to individuals who were unable to be discharged on POD 0 despite a small proportion of patients discharged on POD 0 requiring an early unplanned hospital visit.
Ultimately, our findings demonstrate that those who fail SDD have worse postoperative outcomes than those with SDD success. These results provide preliminary evidence on factors associated with successful and failed SDD, which may provide areas for further research in hopes of improving current ERPs after colorectal surgery.
REFERENCES 1. Zhuang CL, Ye XZ, Zhang XD, Chen B-C, Yu Z. Enhanced recovery after surgery programs versus traditional care for colorectal surgery: a meta-analysis of randomized controlled trials. Dis Colon Rectum. 2013;56:667–678. 2. Lee L, McLemore E, Rashidi L. Same-day discharge after minimally invasive colectomy. JAMA Surg. 2022;157:1059–1060. 3. McLemore EC, Lee L, Hedrick TL, et al. Same day discharge following elective, minimally invasive, colorectal surgery: a review of enhanced recovery protocols and early outcomes by the SAGES Colorectal Surgical Committee with recommendations regarding patient selection, remote monitoring, and successful implementation. Surg Endosc. 2022;36:7898–7914. 4. Lee L, Eustache J, Baldini G, et al. Enhanced Recovery 20—same day discharge with mobile app follow-up after minimally invasive colorectal surgery. Ann Surg. 2021;276:e812–e818. 5. Vu MM, Curfman KR, Blair GE, Shah CA, Rashidi L. Beyond enhanced recovery after surgery (ERAS): evolving minimally invasive colectomy from multi-day admissions to same-day discharge. Am J Surg. 2023;225:826–831. 6. Gignoux B, Gosgnach M, Lanz T, et al. Short-term outcomes of ambulatory colectomy for 157 consecutive patients. Ann Surg. 2018;270:317–321. 7. Seux H, Gignoux B, Blanchet MC, et al. Ambulatory colectomy for cancer: results from a prospective bicentric study of 177 patients. J Surg Oncol. 2022;127:434–440. 8. Alsharqawi N, Alhashemi M, Kaneva P, et al. Validity of the I-FEED score for postoperative gastrointestinal function in patients undergoing colorectal surgery. Surg Endosc. 2019;34:2219–2226. 9. Clavien PA, Barkun J, de Oliveira ML, et al. The Clavien-Dindo classification of surgical complications: five-year experience. Ann Surg. 2009;250:187–196. 10. Clavien PA, Vetter D, Staiger RD, et al. The Comprehensive Complication Index (CCI®): added value and clinical perspectives 3 years “down the line”. Ann Surg. 2017;265:1045–1050. 11. Slim K, Selvy M, Albaladejo P. Enhanced recovery programs and carbon footprint. Anaesth Crit Care Pain Med. 2020;39:665–666. 12. Lee L, Mata J, Ghitulescu GA, et al. Cost-effectiveness of enhanced recovery versus conventional perioperative management for colorectal surgery. Ann Surg. 2014;262:1026–1033. 13. Keller DS, Bankwitz B, Woconish D, et al. Predicting who will fail early discharge after laparoscopic colorectal surgery with an established enhanced recovery pathway. Surg Endosc. 2013;28:74–79. 14. Feroci F, Lenzi E, Baraghini M, et al. Fast-track surgery in real life: how patient factors influence outcomes and compliance with an enhanced recovery clinical pathway after colorectal surgery. Surg Laparosc Endosc Percutan Tech. 2013;23:259–265. 15. Viderman D, Aubakirova M, Abdildin YG. Transversus abdominis plane block in colorectal surgery: a meta-analysis. Front Med (Lausanne). 2022;8:802039. 16. Kamdar NV, Hoftman N, Rahman S, Cannesson M. Opioid-free analgesia in the era of enhanced recovery after surgery and the surgical home: implications for postoperative outcomes and population health. Anesth Analg. 2017;125:1089–1091. 17. Simpson JC, Bao X, Agarwala A. Pain management in enhanced recovery after surgery (ERAS) protocols. Clin Colon Rectal Surg. 2019;32:121–128. 18. Mann-Farrar J, Egan E, Higgins A, et al. Are postoperative clinical outcomes influenced by length of stay in the postanesthesia care unit? J Perianesth Nurs. 2018;34:386–393. 19. Lee L, Eustache J, Tran-McCaslin M, et al. North American multicentre evaluation of a same-day discharge protocol for minimally invasive colorectal surgery using mHealth or telephone remote post-discharge monitoring. Surg Endosc. 2022;36:9335–9344. 20. Wideman TH, Edwards RR, Walton DM, Martel MO, Hudon A, Seminowicz DA. The multimodal assessment model of pain: a novel framework for further integrating the subjective pain experience within research and practice. Clin J Pain. 2018;35:212–221. 21. Flynn DE, Mao D, Yerkovich ST, et al. The impact of comorbidities on post-operative complications following colorectal cancer surgery. PLoS One. 2020;15:e0243995. 22. Molenaar CJL, Minnella EM, Coca-Martinez M, et al.; PREHAB Study Group. Effect of multimodal prehabilitation on reducing postoperative complications and enhancing functional capacity following colorectal cancer surgery: the PREHAB randomized clinical trial. JAMA Surg. 2023;158:572–581. 23. Paradis TRS, Robitaille S, Wang A, et al. Predictive factors for failure of same-day discharge following minimally invasive colectomy and stoma reversal [ASCRS abstract S19]. Dis Colon Rectum. 2023;66:13. 24. Dumitra T, Ganescu O, Hu R, et al. Association between patient activation and health care utilization after thoracic and abdominal surgery. JAMA Surg. 2021;156:e205002. 25. Howren A, Sayre EC, Loree JM, et al. Trends in the incidence of young-onset colorectal cancer with a focus on years approaching screening age: a population-based longitudinal study. J Natl Cancer Inst. 2021;113:863–868. 26. Busch PA, Hausvik GI, Ropstad OK, Pettersen D. Smartphone usage among older adults. Comput Hum Behav. 2021;121:106783.
留言 (0)