Comprehensive DCM rehabilitation outcomes
The present study showed, for the first time, that comprehensive rehabilitation, as practiced in SCL units, administered by a multidisciplinary team, and implementing combined medical and para-medical specific skills to prevent medical complications of SCL, and improve patient functioning, achieved considerable functional gain for persons with DCM of all functional levels, beyond the gain that spinal surgery alone achieved. To assess the net effect of rehabilitation, it would have been reasonable to examine DCM individuals who received only rehabilitation or compare our patients with DCM patients who underwent spinal surgery without rehabilitation. This was not feasible in a retrospective study because (a) the prevailing approach advocates early referral of persons with DCM to surgical decompression, which limited the referral of persons with DCM to rehabilitation before spinal surgery, and (b) the assessments used in this study were not available for patients who were not admitted to rehabilitation. Nevertheless, we inferred about the contribution of rehabilitation alone to improved functioning. Our analyses distinguished the effect of rehabilitation from that of spinal surgery, isolating the effect of late post-surgical motor neurological change on daily performance during rehabilitation and examining the relationship of the functional gain during rehabilitation with the time from spinal surgery to rehabilitation.
In the study group, motor neurological scores increased during rehabilitation by 13%, daily functioning scores by 44%, and scores for ability realization by 37%. The analysis indicated that less than 30% of the improvement in the performance of daily activities during rehabilitation can be attributed to motor neurological recovery that may be related to the late effect of surgery, and about 70% to the increase in ability realization.
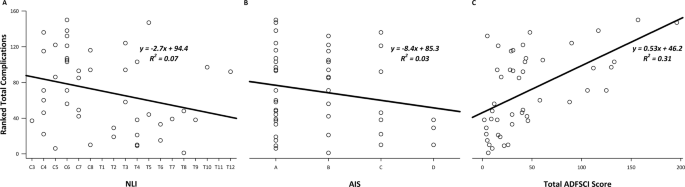
It may be argued that a substantial part of the improvement in performance during rehabilitation, which was not related to neurological changes that occurred during the same period, was a late response to changes caused by the surgery, before the start of rehabilitation. A possible interpretation of this claim is that rehabilitation hastens the rate of gain in performance, but the functional outcome of patients who do not undergo rehabilitation is improving irrespective of the neurological change during rehabilitation, and may ultimately be the same as of those undergoing rehabilitation without concomitant neurological improvement, even if it at a slower rate and over a longer period. We expect, however, that the influence of substantial changes related to surgery, which occurred before the rehabilitation, and are not related to the neurological improvement during rehabilitation, would substantially decrease with the time after the operation, before and during the rehabilitation. Thus, we expect that dSCIM-IIIr would also substantially decrease with the time after the operation. But the correlation between dSCIM-IIIr and the time from spinal surgery to rehabilitation was rather weak, as demonstrated in Fig. 1, which suggests that the contribution of surgical effects to the functional gain during rehabilitation, not related to the neurological recovery during rehabilitation, was minor. This supports the attribution of dSCIM-IIIr mainly, even if not only, to the comprehensive rehabilitation. We can safely extrapolate, therefore, that in patients with DCM, a considerable improvement in performance can be attained by rehabilitation alone, irrespective of the contribution of surgery to performance. Consequently, comprehensive rehabilitation can be offered as adequate conservative care for improving functioning in persons with DCM of all functional degrees.
Considering comprehensive rehabilitation before surgery for DCM
Although comprehensive rehabilitation achieved considerable functional gain for persons with DCM, beyond that of spinal surgery alone, based on the customary approach described in the Introduction, it should be offered only after spinal surgical intervention, at least for individuals with moderate or severe myelopathy [1, 3]. This approach is based on the notion that surgical intervention is more effective and safer than conservative care for these persons. But based on our findings, combined with published data of other studies, comprehensive rehabilitation can be at least as effective, and even safer, as shown below, and therefore should be tried in many cases, before the decision on surgery.
Careful assessment of the DCM literature reveals that the customary approach is not the unequivocal conclusion offered by the published data, because (a) a significant portion of the persons with DCM is at relatively low risk for deterioration with conservative care, contrary to the prevailing notion; (b) in patients with mild, moderate, or severe DCM, the estimated risk of deterioration and complications in the DCM literature is not necessarily lower after surgery than with conservative care; and (c) the deterioration rate under conservative care and the role of neurological change in inducing deterioration may be overestimated in the literature. We address these three points below.
(a)
The prevailing notion that the risk of deterioration in persons with DCM under conservative care is very high was adopted, based on an estimated deterioration rate of 20–62% [1]. Based on the published data, however, it is more plausible to conclude that the risk of deterioration in persons with DCM under conservative care is not high because this estimated deterioration rate indicates that 38–80% of the persons with DCM do not suffer from functional deterioration within 3–6 years of follow-up, and in those with mild DCM, more than 50% can remain unchanged or improve [1, 16].
(b)
If appropriate comparisons are used, the relative risk of deterioration and complications may be lower with conservative care than after surgery. The notion that surgery is safer for individuals with DCM is based on comparisons of the risk of deterioration after surgery with the total risk of deterioration with conservative care [1, 3]. But deterioration is attributed to surgery only if it occurs soon thereafter. Its risk should be compared with the risk of rapid deterioration that occurs soon after conservative care, combined with neurological follow-up. A reasonable estimation of the risk of rapid deterioration (with a course of less than 1–3 months) is between 1.4–13%, and near 7% on average (Table 4) [16,17,18,19]. A reasonable estimation of the average risk of all types of neurological deterioration, peri-operatively or early after DCM surgery is near 9% on average (Table 4) [5, 20,21,22,23,24]. Furthermore, Nakashima and colleagues described late neurological deterioration in 14% of people after laminoplasty, overall, 8.9–30.6% of patients suffered from at least one complication of surgery, and mortality was noted following up to 2.1% of spinal operations for DCM [5, 20,21,22,23,24,25,26,27].
Table 4 Published risks of DCM care.
(c)
The deterioration rate under conservative care and the role of neurological change in inducing it may be overestimated because most DCM studies based the assessment of clinical deterioration mainly on reports of performance. Despite claims of having assessed neurological change, these studies offer limited neurological information (Table 1) [3, 16, 19,20,21,22,23,24,25, 28, 29]. Assessments of performance, including those based on the JOA and mJOA scores, and subjective reports may be affected by several factors modifiable by medication and rehabilitation, and are not necessarily related to the DCM or the surgical intervention [1, 22]. Among these factors are pain, spasticity, motor skills in the presence of abnormal neurological status, fitness, mood, motivation, and primary or secondary gain. The effects of such factors may bias the assessment of change in performance [9]. Quantitative measures of the neurological status revealed a gap between neurological and functional change: Morishita and colleagues described chronic DCM patients with AMS of 91.8 ± 6.4, which represents a relatively mild neurological impairment, but with JOA scores of 10.1 ± 1.8, which represents severe disability. They demonstrated a degree of disability that exceeds that expected based on the DCM-related neurological deficit [18].
These insights suggest that repeated assessments can identify most of the individuals who deteriorate with conservative care before a significant functional change occurs, provided the assessments are sufficiently responsive to neurological changes. Based on the cited literature data (Table 4, if) these individuals are identified during the follow-up and undergo a decompressive operation only when deterioration starts, the overall neurological deterioration and risk of surgical complications for the entire DCM population will most likely be lower than the overall risk with the current customary indications for DCM surgery. Persons with DCM of all grades, who do not show deterioration in repeated neurological assessments, may therefore safely choose conservative care with neurological follow-up, avoiding operative complications for at least several years. For many persons with DCM of all grades, such conservative care can plausibly start with comprehensive rehabilitation, and surgical intervention may be considered if deterioration starts or comprehensive rehabilitation fails to improve performance.
Considering modifications in the guidelines for DCM follow-up and care
Based on our findings, which support the advantage of comprehensive rehabilitation, and on literature data challenging the extent of spine surgery benefits for persons with DCM, we suggest considering the introduction of the following changes into guidelines for DCM follow-up and care:
1.
Introduction of quantitative neurological assessment. For the detection of improvement or deterioration in persons with DCM, a physician or an experienced caregiver should use AMS, ASS and proprioception assessment [14].
2.
Introduction of quantitative assessment of performance. For the assessment and follow-up of the performance of daily activities, an experienced caregiver should use SCIM III [11]. SCI-ARMI can be used to assess the potential to improve performance in rehabilitation [9].
3.
Changing recommendations for interventions. Customary guidelines recommending surgical intervention for severe and moderate DCM, and offering a choice of surgical intervention or a supervised trial of structured rehabilitation for mild DCM, should be changed [1, 2] as follows: (1) Individuals with DCM and none or minimal and stable neurological and functional deficit should be followed up. Those with disruptive minimal deficits should be referred to ambulatory physical or occupational therapy. (2) Individuals with DCM with more than minimal and stable neurological or functional deficit should be assessed in a spinal rehabilitation facility for quantitative neurological status, actual performance, and the potential to improve performance in rehabilitation. Based on this assessment, patients should be referred to ambulatory rehabilitation, inpatient comprehensive rehabilitation, or consultation with a spine surgeon. (3) Surgical intervention should be considered if deterioration is evident in quantitative neurological assessments. Surgery may be also considered if actual performance is significantly impaired and close to potential performance, which means that the disability is significant and the potential to improve it in rehabilitation is poor.
4.
Introduction of follow-up instructions. Regular follow-up should follow ambulatory or inpatient rehabilitation. When DCM is diagnosed or clinical worsening is reported, initial follow-up should be conducted weekly, to enable identification of deteriorations that may occur within less than two weeks. If no deterioration is detected after two weeks, the follow-up should be monthly, to enable identification of deterioration that may occur within 1 month. After 3 months, it should be repeated every 3 months, to enable identification of deterioration that may occur within 3 months, and after a year without deterioration, every year, to enable identification of late deterioration.
5.
Introduction of instructions for post-operative assessment and care. After surgical intervention for DCM, patients should be referred to assessment in a SCL rehabilitation unit. Based on the findings of this assessment, patients should be referred to follow-up, ambulatory rehabilitation, or comprehensive inpatient rehabilitation.
Limitation of the study
A limitation of the present study is the lack of patients who received only surgical or only non-surgical treatment in the study sample. Our analyses circumvented this consequence of the prevailing approach to treating DCM.
Future research
To support our findings and their generalizability to all individuals with DCM, we recommend performing a study comparing patient groups after comprehensive rehabilitation alone and after surgery alone. To enable such a comparison, however, the guidelines for DCM care should be modified, as suggested in this article, at least for participants of the comparative study.



留言 (0)