
記住我






Thyroid dysfunction (TD) is associated with an increased risk of cardiac arrhythmias, atherosclerotic vascular disease, and heart failure (HF) [1,2]. It has also been associated with a higher risk of premature morbidity and death [3–7] as well as with an increased incidence of CV risk factors such as hypertension, diabetes, and dyslipidemia [8,9]. Moreover, TD is now recognized as a CV risk factor [10]. Thus, undiagnosed TD may constitute additional risk in patients predisposed to cardiovascular diseases (CVDs). Accordingly, screening CVD high-risk patients for TD and treating them accordingly, seems to be justified [10].
Despite the frequent occurrence of CVD comorbidities in patients with TD, few studies have assessed the level of thyroid hormones in the general cardiac population at acute admittance. Moreover, the prevalence of TD among the population varies in different studies and can be influenced by several factors such as age, sex, ethnicity, and iodine status [11]. It is estimated that the prevalence of TD globally is approximately 5% [12]. Data on the incidence of TD in Middle Eastern countries is limited [13].
To address this gap, we analyzed medical records of all hospitalized cardiac patients in a single tertiary medical center in Jerusalem, Israel, over 12 years. We sought to investigate the prevalence of TD and its association with CVD and other risk factors. We also sought to investigate whether the thyroid stimulation hormone (TSH) level on admission has a predictive value for long-term outcomes.
Materials and methods Study populationThis study was a single-center retrospective cohort study of consecutive adult patients who were admitted to the Cardiology Department and Cardiac ICU (CICU) of Jesselson Integrated Heart Center at Shaare Zedek Medical Center (SZMC), Jerusalem, Israel, over a 12-year period from 1 January 2005 to 1 May 2017.
The study was approved by the Institutional Ethical Committee of SZMC (Application number: 0035-19-SZMC) at Jerusalem, Israel (Chairperson Prof A. Steinberg) on 26 February 2019.
The Statistical Package for the Social Sciences (SPSS) software (IBM, Armonk, NY) was used to analyze the medical records of patients ≥18 years of age who were acutely admitted during the study period. Patients were excluded from the analysis if the TSH data was missing. For patients who were admitted more than once over the study period, only the first admission was included in the analysis. The flowchart in Supplementary Figure S1, Supplemental digital content 1, https://links.lww.com/CAEN/A56 shows the process followed to select and categorize the study population.
Data collection and outcomesData on demographic characteristics, medical history, conventional CV risk factors, medications, laboratory test results, and TSH measurements, were collected for analysis. In addition, the length of stay (LOS) in hospital, discharge diagnoses and procedures were abstracted from the discharge summaries of the patients’ electronic medical records by a single investigator. The primary admission diagnoses could not be determined. Data on survival after discharge from January 2005 to May 2017 were derived from the National Population Registry of the Israel National Statistical Office by using unique identifiers.
Measurement and definitions of thyroid functionAs part of the routine clinical procedure, the level of TSH was measured in blood collected on the day after admission. Free thyroxine (fT4) and free triiodothyronine (fT3) were measured only in those patients with a markedly abnormal level of TSH or if the measurements were requested by the treating physician or senior endocrinologist. Serum TSH, fT4 and fT3 were measured by chemiluminescence immunoassay using the Architect i2000SR immunoassay analyzer. The reference values were 0.35–5.0 mIU/L for TSH, 0.7–1.48 ng/dl for fT4 and 1.71–3.71 pg/ml for fT3.
In clinical routine, screening is frequently performed using TSH only [14]. Therefore, the patients were categorized retrospectively into five subgroups based on TSH level at admission as follows: normal TSH (0.35–5.0 mIU/L), markedly reduced TSH (≤ 0.1 mIU/L), mildly reduced TSH (0.1 < TSH < 0.35 mIU/L), mildly elevated TSH (5.0 < TSH < 10.0 mIU/L), and markedly elevated TSH (> 10.0 mIU/L).
Statistical analysisUsing SPSS, baseline characteristics and outcomes including LOS and mortality rate were reported in number and percentage for categorical variables and in mean ± SD or median (interquartile range [IQR]) for continuous variables. Continuous variables were compared using one-way analysis of variance or the Kruskal–Wallis test, and the categorical variables were compared using the chi-square test. The TSH levels were analyzed as continuous variables after natural logarithmic transformation to normalize distribution.
Stepwise multivariate logistic regression analysis was used with the normal TSH subgroup as the reference to calculate the odds ratio (ORs) to identify demographic and clinical factors associated with abnormal TSH level (TSH < 0.35 or > 5.0 mIU/L) and to examine the association between prolonged LOS (defined as > 5 days) and TSH level. The regression model included variables that showed statistical significance or that were known to be clinically relevant such as age, sex, smoking status (current or previous), chronic kidney disease (CKD) and presence of diabetes (DM), dyslipidemia, pacemaker/implantable cardioverter defibrillator (ICD)/cardiac resynchronization therapy (CRT), amiodarone use, levothyroxine use, hypertension (HTN), myocardial infarction (MI), HF and atrial fibrillation/flutter (AF). Results were presented as adjusted ORs (AdjORs) at a 95% confidence interval (CI). Long-term survival was estimated by Kaplan–Meier analysis, and differences in survival were assessed using the log-rank test. The Cox proportional hazards model was used to estimate the hazard ratio (HR) of each TD subgroup. The HRs were adjusted for the same clinically relevant covariates mentioned above, using normal range TSH as the reference. All analyses were two-tailed. A value of P < 0.05 was considered statistically significant.
ResultsThere were 31 909 acute admissions to the Cardiology Department and CICU between 1 January 2005 to 1 May 2017. Among them, 14369 met the inclusion criteria.
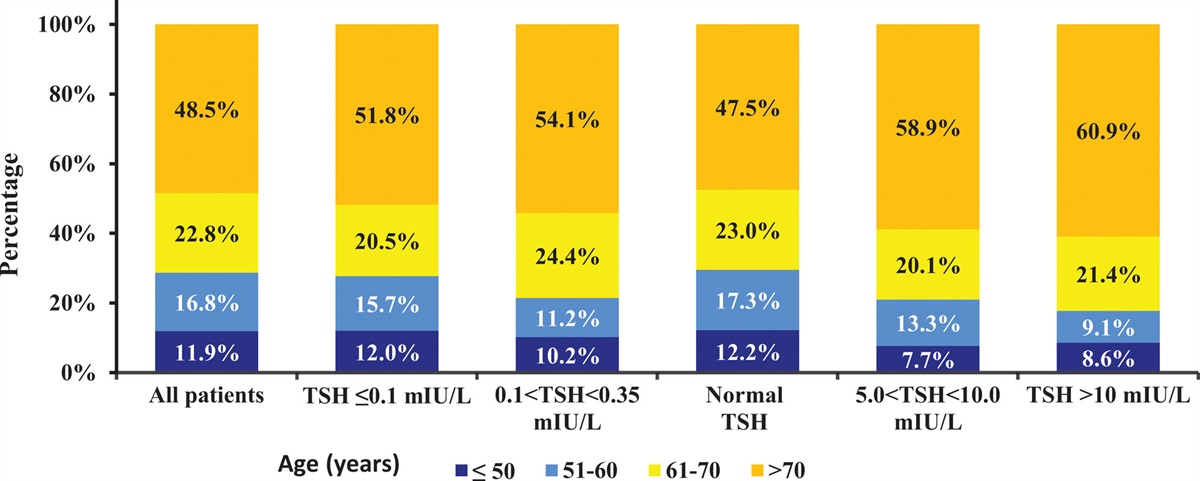
Baseline characteristicsTable 1 shows the baseline characteristics of the study population as a whole and by TSH subgroup. The mean (± SD) age was 67 ± 15 years, 38.3% of patients were women and 48.5% were older than 70 years. The mean (median) level of TSH at admission was 2.42 (3.54) mIU/L.
Table 1 - Baseline characteristics of study population by TSH level Characteristic Overall TSH, mIU/L P-value Markedly reducedData are presented as means ± standard deviations or as median (interquartile ranges [IQRs]) for continuous variables and as numbers with proportions for categorical variables.
P-values are derived from one-way ANOVA models for continuous variables and from chi-square tests for categorical variables.
Valid cases for variables (n = 14369; 100%) with exception for medications (n = 14113; 98.2%).
A P-value of < 0.05 indicates a significant difference when compared with normal TSH level (0.3501–5.0 mIU/L).
CABG, coronary artery bypass graft; CRT, cardiac resynchronization therapy; ICD, implantable cardioverter defibrillator; LV, left ventricle; PCI, percutaneous coronary intervention; TSH, thyroid stimulating hormone.
A total of 12 904 (89.8%) individuals had a TSH level within the normal range and 1465 (10.2%) had TD. Among the 1465 patients with TD, the mildly elevated TSH subgroup was the largest (n = 776; 5.4%) followed by the mildly reduced TSH (n = 303; 2.1%), markedly elevated TSH (n = 220; 1.5%) and markedly reduced TSH (n = 166; 1.2%) subgroups.
Table 1 shows that compared with the reference group (normal TSH of 0.35–5.0 mIU/L), patients with TD were more likely to be female (P < 0.001), older than 70 years (P < 0.001), to have a history of smoking (P < 0.001), essential HTN (P = 0.03), dyslipidemia (P = 0.01), HF (P < 0.001), AF (P < 0.001), pulmonary hypertension (P < 0.001), CKD (P < 0.001) and cardiac pacemaker/ICD/CRT (P < 0.001). TD patients were also more likely to be taking levothyroxine or amiodarone (P < 0.001).On the other hand, no significant association was found between TD and a history of coronary artery disease (CAD), DM or stroke/transient ischemic attack.
The data analysis also revealed that a small number of patients were taking other medications than Amiodarone and thyroid preparations that could interfere with thyroid function tests, namely, glucocorticoids (n = 264; 1.9%), carbamazepine (n = 65; 0.5%), phenytoin (n = 23; 0.2%), and lithium (n = 14; 0.1%). In addition, a small number of patients had supraventricular tachycardia (n = 207; 1.5%) or ventricular tachycardia/fibrillation (n = 168; 1.2%). However, due to the small numbers, the differences between the subgroups were statistically insignificant For other related clinical and laboratory characteristics see Supplementary Table S1, Supplemental digital content 2, https://links.lww.com/CAEN/A57.
Figure 1 shows the levels of TSH by age group (≤ 50, 51–60, 61–70 and > 70 years). It can be seen that there was a significant increase in TSH level with increasing age, with a higher prevalence of TD in patients aged > 70 years compared to those aged < 70 years (P < 0.001), particularly among the markedly elevated TSH subgroup.
 Fig. 1:
Fig. 1: TSH distribution by age group.
The association between thyroid dysfunction and cardiovascular diseasesTable 2 shows the results of the multivariate logistic regression analysis performed to identify the associations between an abnormal TSH level (TSH < 0.35 or > 5 mIU/L) and clinical characteristics. After adjusting for potential confounders, female gender (OR = 1.25), levothyroxine use (OR = 3.55), amiodarone use (OR = 1.96), history of HF (OR = 1.28), AF (OR = 1.24), and CKD (OR = 1.291) were significantly associated with abnormal TSH levels.
Table 2 - Associations between abnormal TSH levels and patient characteristics by multivariate logistic regression model Covariate AdjOR 95% CI for OR P-value Age, >70 years 1.00 0.99–1.01 0.01 Gender (female) 1.25 1.09–1.41 0.001 Smoking 1.01 0.88–1.17 0.88 Hypertension 0.95 0.83–1.09 0.49 Diabetes 1.02 0.90–1.16 0.72 Dyslipidemia 0.85 0.76–0.96 0.01 Myocardial infarction 1.17 1.00–1.37 0.047 Congestive heart failure 1.28 1.09–1.50 0.003 Atrial fibrillation/flutter 1.24 1.09–1.41 0.001 Renal failure 1.29 1.10–1.50 0.001 Presence of pacemaker/ICD/CRT 1.14 0.96–1.36 0.14 Levothyroxine use 3.55 3.07–4.11 < 0.001 Amiodarone use 1.96 1.60–2.41 < 0.001Notes: Adjusted for age, sex, smoking, hypertension, diabetes, dyslipidemia, myocardial infarction, congestive heart failure, atrial fibrillation/flutter, renal failure, presence of pacemaker/ICD/CRT, levothyroxine use, and amiodarone use.
Abnormal TSH level defined as TSH < 0.35 or >5 mIU/L.
Significance level defined as P < 0.05 at 95% CI.
AdjOR, adjusted odds ratio; CI, confidence interval; CRT, cardiac resynchronization therapy; ICD, implantable cardioverter defibrillator; TSH, thyroid stimulating hormone.
Among the 14369 patients, 2975 (20.7%) died over a mean follow-up of 1012 days (quartiles: 415–2008 days). Supplementary Figure S2, Supplemental digital content 1, https://links.lww.com/CAEN/A56 shows the Kaplan–Meier survival curves for mortality in the five TSH subgroups, with normal range TSH as the reference. It can be seen that there were significant differences in mortality among the five subgroups with the markedly elevated TSH group having the worst prognosis (P < 0.001; by the log-rank test).
Table 3 shows the results of the multivariate logistic regression model, which was adjusted for age, sex, smoking, CKD, presence of DM, dyslipidemia, pacemaker/ICD/CRT, amiodarone use, levothyroxine use, CVD, HTN, MI, HF, and AF, with normal range TSH as the reference. The analysis revealed a statistically significant highest mortality rate with mildly reduced TSH subgroup (HR = 1.44), followed by the markedly elevated TSH subgroup (HR = 1.40) and the mildly elevated TSH subgroup (HR = 1.27). Furthermore, the markedly reduced TSH had a lower mortality rate (HR = 0.79) than the normal TSH subgroup. However, this result was NS.
Table 3 - Hazard ratios for mortality rate by TSH level according to multivariate survival analysis TSH subgroup No. of deaths (%) AdjHR 95% CI for HR P-value Normal TSH 2531/12904Each predictor was separately entered in a Cox regression model, adjusted for age, sex, smoking, hypertension, diabetes, dyslipidemia, myocardial infarction, congestive heart failure, atrial fibrillation/flutter, renal failure, presence of pacemaker/ICD/CRT, levothyroxine use, and amiodarone use.
Cox survival analysis was taken with the normal range TSH (0.3501–5.0) as the reference group.
Significance was defined as P < 0.05 at 95% CI.
AdjHR, adjusted hazard ratio; CI, confidence interval; TSH, thyroid stimulating hormone.
The median LOS was 5 days (IQR 4–7 days). Figure 2 shows the association between LOS and TSH level. It can be seen that the markedly elevated subgroup had the longest LOS (9.2 ± 8.05 days) followed by the mildly reduced TSH subgroup (8.1 ± 8.8 days).
 Fig. 2:
Fig. 2: Length of hospital stay (LOS) by TSH level. Notes: Multivariate analysis was taken with the normal range TSH (0.3501–5.0) as the reference group. Adjusted for age, sex, hypertension, smoking, hypertension, diabetes, dyslipidemia, myocardial infarction, congestive heart failure, atrial fibrillation/flutter, renal failure, presence of pacemaker/ICD/CRT, levothyroxine use and amiodarone use. *Significant difference between this group and the reference group. Significance was defined as P < 0.05.
In multivariate logistic regression for the association between prolonged LOS (> 5 days) and TSH level, there was an association between TD and prolonged LOS, with the longest LOS among those with markedly elevated TSH (adjOR = 1.69), followed by those with mildly reduced (adjOR = 1.38) and mildly elevated TSH (adjOR = 1.18). A markedly reduced TSH had no significant impact on prolonged LOS (Supplementary Table S2, Supplemental digital content 2, https://links.lww.com/CAEN/A57).
DiscussionTD is common in the general population and the heart is a major target for thyroid hormone action. The most important findings of the study are: (a) TD prevalence is 10.2% in critically ill patients admitted to the cardiology department and CICU; (b) cardiac patient subgroups with a particularly increased incidence of TD, include females, patients with HF, CKD or AF, and patients taking amiodarone or levothyroxine; (c) TSH at admission was a predictor of mortality and LOS in these patients, and the association was independent of traditional risk factors.
There is a huge variability in the epidemiology of TD worldwide [11]. The National Health and Nutrition Examination Survey III identified a prevalence of 4.6% and 1.3% for hypothyroidism and hyperthyroidism, respectively [15]. The Framingham study reported that 13.6% of women older than 60 years have TSH concentrations above 5.0 mIU/L [16]. A study in Israel evaluating 422 242 outpatients reported a TD prevalence of 5% [17], while another study in Israel assessing 17 440 individuals (average age 83 years, majority women) reported a higher prevalence of TD at 14.3%, 11% with subclinical hypothyroidism [18]. However, these studies used population-based samples. It is well known that both TD and CVD are common in the aging population and often coexist in the same individual. Lervasi et al. investigated 3121 patients admitted with acute forms of CVD and reported a prevalence of subclinical hypothyroidism (6.6%), subclinical hyperthyroidism (3.1%), and low T3 (29.2%) [19]. In a study among 963 patients with dilated cardiomyopathy, 7.1% had subclinical hyperthyroidism, 84.7% had euthyroidism, and 8.2% had subclinical hypothyroidism [20]. In our study, we found that almost half of the patients with TD were aged > 70 years, and there was an age-related increase in TD prevalence. Furthermore, TD was more common in women, and a mildly elevated TSH level was the most frequent dysfunction (5.4%). Our findings support previous evidence that TD is a common condition and is particularly prevalent in older women [21–23].
Several studies have examined the relationship between thyroid function and the incidence of CVD and its risk factors [1–9]. Among the many known comorbidities and risk factors, our study identified female sex, a diagnosis of HF, CKD or AF, amiodarone and levothyroxine usage as significantly associated with abnormal TSH levels. Furthermore, the associations remained statistically significant even after adjusting for the baseline CV risk profiles. This observation is in accordance with other studies showing a strong correlation between TD and these variables [24–30].
Previous studies on the association of TSH levels with the incidence of CAD and stroke found conflicting findings. Some studies showed that there is an increased incidence of CAD and stroke In patients with TD [4,5,31–34], others did not [35–38]. In our study, we failed to find a statistically significant association between the incidence of CAD or stroke with TD. Concordant with our study, Mendelian randomization studies found no indication of an association between TD and CAD [35,37]. Langen et al. [37] found no association between hyperthyroidism or hypothyroidism with stroke. Furthermore, the meta-analysis by Møllehave et al. [38] found no evidence of a harmful effect of decreased or increased TSH on CAD or stroke in the general population, as in our study.
In our study, we found an association between TSH and mortality. The highest mortality occurred among patients with mildly reduced TSH levels (0.1 < TSH < 0.35 mIU/L). This is in good agreement with the results of recent updated meta-analyses which found an increased mortality risk in overt and subclinical hypothyroidism [32,39].
With respect to decreased serum TSH levels, our study found that patients with overt hyperthyroidism (TSH ≤ 0.1 mIU/L) had a lower mortality risk than those with normal TSH levels; however, these results were NS. These findings are surprising and may, at first, appear to be counterintuitive. Yet, interestingly, these findings are consistent with studies that showed no association between overt hyperthyroidism and mortality [23,35,40–42]. In a study comparable to ours, Langen et al. [37] found no association between lower levels of TSH and mortality or CV morbidity among 5211 participants from the general population. Furthermore, a study by Qari et al. [43] that evaluated 502 ICU patients found a lower mortality risk with TSH < 0.1 mIU/L compared to those with normal thyroid function. Conversely, Parle et al. [40] found an association between overt hyperthyroidism and the risk of total mortality in their large study. In another study by Collet et al., subclinical hyperthyroidism has been linked to an increased risk for total and CAD mortality [5].
In addition to mortality, our retrospective cohort study showed that baseline TSH had a U-shaped longitudinal association with LOS. TSH levels higher than 10 mIU/L are associated with a LOS. A potential relationship was observed for reduced TSH (< 0.1) but was diminished after adjusting to variables. There are only a few published articles which have investigated this association, our study supports these findings. A study by Omelyanenko et al. [44] evaluated 40 ICU patients with pneumonia and found that longer in-hospital stay was associated with higher TSH and lower fT4 values on admission. In contrary, Qari et al. [43] found that the ICU length of stay was the longest for hyperthyroid patients, while those with hypothyroidism had the shortest stay.
Strengths and limitations of the studyOur study has many strengths, including the use of a very large database, extensive statistical and sensitivity analyses contributing to the validity of the data and a careful assessment of longitudinal outcomes.
It should be noted that this study has some limitations. First, the study is a retrospective analysis of data from a single medical center and is therefore subject to all the limitations that apply to this type of study. Second, TSH data was missing for some of the patients, possibly due to laboratory errors and incomplete or missing blood samples. Third, in this study population, TSH tests were performed at times of acute illness and this may have affected the laboratory results due to the impact of euthyroid sick syndrome (ESS), which is characterized mainly by low T3 levels with low or normal TSH levels. However, a close examination of patients with low TSH levels (< 0.1) tested for ft3 as well showed that only 3.3% had low free T3 levels (Supplementary Table S3, Supplemental digital content 2, https://links.lww.com/CAEN/A57), suggesting that ESS cannot explain the majority of low TSH level results in this cohort. Fourth, this study focused mainly on the results of a single screening TSH test. Thus the number of patients whose thyroid function may have normalized spontaneously or progressed to overt hypothyroidism or hyperthyroidism is unknown. Finally, the lack of data regarding the specific cause of death renders it impossible to determine related mechanism.
ConclusionThis study revealed that among patients hospitalized with acute CVD, there is a prevalence of TD amounting to 10.2%. Notably, TD is more prevalent in patients with a history of hypothyroidism, those undergoing levothyroxine treatment, females, individuals diagnosed with HF, AF, and CKD, as well as those receiving amiodarone therapy. Furthermore, cardiac patients with TD exhibited poorer overall survival rates and longer hospital stays in comparison to individuals with normal TSH levels. These findings suggest that assessing TSH levels could serve as a potent tool for predicting mortality and determining the length of hospitalization in cardiac patients. Consequently, it is advisable for cardiology departments, particularly for high-risk groups, to consider implementing routine screening for TD. This screening is both cost-effective and readily accessible, and further research is warranted to explore whether optimizing thyroid function can provide benefits to these patients.
AcknowledgementsWe thank Ms. Farkash Rivka for her contribution to electronic medical record data retrieval and statistical analyses.
Conflicts of interestThere are no conflicts of interest.
References 1. Jabbar A, Pingitore A, Pearce SH, Zaman A, Iervasi G, Razvi S. Thyroid hormones and cardiovascular disease. Nat Rev Cardiol 2017; 14:39–55. 2. Razvi S, Jabbar A, Pingitore A, Danzi S, Biondi B, Klein I, et al. Thyroid hormones and cardiovascular function and diseases. J Am Coll Cardiol 2018; 71:1781–1796. 3. Singh S, Duggal J, Molnar J, Maldonado F, Barsano CP, Arora R. Impact of subclinical thyroid disorders on coronary heart disease, cardiovascular and all-cause mortality: a meta-analysis. Int J Cardiol 2008; 125:41–48. 4. Rodondi N, den Elzen WP, Bauer DC, Cappola AR, Razvi S, Walsh JP, et al.; Thyroid Studies Collaboration. Subclinical hypothyroidism and the risk of coronary heart disease and mortality. JAMA 2010; 304:1365–1374. 5. Collet TH, Gussekloo J, Bauer DC, den Elzen WP, Cappola AR, Balmer P, et al.; Thyroid Studies Collaboration. Subclinical hyperthyroidism and the risk of coronary heart disease and mortality. Arch Intern Med 2012; 172:799–809. 6. Selmer C, Olesen JB, Hansen ML, von Kappelgaard LM, Madsen JC, Hansen PR, et al. Subclinical and overt thyroid dysfunction and risk of all-cause mortality and cardiovascular events: a large population study. J Clin Endocrinol Metab 2014; 99:2372–2382. 7. Kannan L, Shaw PA, Morley MP, Brandimarto J, Fang JC, Sweitzer NK, et al. Thyroid dysfunction in heart failure and cardiovascular outcomes. Circ Heart Fail 2018; 11:e005266. 8. Talwalkar P, Deshmukh V, Bhole M. Prevalence of hypothyroidism in patients with type 2 diabetes mellitus and hypertension in India: a cross-sectional observational study. Diabetes Metab Syndr Obes 2019; 12:369–376. 9. Klein I, Danzi S. Thyroid disease and the heart. Circulation 2007; 116:1725–1735. 10. Cappola AR, Desai AS, Medici M, Cooper LS, Egan D, Sopko G, et al. Thyroid and cardiovascular disease: research agenda for enhancing knowledge, prevention, and treatment. Thyroid 2019; 29:760–777. 11. Taylor PN, Albrecht D, Scholz A, Gutierrez-Buey G, Lazarus JH, Dayan CM, et al. Global epidemiology of hyperthyroidism and hypothyroidism. Nat Rev Endocrinol 2018; 14:301–316. 12. Vanderpump MP. The epidemiology of thyroid disease. Br Med Bull 2011; 99:39–51. 13. Al Shahrani AS, El-Metwally A, Al-Surimi K, Salih SB, Saleh Y, Al-Shehri A, et al. The epidemiology of thyroid diseases in the Arab world: A systematic review. J Public Health Epidemiol 2016; 8:17–26. 14. Jonklaas J, Bianco AC, Bauer AJ, Burman KD, Cappola AR, Celi FS, et al.; American Thyroid Association Task Force on Thyroid Hormone Replacement. Guidelines for the treatment of hypothyroidism: prepared by the American Thyroid Association task force on thyroid hormone replacement. Thyroid 2014; 24:1670–1751. 15. Hollowell JG, Staehling NW, Flanders WD, Hannon WH, Gunter EW, Spencer CA, et al. Serum TSH, T(4) and thyroid antibodies in the United States population (1988 to 1994): National Health and Nutrition Examination Survey (NHANES III). J Clin Endocrinol Metab 2002; 87:489–499. 16. Sawin CT, Castelli WP, Hershman JM, McNamara P, Bacharach P. The aging thyroid Thyroid deficiency in the Framingham Study. Arch Intern Med 1985; 145:1386–1388. 17. Meyerovitch J, Rotman-Pikielny P, Sherf M, Battat E, Levy Y, Surks MI. Serum thyrotropin measurements in the community: five-year follow-up in a large network of primary care physicians. Arch Intern Med 2007; 167:1533–1538. 18. Grossman A, Weiss A, Koren-Morag N, Shimon I, Beloosesky Y, Meyerovitch J. Subclinical thyroid disease and mortality in the elderly: a retrospective cohort study. Am J Med 2016; 129:423–430.
留言 (0)