Study population
We used data from the AICOPP, including 1520 incident dialysis patients. Details of the AICOPP have been previously described [14]. The cohort included patients who initiated dialysis between October 2011 and September 2013 at 17 facilities in Aichi, Japan. We screened patients aged ≥20 years and enrolled those who were discharged alive after hospitalization for dialysis initiation. Written informed consent was obtained from all patients. In our study of patients registered with AICOPP, we excluded patients referred to nephrologists <90 days prior to dialysis initiation or whose duration of nephrologist care was unknown, and patients who opted for peritoneal dialysis.
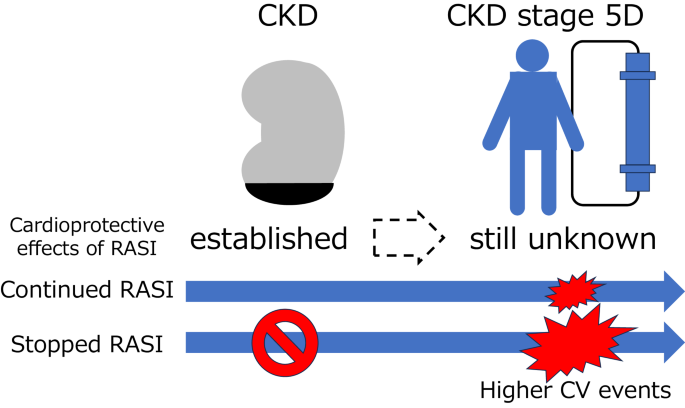
We recruited patients who had used angiotensin converting enzyme inhibitors (ACEIs) or angiotensin II receptor blockers (ARBs) 3 months prior to hemodialysis (HD) initiation and those who had data of ACEIs or ARBs at the time of HD initiation for survival analysis.
Baseline variables
Baseline demographic and clinical data, including blood and urine test results, were collected immediately before or during hospitalization for HD initiation. Body mass index (BMI) was calculated using the following formula: BMI = weight(kg)/height(m)2. Diabetes mellitus was defined as fasting blood glucose ≥126 mg/dL, casual blood glucose ≥200 mg/dL, HbA1c (NGSP) ≥ 6.5%, use of insulin, or use of oral hypoglycemic agents. A history of CV disease (CVD) was defined as a history of heart failure requiring hospitalization, coronary artery intervention, heart bypass surgery, stroke, aortic disease requiring surgery, or peripheral artery disease requiring hospitalization. Urgent dialysis was defined as emergency dialysis or dialysis initiation using an indwelling vascular catheter when faced with a risk to life. Emergency dialysis initiation was referred to as unscheduled initiation. The estimated glomerular filtration rate (eGFR) was calculated using the Japanese Society of Nephrology’s equation: eGFR = 194 × serum creatinine–1.094 × age–0.287 (×0.739 for women). The use of diuretics before dialysis initiation included regular loop diuretics, thiazide-type diuretics, or spironolactone [14, 15]. The use of RASIs was defined as the use of ACEIs or ARBs. We divided patients into four groups according to the patterns of RASIs use 3 months before and at the time of HD initiation: continued, stopped, did not use, and started during the 3 months prior to HD initiation [16]. Patients with missing this information were assigned to the unknown group (Supplementary Table 1).
Outcomes
The study outcomes were all-cause mortality and CV events after HD initiation. CV events were defined as heart failure, acute coronary syndrome, stroke, or peripheral artery disease requiring hospitalization [15]. Outcome data of all patients in this cohort were collected by reviewing the medical records of the AICOPP group or by sending letters to each dialysis clinic where patients were transferred for maintenance HD. Patients were followed up from the day of dialysis initiation, until either death, failure to follow-up, kidney transplantation, recovery from dialysis therapy, or the end of follow-up on September 30, 2016 [17].
Statistical analysis
The baseline characteristics of the cohort for survival analysis were summarized into two groups: continuing RASIs and stopping RASIs, with normally and non-normally distributed variables and categorical variables as mean (standard deviation [SD]), median (interquartile range [IQR]), and number (percentage), respectively. Group differences were assessed using Student’s t test, Wilcoxon rank sum test, and chi-square test for continuous variables with approximately normal distributions, non-normally distributed variables, and categorical data, respectively.
We estimated survival across the two groups using the Kaplan–Meier method. Differences in survival estimates between the two groups were assessed using the log-rank test. We performed analyses using multiple imputations by chained equations in the multivariable models to handle missing data. We performed chained equations with 100 imputations and combined the estimates of the analysis per dataset using Rubin’s rule. After multiple imputations, we constructed the multivariable Cox proportional hazard models to assess the risk of mortality and CV events associated with stopping RASIs and clinical characteristics. Three models were explored: Model 1 was unadjusted; Model 2 was adjusted for age, sex, BMI, history of diabetes mellitus, and history of CVD; and Model 3 additionally accounted for serum creatinine, serum potassium, eGFR decline (the change in eGFR for 3 months before dialysis initiation), and use of ion exchange resin, antiplatelet drugs, β-blockers, diuretics, and urgent dialysis. As sensitivity analyses for CV events in the stopping RASIs group, we performed Fine and Gray competing-risk analyses considering non-CV death as a competing risk. In case of significant association between mortality or CV events, and stopping RASIs, subgroup analyses according to age (<75 vs. ≥75 years), sex, diabetes mellitus, and history of CVD were performed.
In all analyses, a two-sided p-value of <0.05 was considered statistically significant. All the statistical analyses were performed using Stata version 17 (StataCorp, College Station, Texas, USA).

留言 (0)