
記住我



Colon cancer is a common cancer worldwide, and approximately 30% to 50% of patients treated with curative resection are later diagnosed with disease recurrence.1–3
The lungs are one of the most common sites of colon cancer metastasis.4–6 Treatment of pulmonary metastasis depends on the location, number, and size of tumors. In addition, the patient’s health status and accompanying metastases are important factors affecting treatment outcomes. Metastasectomy of lung lesions is the only radical treatment for pulmonary metastasis that allows long-term survival.
Only a few studies have investigated pulmonary metastasis in colon cancer, and they reported that 2% to 10% of patients developed pulmonary metastasis. However, patient characteristics were heterogeneous, and data on pulmonary metastasis incidence by the TNM stage were scarce.
Therefore, the objective of this study was to evaluate pulmonary metastasis incidence in colon cancer treated with radical surgery without metastasis and identify risk factors for pulmonary metastasis according to the TNM stage.
MATERIALS AND METHODSThis retrospective study included all patients with colon cancer without metastasis who underwent radical surgery for primary tumor at the Samsung Medical Center between January 2007 and December 2016. The following patients were excluded from the study: those diagnosed with metastasis before their operation, those with familial cancer or an indeterminate lesion in the lungs on a chest CT scan before the operation, patients being treated for recurrent disease, those who underwent palliative surgery or preoperative chemotherapy, and patients lacking follow-up data. The preoperative diagnosis was performed with colonoscopy, abdominopelvic CT scan, and chest CT scan. This study was approved by the Institutional Review Board of Samsung Medical Center.
All patients underwent radical resection of their primary tumor with regional lymphadenectomy. The TNM stage was determined by the eighth edition of the American Joint Cancer Committee.7 Patients underwent adjuvant chemotherapy according to National Comprehensive Cancer Network guidelines.8 Histopathologic features were evaluated by 2 GI pathologists who had no clinical information about the patients. Patients underwent abdominopelvic CT and chest CT every 3 or 6 months after the operation. Colonoscopy was performed 1 year after the primary operation and then every other year after that.
Statistical analyses were performed using Rex (version 3.0.3; RexSoft Inc., Seoul, Korea) and SPSS version 27 (SPSS Inc., Chicago, IL). The χ2 and Fisher exact probability tests were used to analyze categorical variables. The Student t test and the Wilcoxon rank-sum test were used to analyze continuous variables. One-way ANOVA was used to analyze quantitative differences between the groups. The Kaplan-Meier method was used to analyze survival curves, and differences between the curves were evaluated using the log-rank test. The Cox proportional hazards regression model was used to analyze the variables that could independently influence survival and risk grouping. Variables with a p value of <0.05 in the univariable analysis were included in the multivariable analysis using a Cox proportional model. A p value of ≤0.05 in the multivariable analysis was considered statistically significant.
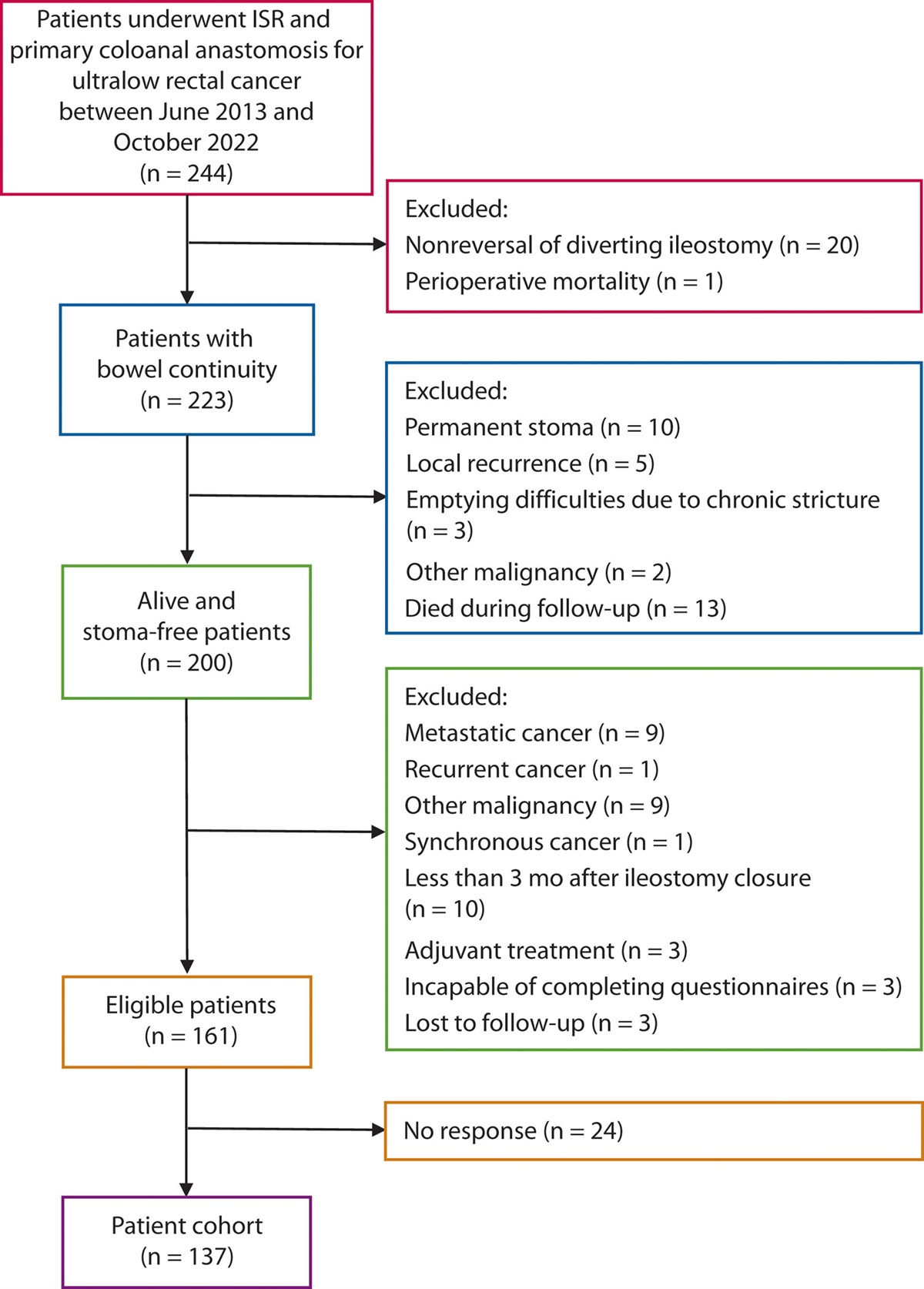
RESULTSThe flowchart of patient selection is presented in Figure 1. A median follow-up of 70 (range, 7–172) months and a total of 4889 patients with colon cancer treated with radical surgery were analyzed. This analysis included 2809 men and 2080 women with a median age of 60 (SD, 11.2 ) years. The distribution of tumor locations was as follows: cecum (n = 240), ascending colon (n = 1200), transverse colon (n = 346), descending colon (n = 323), and sigmoid colon (n = 2780). The distribution of the TNM stage was as follows: stage I (n = 1168), stage II (n = 1653), and stage III (n = 2068).
 FIGURE 1.:
FIGURE 1.: Flow chart of patient selection.
Of the 4889 patients with colon cancer, 156 (3.2%) were diagnosed with pulmonary metastasis with a median interval of 16 months from radical surgery for colon cancer to detection of pulmonary metastasis. Baseline clinicopathologic features of patients with and without pulmonary metastasis are described in Table 1. Patients with pulmonary metastasis had higher preoperative CEA level, TNM stage, and N stage, as well as higher rates of cancer obstruction, ulceration, lymphatic invasion, vascular invasion, perineural invasion, tumor budding, and adjuvant chemotherapy (Table 1). The incidence rate of pulmonary metastasis by the TNM stage was 0.5% in stage I, 1.6% in stage II, and 6% in stage III (Fig. 2).
TABLE 1. - Baseline clinicopathologic features of patients with lung metastasis after radical resection of colon cancer Variable Without pulmonary metastasis (n = 4733) With pulmonary metastasis (n = 156) p Age, y, median (range) 62 (21–93) 63 (26–87) 0.148 Sex 0.916 Male 2720 (57.5%) 89 (57.1%) Female 2013 (42.5%) 67 (42.9%) BMI, median (range) 23.2 (14.7–44) 23.1 (15–31) 0.158 CEA, ng/mL <0.001 <5 4021 (85%) 107 (68.6%) ≥5 712 (15%) 49 (31.4%) Cancer obstruction <0.001 No 3968 (83.8%) 103 (66.0%) Yes 765 (16.2%) 53 (34.0%) Cancer perforation 0.082 No 4665 (98.6%) 151 (96.8%) Yes 68 (1.4%) 5 (3.2%) Gross type <0.001 No ulceration 1488 (31.4%) 25 (16.0%) Ulceration 3245 (68.6%) 131 (84.0%) Tumor size, cm, median (range) 4 (0.1–15) 4.5 (0.5–12) 0.072 Differentiation 0.282 Well to moderate 4347 (91.8%) 147 (94.2%) Poor, MAC, SRC 386 (8.2%) 9 (5.8%) TNM stage <0.001 I 1162 (24.5%) 6 (3.8%) II 1627 (34.4%) 26 (16.7%) III 1944 (41.1%) 124 (79.5%) T stage <0.001 T1 744 (15.7%) 7 (4.5%) T2 671 (14.2%) 7 (4.5%) T3 2709 (57.2%) 87 (55.8%) T4 609 (12.9%) 55 (35.2%) N stage <0.001 N0 2788 (58.9%) 32 (20.5%) N1 1382 (29.2%) 76 (48.7%) N2 563 (11.9%) 48 (30.8%) No. of harvested LN 0.759 <12 363 (7.7%) 13 (8.3%) ≥12 4370 (92.3%) 143 (91.7%) Lymphatic invasion <0.001 No 3273 (69.2%) 70 (44.9%) Yes 1460 (30.8%) 86 (55.1%) Vascular invasion <0.001 No 4159 (87.9%) 109 (69.9%) Yes 574 (12.1%) 47 (30.1%) Perineural invasion <0.001 No 3784 (80%) 83 (53.2%) Yes 949 (20%) 73 (46.8%) Tumor budding <0.001 No 2843 (60.1%) 51 (32.7%) Yes 1890 (39.9%) 105 (67.3%) Adjuvant CTx 0.029 No 2271 (48%) 61 (39.1%) Yes 2462 (52%) 95 (60.9%)CTx = chemotherapy; LN = lymph node; MAC = mucinous adenocarcinoma; SRC = signet-ring cell.
 FIGURE 2.:
FIGURE 2.: Incidence of pulmonary metastasis according to the TNM stage.
In 156 patients diagnosed with pulmonary metastasis, 40 showed combined metastasis to other sites. Twenty patients had hepatic metastasis, which was the most common metastatic site, and other metastasis sites were para-aortic lymph node, peritoneal seeding, ovary, spleen, anastomosis site, pelvic mass, and bone.
The risk factors for pulmonary metastasis were preoperative CEA >5 ng/mL (p = 0.025), cancer obstruction (p = 0.014), advanced N stage (p < 0.001), venous invasion (p = 0.016), perineural invasion (p = 0.005), and adjuvant chemotherapy received for primary colon cancer in multivariable analysis (p < 0.001; Table 2). In subgroup analyses, only perineural invasion was a risk factor for pulmonary metastasis in stage I (p = 0.022). In stage II, preoperative CEA >5 ng/mL (p < 0.001), cancer perforation (p = 0.003), and tumor budding (p = 0.020) were independent risk factors for pulmonary metastasis in multivariable analysis. In stage III, cancer obstruction (p = 0.017), advanced pT stage (p = 0.012), number of harvested lymph nodes <12 (p = 0.001), venous invasion (p = 0.007), perineural invasion (p = 0.014), and adjuvant chemotherapy not received (p < 0.001) were independent risk factors for pulmonary metastasis (Table 3).
TABLE 2. - Univariable and multivariable analyses of prognostic factors for pulmonary metastasis after radical resection of colon cancer Variables Univariable analysis Multivariable analysis p p HR 95% CI Age 0.111 Sex 0.900 BMI 0.128 CEA, ng/mL <0.001 0.025 1.510 1.054–2.163 Cancer obstruction <0.001 0.014 1.576 1.095–2.270 Cancer perforation 0.041 0.234 1.752 0.696–4.410 Gross type <0.001 0.532 1.164 0.723–1.874 Tumor size 0.033 0.092 0.927 0.848–1.013 Differentiation 0.358 T stage <0.001 0.587 N stage <0.001 <0.001 3.261 1.869–5.692 No. of harvested LN 0.796 Lymphatic invasion <0.001 0.334 1.191 0.835–1.698 Vascular invasion <0.001 0.016 1.591 1.089–2.325 Perineural invasion <0.001 0.005 1.635 1.157–2.310 Tumor budding <0.001 0.156 1.313 0.901–1.913 Adjuvant CTx <0.001 <0.001 2.412 1.716–3.430CTx = chemotherapy; LN = lymph node.
CTx = chemotherapy; LN = lymph node.
Patients diagnosed with pulmonary metastasis were treated with either operation or chemotherapy depending on their physical status, character of pulmonary metastasis (location, number, and size), and accompanying metastasis of other organs. Ninety-five patients (60.9%) underwent radical surgery, 36 patients (23.1%) underwent palliative chemotherapy, and 25 patients (16%) did not undergo any treatment because of poor performance or patient refusal to undergo chemotherapy. The overall survival of patients with pulmonary metastasis was significantly higher in the radical surgery group than in the chemotherapy group (85.3% vs 11.1%, p < 0.001; Fig. 3). The median months from the day of suspicion for pulmonary metastasis to operation day was 3 months (range, 0–29). Of the 95 patients who underwent operation for pulmonary metastasis, 82 (86.3%) underwent wedge resection and 13 (13.7%) underwent lobectomy. Of the 95 patients, 70 (73.7%) underwent chemotherapy before or after surgery, and among these, 67 patients (95.7%) received chemotherapy preoperatively and 3 (4.3%) received chemotherapy postoperatively. Chemotherapy regimens were as follows: XELOX (capecitabine + oxaliplatin), XELIRI (capecitabine + irinotecan), FOLFOX (folinic acid/5-FU/oxaliplatin), 5-fluorouracil (5-FU) + leucovorin, and FOLFOX/FOLFIRI (folinic acid/5-FU/irinotecan) + bevacizumab/cetuximab. Among the 25 patients who did not undergo chemotherapy, 8 refused chemotherapy, 7 could not endure chemotherapy because of their poor general condition, 2 could not manage the side effects of chemotherapy, and 8 had an unknown reason. Of the 95 patients with pulmonary metastasis treated with an operation, 29 (30.5%) were diagnosed with rerecurrence of pulmonary metastasis. Thirty-six with pulmonary metastasis were treated with chemotherapy. The palliative chemotherapy regimens included XELOX, FOLFOX, FOLFIRI, XELIRI, and XELOX/FOLFOX/FOLFIRI + bevacizumab/cetuximab.
 FIGURE 3.:
FIGURE 3.: Overall survival curve according to treatment type for pulmonary metastasis.
DISCUSSIONIn this study, pulmonary metastasis in colon cancer without synchronous metastasis was evaluated. By the TNM stage, the pulmonary metastasis incidence rate was 0.5% in stage I, 1.6% in stage II, and 6% in stage III. Among patients with pulmonary metastasis, 60.9% underwent radical resection of metastatic lesions, and their cancer-specific survival was significantly higher than those in the chemotherapy group.
The lungs are one of the most common sites for colon cancer metastasis. Oligometastasis in the lungs from colon cancer can be treated with resection with the R0 state, which increases overall survival within the range of 45% to 65%.9 Previous studies showed 4.7% to 5.1% rates of pulmonary metastasis, which was higher than this study. This might be due to differences in patient selection, which included stage IV and rectal cancer. Also, we excluded patients with indeterminate lesions in the lungs on chest CT. In previous studies, patients with indeterminate lesions in the lungs on a chest CT scan accounted for 10.2% to 30.9% of pulmonary metastasis.10–12 Excluding patients with indeterminate lesions thus might have reduced the metastasis rate compared with previous studies. Pulmonary metastasis incidence was significantly higher in stage III, compared with stages I and II, which was similar to previous results.13,14 Lymph node metastasis was a significant risk factor for pulmonary metastasis, which might have affected the higher incidence of pulmonary metastasis in stage III colon cancer compared with stage I and II.15
In this study, preoperative CEA was a risk factor for pulmonary metastasis. Previous studies also indicated that preoperative CEA was a significant risk factor for pulmonary metastasis.16,17 In histopathologic results, vascular invasion and perineural invasion were risk factors for pulmonary metastasis. Venous invasion is defined as extramural and intramural vascular invasion, and it is related to lymph node metastasis and is a predictive factor of colorectal cancer recurrence.18,19 Perineural invasion of tumor cells that present in the nerve sheath or as tumor foci that take up 33% or more of the outer circumference of the nerve is also a predictive factor for colorectal cancer recurrence.18,20,21 Similar to previous studies, pathologic T and N stages were independent risk factors for pulmonary metastasis in this study.16,22 Moreover, adjuvant chemotherapy was a risk factor for pulmonary metastasis in the entire cohort, likely because patients who underwent chemotherapy were in an advanced stage of colon cancer. In the subgroup analysis, the absence of adjuvant chemotherapy was identified as a risk factor for pulmonary metastasis in stage III colon cancer, which is not surprising given that chemotherapy contributes to improved disease-free survival.23–25
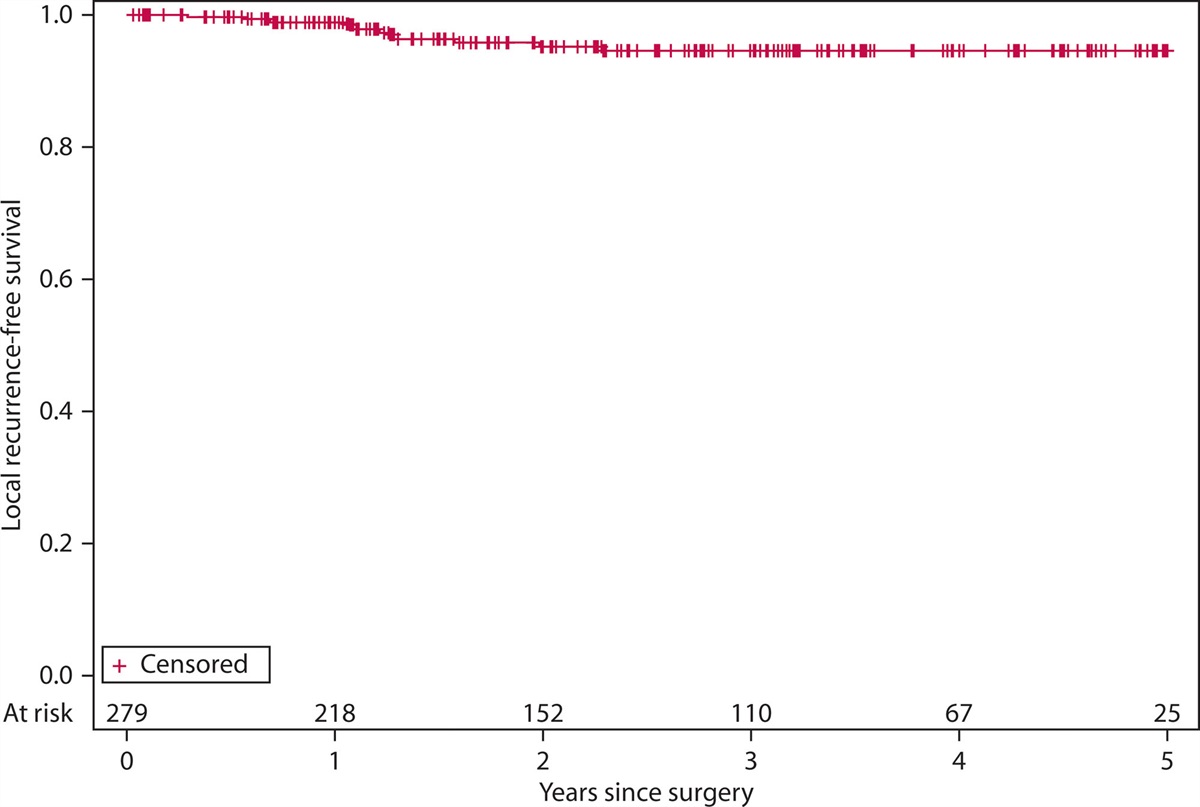
Pulmonary metastasis was treated either by operation or chemotherapy, except for patients who either refused to undergo chemotherapy or who were unable to undergo chemotherapy. The percentage of patients who underwent an operation for pulmonary metastasis was 60.9%, which was much higher than previous studies reported.13,26 Also, 5-year cancer-free survival after lung metastasectomy for colon cancer was higher in this study than in previous studies.13,27 This might be due to the expanded indication for operation with advanced diagnostic tools for detecting pulmonary metastasis.28,29
This study has several limitations. First, it was conducted at a single center and is a retrospective study. Second, we excluded patients diagnosed with recurrence at another site before pulmonary metastasis to maintain consistent cohort characteristics. Thus, we were not able to evaluate the oncologic outcomes and risk factors for pulmonary metastasis that occurred after another recurrence. Third, the study duration was long, which might account for the heterogeneity in treatments for pulmonary metastasis. Fourth, this study was conducted at a high-volume quaternary center. Furthermore, it is important to note that some patients underwent regular surveillance at peripheral hospital systems, which could potentially lead to the loss of patients who developed pulmonary metastasis.
CONCLUSIONPreoperative CEA >5 ng/mL, cancer obstruction, advanced pT stage, advanced N stage, vascular invasion, perineural invasion, and adjuvant chemotherapy not received for primary colon cancer were risk factors for pulmonary metastasis in colon cancer. Also, patients who underwent radical surgery for lung metastasis had better survival compared with patients who underwent chemotherapy. Therefore, patients with risk factors for pulmonary metastasis should be recommended for intensive follow-up to detect lung metastasis, and they should be treated with radical surgery to give them the most favorable oncologic outcomes.
REFERENCES 1. Ferlay J, Colombet M, Soerjomataram I, et al. Cancer statistics for the year 2020: an overview. Int J Cancer. 2021;149:778–789. 2. Manfredi S, Bouvier AM, Lepage C, Hatem C, Dancourt V, Faivre J. Incidence and patterns of recurrence after resection for cure of colonic cancer in a well defined population. Br J Surg. 2006;93:1115–1122. 3. O’Connell MJ, Campbell ME, Goldberg RM, et al. Survival following recurrence in stage II and III colon cancer: findings from the ACCENT data set. J Clin Oncol. 2008;26:2336–2341. 4. Qiu M, Hu J, Yang D, Cosgrove DP, Xu R. Pattern of distant metastases in colorectal cancer: a SEER based study. Oncotarget. 2015;6:38658–38666. 5. Disibio G, French SW. Metastatic patterns of cancers: results from a large autopsy study. Arch Pathol Lab Med. 2008;132:931–939. 6. Hugen N, van de Velde CJH, de Wilt JHW, Nagtegaal ID. Metastatic pattern in colorectal cancer is strongly influenced by histological subtype. Ann Oncol. 2014;25:651–657. 7. Amin MB, Edge S, Greene FL, et al, eds. AJCC cancer staging manual. 7th ed. New York: Springer, 2017. 8. Benson AB, Venook AP, Al-Hawary MM, et al. Rectal cancer, version 22022, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2022;20:1139–1167. 9. Okumura T, Boku N, Hishida T, et al. Surgical outcome and prognostic stratification for pulmonary metastasis from colorectal cancer. Ann Thorac Surg. 2017;104:979–987. 10. Quyn AJ, Matthews A, Daniel T, Amin AI, Yalamarthi S. The clinical significance of radiologically detected indeterminate pulmonary nodules in colorectal cancer. Colorectal Dis. 2012;14:828–831. 11. Kim CH, Huh JW, Kim HR, Kim YJ. Indeterminate pulmonary nodules in colorectal cancer: follow-up guidelines based on a risk predictive model. Ann Surg. 2015;261:1145–1152. 12. Brent A, Talbot R, Coyne J, Nash G. Should indeterminate lung lesions reported on staging CT scans influence the management of patients with colorectal cancer? Colorectal Dis. 2007;9:816–818. 13. Watanabe K, Saito N, Sugito M, Ito M, Kobayashi A, Nishizawa Y. Incidence and predictive factors for pulmonary metastases after curative resection of colon cancer. Ann Surg Oncol. 2013;20:1374–1380. 14. Mitry E, Guiu B, Cosconea S, Jooste V, Faivre J, Bouvier AM. Epidemiology, management and prognosis of colorectal cancer with lung metastases: a 30-year population-based study. Gut. 2010;59:1383–1388. 15. Watanabe K, Nagai K, Kobayashi A, Sugito M, Saito N. Factors influencing survival after complete resection of pulmonary metastases from colorectal cancer. Br J Surg. 2009;96:1058–1065. 16. Huang Y, Zhao M, Yin J, et al. Pulmonary metastasis in newly diagnosed colon-rectal cancer: a population-based nomogram study. Int J Colorectal Dis. 2019;34:867–878. 17. Ge Y, Lei S, Cai B, et al. Incidence and prognosis of pulmonary metastasis in colorectal cancer: a population-based study. Int J Colorectal Dis. 2020;35:223–232. 18. Kim S, Huh JW, Lee WY, et al. Lymphovascular invasion, perineural invasion, and tumor budding are prognostic factors for stage I colon cancer recurrence. Int J Colorectal Dis. 2020;35:881–885. 19. Leijssen LGJ, Dinaux AM, Amri R, et al. Impact of intramural and extramural vascular invasion on stage II-III colon cancer outcomes. J Surg Oncol. 2019;119:749–757. 20. Liebig C, Ayala G, Wilks J, et al. Perineural invasion is an independent predictor of outcome in colorectal cancer. J Clin Oncol. 2009;27:5131–5137. 21. Huh JW, Lee JH, Kim HR, Kim YJ. Prognostic significance of lymphovascular or perineural invasion in patients with locally advanced colorectal cancer. Am J Surg. 2013;206:758–763. 22. Kim HY, Lee SJ, Lee G, et al. Should preoperative chest CT be recommended to all colon cancer patients? Ann Surg. 2014;259:323–328. 23. André T, Boni C, Mounedji-Boudiaf L, et al.; Multicenter International Study of Oxaliplatin/5-Fluorouracil/Leucovorin in the Adjuvant Treatment of Colon Cancer (MOSAIC) Investigators. Oxaliplatin, fluorouracil, and leucovorin as adjuvant treatment for colon cancer. N Engl J Med. 2004;350:2343–2351. 24. André T, Boni C, Navarro M, et al. Improved overall survival with oxaliplatin, fluorouracil, and leucovorin as adjuvant treatment in stage II or III colon cancer in the MOSAIC trial. J Clin Oncol. 2009;27:3109–3116. 25. Kuebler JP, Wieand HS, O’Connell MJ, et al. Oxaliplatin combined with weekly bolus fluorou
留言 (0)