The aim of this study was to use the ADLIR score to assess the functional internal rotation after a minimum follow-up of 2 years following RSA without SSc reattachment. The median ADLIR score was 88 (IQR: 81–96) and 79% of the patients had a score of 79 or higher (considered a satisfactory score). Only one patient (0.5%) required a revision for a dislocation. None of the analysed factors were significantly associated with the ADLIR score in the regression model. Overall, these findings demonstrate that satisfactory results in terms of functional internal rotation at a midterm follow-up can be achieved with RSA without SSc reattachment, along with low rates of instability. Considering the importance of internal rotation in daily activities, these results suggest that the patient’s satisfaction and quality of life are not likely to be impacted by a limitation on the internal range of motion after RSA.
Functional internal rotation
Few previous studies have evaluated postoperative functional internal rotation using a patient-reported score. Beckers et al. reported a mean postoperative ADLIR score of 88 at a minimum of 2 years follow-up in a small cohort who had undergone RSA without SSc reattachment [2]. The outcomes of this pilot study are congruent with the current study. Only two other studies investigated the ADLIR score after RSA. However, they included patients who underwent RSA combined with a tendon transfer, which is not comparable to the current cohort [1, 36]. The results per question in the current study also revealed that patients consider that their loss of internal rotation slightly affects their general shoulder function and that reaching the back poses a slight difficulty for most patients, but other movements and activities generally pose no difficulty for patients. Consequently, in the case of generally positive results, questions 4 to 9 do not seem to contribute to the total result; they would only be discriminative in the case of poorer results. The first question of the questionnaire, which evaluates shoulder function in internal rotation globally, highly influences the final result. The interpretation of this question may also prove difficult for some patients. Therefore, developing a more specific questionnaire that includes more detailed questions could be considered.
To our knowledge, no previous study has compared the postoperative functional internal rotation between reattachment and no reattachment of the SSc during RSA. However, several studies have compared the clinical ROM between the two techniques. The reported results are contradictory; some studies reported no significant difference between the two groups [11, 22, 26, 32, 39], while other studies suggest that leaving the SSc tendon detached in RSA leads to a loss of internal rotation [16, 38]. Engel et al. described a loss of 8° in ROM in internal rotation when the SSc tendon was not repaired compared to when the SSc tendon was repaired in a small randomised cohort of 50 patients with a follow-up of 1 year [16]. Similarly, Rohman et al. identified that not repairing the SSc was a risk factor for a loss of internal rotation in a large cohort of patients [38]. However, a logistic regression was used for loss of and increase in internal rotation, and no direct comparison of internal rotation between patient groups with and without SSc repair is reported. The exact role of the SSc muscle after RSA remains disputed. Although no comparison could be made between SSc reattachment and no reattachment in the current study, we report a median level of internal rotation reaching the 3rd lumbar vertebra. This result is similar to previous studies reporting internal rotation using anatomical landmarks, regardless of the handling of the SSc. Two studies reported the internal rotation of the entire cohort without making a distinction based on the handling of the SSc. Rohman et al. reported that the mean level reached was lumbar vertebrae 4–5, and Rol et al. reported that the lumbosacral region was the mean level reached [38, 39]. These findings suggest that the postoperative internal rotation in our cohort may be equal or superior to the overall outcomes in the literature, regardless of SSc reattachment.
The majority of the humeral components (85%) were placed in 30° of retroversion. One biomechanical study reported a significant decrease in ROM in internal rotation with greater retroversion (p < 0.05) [3]. In contrast, a retrospective study comparing RSA placed in 20° of retroversion with 0° found no difference in ROM or difficulty in activities of daily living with the exception of difficulty in washing the back and fastening a bra behind the back, which was more difficult with 20° of retroversion (p = 0.026) [37]. A similar retrospective study found no difference in ROM, strength, Constant score or Oxford score when comparing 0° and 20° of retroversion [12]. Degrees of retroversion was not significantly associated with ADLIR or ROM (outcomes) in the regression models. However, the majority of the components were placed in 30° of retroversion, resulting in a homogeneous cohort that was not suitable for a comparison between different grades of retroversion. Our results show that the internal rotation is satisfactory when the humeral component is placed in 30° of retroversion in most cases. A recent computer-assisted study by Hochreiter et al. reported the ideal component placements in order to obtain the best range of motion in internal rotation; the largest impingement-free functional internal rotation was achieved when combining a posteroinferior baseplate position, a greater inferior glenosphere overhang, a baseplate inclination angle of 90°, 6 mm of glenosphere lateralisation with respect to the baseline setup, a lower NSA and anteversion of the humeral component [23].
In the current study, with regards to regression analysis with ADLIR score as the outcome, none of the factors were associated with the ADLIR score, although age and smoking approached significance (0.0677 and 0.0594, respectively).
Stability
Another commonly voiced concern of leaving the SSc tendon detached is humeral joint instability. Edwards et al. compared 62 patients with a reparable SSc to 76 patients with an irreparable SSc [15]. All seven of the postoperative dislocations occurred in the group in which the SSc was irreparable. The authors suggest that an attempt to repair the SSc should be made in every case. However, in this study, the non-SSc-repair population consisted of complex cases in which the SSc was irreparable, resulting in a selection bias. Dislocations are more likely in patients with complex diagnoses, including proximal humeral non-union, fixed glenohumeral dislocation and failed prior arthroplasty. In contrast, in our study, only one dislocation occurred among the 210 patients meeting the inclusion criteria. The dislocation occurred 28 days after surgery. The diagnosis for the primary RSA was osteonecrosis of the proximal humeral head after plate fixation 2 years earlier. The patient underwent revision surgery with replacement of the polyethylene insert. To our knowledge, two meta-analyses explored SSc status in RSA as risk factor for dislocation. One study reported a higher dislocation risk in the case of SSc deficiency. The odds ratio for dislocation was 18.43 (p = 0.0006) [29]. The other study explored the influence of SSc repair on dislocation. This study showed no significant difference in risk of dislocation between repair and no repair of the SSc. The dislocation rate was 1.6% in patients with no repair of the SSC and 0.8% in patients with a repair (OR [95% CI] − 0.70 [− 1.82, 0.41] [13]. The differences between the dislocation rates in the literature could be attributed to the use of a different prothesis design or different surgical techniques, along with the placement of the humeral component for which the retroversion was above 20° in 93% of the cases in our cohort. Although humeral component retroversion is associated with decreased stability of the prosthesis in biomechanical studies [17], the high degree of humeral component retroversion in our cohort did not seem to translate to increased dislocation rates. Some other factors could have influenced the observed outcomes, such as the degree of glenoid version, the follow-up time, or the postoperative protocol. In our cohort it was not statistically feasible to analyse the influences of these factors in detail due to the low number of dislocations.
External rotation
Reattachment of the SSc has been suggested to restrict the ROM in external rotation [40]. The median ADLER score in our study was 30, showing that there was excellent functional external rotation in patients who had undergone RSA without SSc reattachment. To our knowledge, there are no studies investigating the role of the SSc in RSA that report the ADLER score as an outcome. Two studies investigating RSA combined with a tendon transfer reported the ADLER score [34, 50], but those are not comparable to our cohort, who underwent RSA alone. Nonetheless, the excellent ADLER score in our cohort may support the suggestion that the absence of the SSc tendon leads to a less restricted functional external rotation. However, this must be confirmed in a comparative study. Older age at the time of surgery and smoking were associated with a lower ADLER score in the regression analysis (Table 9). Previous studies did not find this correlation. One study comparing cohorts of younger (< 65 years) and older (> 70 years) patients found no difference in PROMs after RSA but a greater range of motion in the younger group [28]. In contrast, one study found higher ASES scores and greater internal rotation ROM in patients older than 60 years compared to younger patients [6]. The median age in the current cohort is notably higher (73 years), potentially explaining the incongruency. In contrast to our findings, one previous study found no difference in PROMs or ROM outcomes between smokers and non-smokers [46]. However, smoking may also be correlated with other factors not measured in the current study, such as socio-economic status, which is associated with worse outcomes [45].
Radiographic measurements
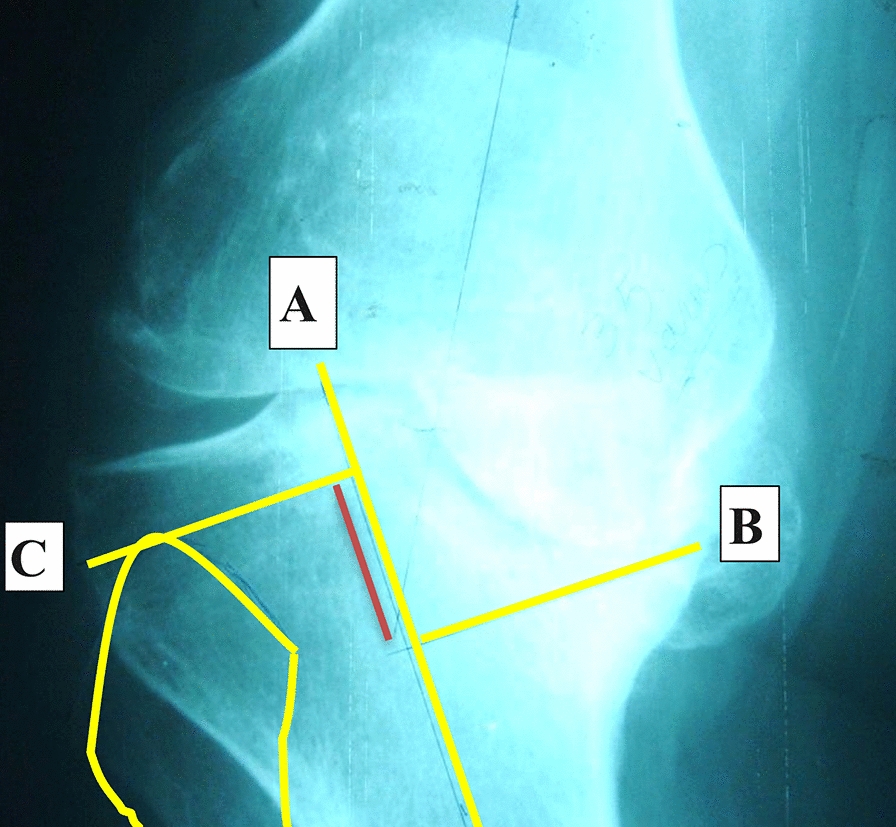
Boutsiadis et al. established the LSA and DSA as reproducible measurements to estimate lateralisation and distalisation after RSA, and they showed an interobserver agreement of 0.78 (substantial agreement) for LSA and 0.81 (almost perfect agreement) for DSA [5]. Our study showed similar results regarding interobserver agreement; 0.78 (substantial agreement) for LSA and 0.89 (almost perfect agreement) for DSA, confirming that the measurement of these angles is reliably reproducible. Thupé et al. showed lower interobserver agreement in patients who underwent RSA after a proximal humeral fracture; they report fair agreement for LSA and moderate agreement for DSA [43]. However, the authors attributed the lower agreement to the difficulty in analysing tuberosity position in patients who underwent RSA after proximal humeral fracture. Notably, the radiographic measurements (LSA, DSA and SBOD) were not significantly correlated with ADLIR or ROM results in the regression models, suggesting that the placement of the prosthesis, such as the baseplate positioning, amount of reaming and positioning of the humeral component, does not influence the (functional) internal rotation. However, this finding may also be attributed to the cohort size and homogeneity. It is possible that more significant associations may be found in a larger, more heterogeneous cohort. Furthermore, implant positioning is best assessed on computed tomography rather than plain radiographs.
Limitations
This study has several limitations to consider when interpreting the results. First, the patients were identified retrospectively. Since leaving the SSc tendon detached is standard practice at our centre, it was not possible to compare SSc reattachment with no reattachment. Preoperative assessment of the SSc was also not reported in our series. However, we were able to report detailed and satisfactory results of our technique, which can be compared with current and future literature. Other techniques that were used in a portion of the cases, such as BIO-RSA and tendon transfers, may also have influenced the outcome. Secondly, no preoperative scores were available, so we were not able to compare the postoperative to the preoperative outcomes. Third, in this study we used a single prosthesis design, with a 155° humeral neck-shaft angle and an inlay design. For the glenoid component, an inferior overhang of at least 5 mm is systematically created to avoid impingement, which leads to instability and notching. In the paragraphs above, we compare our results with other studies for which these parameters may be different. The single-prosthesis design and single technique used limit the generalisability of our outcomes but they do increase the internal validity of the study. Fourth, the radiographic measurements are dependent on the position of the arm and the angle at which the radiograph was taken. This may potentially introduce bias due to differences in the resting arm position between patients based on sex or BMI. However, the high interobserver agreement demonstrates the high reliability of the radiographic measurements. Furthermore, the position of the scapula on the thorax and the degree of lordosis were not taken into account, which may also have influenced the ROM in internal rotation [30, 31]. Additionally, the interpretation of the ADLIR questionnaire can differ between patients, potentially introducing a bias. For example, personal preferences and cultural differences may influence the movements required for daily activities such as personal hygiene. Lastly, the questionnaires were administered over the phone or by email, potentially introducing a bias based on the medium that was used. However, using several media to collect data resulted in a response rate of more than 80%, which allowed for the analysis of a large cohort and reduces the chance of bias due to non-responders or missing data.
Future perspective
Future prospective studies comparing the functional internal and external rotation in daily life between RSA cases with and without SSc reattachment are required to demonstrate the functional superiority of one of the two techniques. Furthermore, studies could compare outcomes between different prosthetic designs and surgical approaches. Longitudinal assessments with preoperative and postoperative scores may provide a more comprehensive understanding of patient outcomes.









留言 (0)