
記住我

A 65-year-old Japanese woman with cerebellar malformation identified during a medical checkup was referred to our hospital for further evaluation. Her medical history was unremarkable. She was born to nonconsanguineous parents from neighboring towns and had healthy siblings. She had mild intellectual disability but had graduated junior high school and worked in factories. She was a slow runner during childhood and had difficulty walking in her early 60 s, with a slow, broadly based gait. At 64 years of age, she noticed memory loss and attention deficits. At 65 years of age, during a general medical examination, she was diagnosed with cognitive impairment and cerebellar hypoplasia on brain magnetic resonance imaging (MRI). She denied having any muscle weakness or dyspnea. She was subsequently admitted to our hospital for further evaluation.
Neurological examination revealed vision loss in the left eye, left conductive hearing loss, impaired smooth pursuit of eye movement, mild cerebellar ataxia in the trunk and limbs, and hyperreflexia in the lower extremities. She also had a cataract in her left eye, but myopia and retinal involvement were unremarkable. The results of cognitive function assessment were as follows: 22/30 points on the Mini-Mental Scale Examination; 16/30 points on the Montreal Cognitive Assessment; and visual IQ: 75, performance IQ: 71, and full-scale IQ: 70 on the Wechsler Adult Intellectual Scale third edition. Blood test results revealed no abnormal findings. Brain MRI revealed multiple cysts in the antero-superior vermis and posterior-superior aspects of the hemispheres, cerebellar dysplasia, vermis hypoplasia, rhomboid shaped fourth ventricle, splayed superior cerebellar peduncles, and short pons (Fig. 1); however, supratentorial anomalies were absent. Diffusion tensor imaging showed preservation of the superior cerebellar peduncles decussate. Brain SPECT imaging, computed tomography, and whole-exome sequencing and filtering analysis revealed cerebellar hypoperfusion, absent cystic lesions or situs inversus, and a rare homozygous variant of c.1711_1712del in LAMA1 (NM_005559.4), which lead to p. Ala571Profs*8 (NP_005550.2), respectively. Based on these clinical and genetic test results, the patient was finally diagnosed with PTBHS.
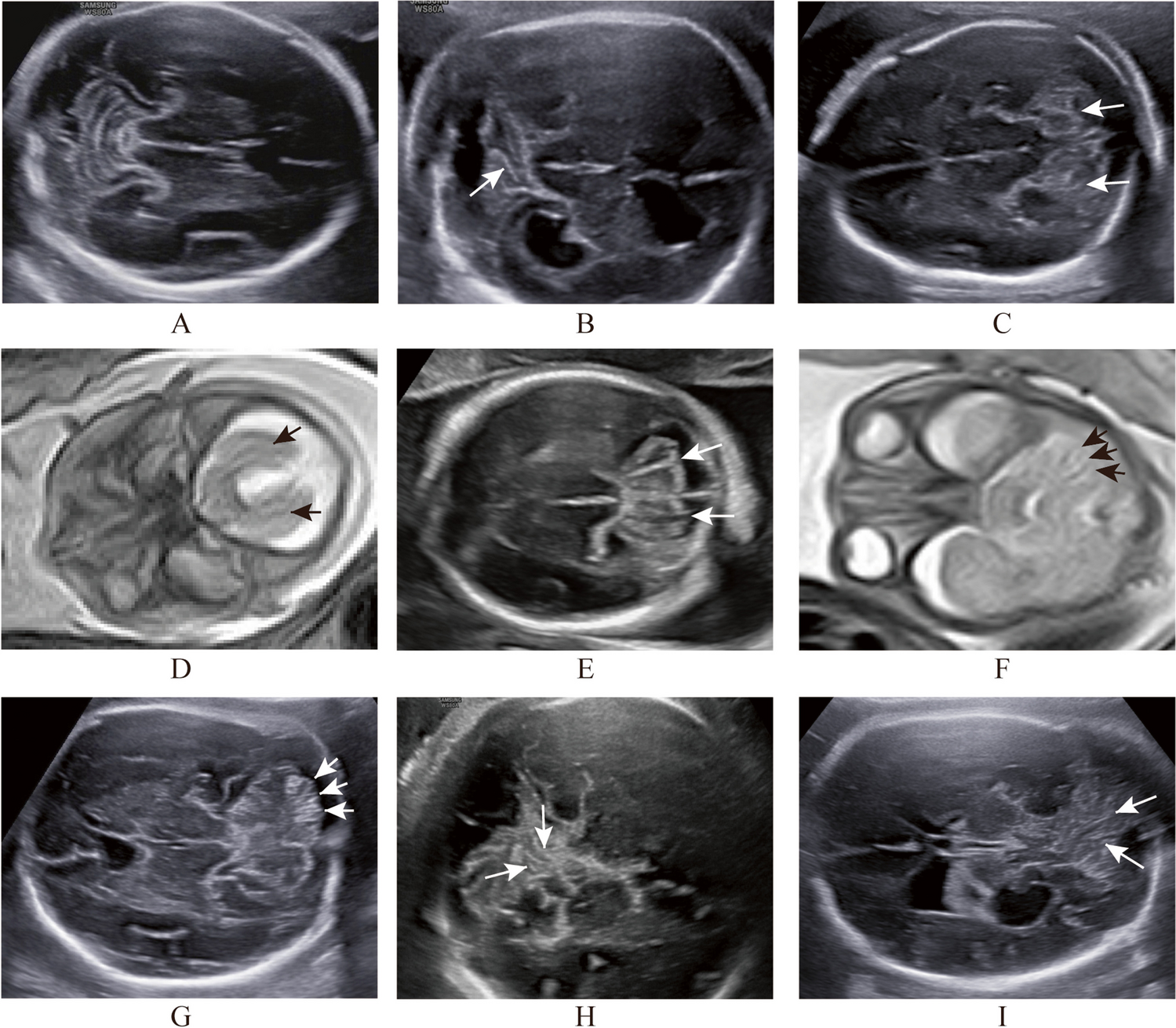
Fig. 1
Magnetic resonance images (MRI): A Axial T1-weighted MRI, B Axial T2-weighted MRI, C Coronal T1-weighted MRI, and D Sagittal T1-weighted MRI. These images show elongated superior cerebellar peduncles without thickness or straight shape (A), multiple cerebellar cysts (B), splayed superior cerebellar peduncles (C), vermis hypoplasia, and rhomboid shaped fourth ventricle (D)
留言 (0)