
記住我
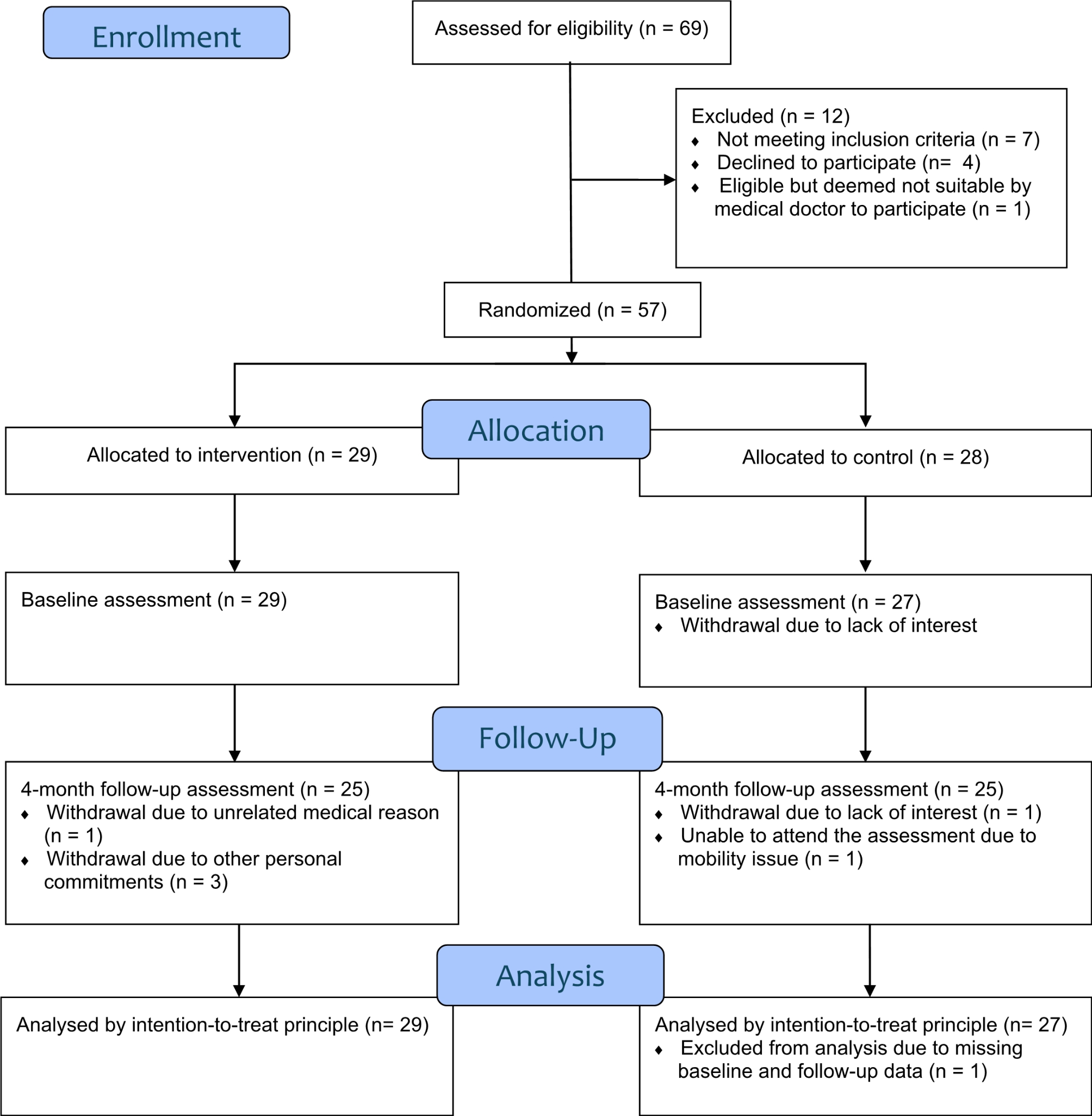








A total of 270 studies were retrieved, including 242 studies from databases, 19 studies from registers, and 9 studies from websites and citation searching. After excluding 87 duplicate studies, titles and abstracts were read, 145 irrelevant articles were excluded, and the full texts of the remaining studies were sought for reading and eligibility assessment. Finally, 35 studies were evaluated for inclusion, of which 26 studies were excluded for reasons (like stroke more than 3 months at the time of diagnosis, inappropriate intervention methods, not RCT), and 9 studies met the eligibility criteria and were included for quality analysis. Figure 1 shows the PRISMA flow diagram of study selection.
Fig. 1
PRISMA search flow diagram
Characteristics of the included studiesThe included 9 studies were conducted between 2015 and 2022, while 3 studies [6, 43, 44] published in 2021 and 2022 updated the topic of this section and were not included in the previous review. Studies were conducted in China [43,44,45,46], Korea [6, 47], Spain [22, 48], and Britain [49]. Although the included studies varied by location, the synthesis of evidence can provide guidance and help for practice and further research. The main characteristics of the included studies are summarized in Table 2.
Table 2 Characteristics of the included 9 studiesParticipantsThe 9 studies enrolled 526 participants, with the number of participants varying from 40 [47] to 109 [48]. The mean age of the participants was 61.6 years. Participants included in all studies contained both genders, but there was an overall predominance of male participants. All participants in this study had less than three months of stroke onset. Three studies [6, 45, 49] included patients within 2 weeks of stroke. Two studies [22, 46] included patients within 1 to 3 weeks of stroke. One study [48] included patients within 3 weeks of stroke. Others [43, 44, 47] included patients within 3 months of stroke. Most included studies did not assess the initial MIP and MEP, while only 3 studies [22, 48, 49] evaluated the initial MIP and MEP. The average of the initial MIP and MEP was 40 cmH2O and 60 cmH2O respectively. Research shows that the normal values of MIP and MEP are as follows: MIP (118.4 ± 37.2 cmH2O for men, 84.5 ± 30.3 cmH2O for women), MEP (140 ± 30cmH2O for men, 95 ± 20 cmH2O for women), while lower than normal values are considered a decrease in MIP and MEP [50, 51]. The original average MIP and MEP in the included studies are both considered decreases.
InterventionsAll included studies performed RMT in the intervention group (IG). Six studies performed IMT and EMT [6, 22, 43, 44, 47, 48], while the remaining studies only had IMT [45, 46, 49]. Both IG and the Control Group (CG) carried out regular rehabilitation therapy. Six studies [6, 43,44,45,46,47] used regular rehabilitation programs in the CG. Three studies [22, 48, 49] used sham MIP + MEP with the workloads fixed in the CG, which was not enough to improve respiratory muscle strength or endurance. Regarding the devices used in the IG, they were different: Threshold, Orygen-Dual valve, Respironics, A flow-oriented incentive spirometer, Acapella vibratory, SECCO S2 intelligent respiratory training instrument, POWERbreathe, all from the manufacturer (Details in Table 2). Although different types of devices were used, most of the studies were threshold resistance, while only Gu et al. [45] and Choi et al. [6] were variable resistance.
The parameters of intervention were different across the studies. Although the intensity of RMT in the included studies varied, they started at 30% to 50% of MIP/MEP and were adjusted with the intervention weekly or biweekly. RMT with an intensity of less than 30% may not improve inspiratory muscle strength and exercise tolerance [27]. Additionally, the frequency and duration also varied in these studies. The time of the sessions varied from 20 to 30 min. Five studies [6, 43, 44, 46, 47] tended to adopt 30 min, and the remaining studies [22, 45, 48, 49] used 5 sets or 5–10 sets with 3 or 10 repetitions. Furthermore, sessions were carried out 5 to 14 times per week. The duration of the intervention ranged between 3 to 8 weeks.
Methodological quality and risk of bias of included studiesThe methodological quality and risk of bias of included studies were critically evaluated using the PEDro scale and the Cochrane Risk of Bias tool. Table 3 presents each item score and the results of 9 RCT studies. The risk of bias graph is shown in Fig. 2. The studies of Messaggi-Sartor et al. [48] and Yu et al. [46] were the highest scores with a PEDro score of eight points, and their methodological quality can be regarded as 'good'. Furthermore, there were also 6 studies [6, 22, 43,44,45, 49] whose methodological quality can be regarded as 'good'. Though the lowest score was five points for the study of Yoo and Pyun [47], its methodological quality can be regarded as ‘fair’. The mean PEDro score of the included studies was 6.5 (range 5 to 8). Therefore, it is considered good-quality evidence.
Table 3 Study quality on the PEDro Scale of 9 studiesFig. 2
Risk of bias graph the included 9 studies
All the critically appraised studies reported random allocation, baseline similarity, between-group differences, and point estimate and variability. Eight studies [6, 22, 43,44,45,46, 48, 49] provided intention-to-treat analysis. Five studies reported respectively appropriate follow-up data [43,44,45,46,47] and reported concealed allocation [6, 44, 46, 48, 49]. Four studies [22, 46, 48, 49] provided blindness to outcome assessors, which may introduce detection bias. However, only one studies [48] showed blind participants. None of the studies blinded the therapists. Participants and therapists were not blinded, which could lead to performance bias. However, performance bias should not be considered a preferential bias effect because it is difficult or impossible to blind participants and therapists in the process of implementing complex interventions [52]. Therefore, despite the performance bias and detection bias in these studies, the lack of blinding for participants and therapists was accepted in this review but taken into account when interpreting the results.
Effect of interventionsEffect of respiratory muscle training on respiratory muscle strengthThe MIP and MEP were assessed in six studies [6, 22, 45, 46, 48, 49]. RMT produced a statistically significant effect on improving MIP (n = 309, MD = 10.93, 95%CI: 8.51-13.36, p < 0.00001, I2 = 0%) (Fig. 3) and MEP (n = 309, MD = 9.01, 95%CI: 5.34–12.69, p < 0.00001, I2=37%) (Fig. 4) in patients with early stroke compared to the CG. Sensitivity exclusion analysis showed that no study significantly affected the pooled results of MIP and MEP after excluding the study one by one.
Fig. 3
The pooled effect size of respiratory muscle training (RMT) on Maximal Inspiratory Pressure (MIP) between RMT and control groups. IMT = inspiratory muscle training; EMT = expiratory muscle training
Fig. 4
The pooled effect size of respiratory muscle training (RMT) on Maximal Expiratory Pressure (MEP) between RMT and control groups. IMT = inspiratory muscle training; EMT = expiratory muscle training
Three studies [6, 22, 48] performed IMT + EMT, while three studies [45, 46, 49] only carried out IMT. The subgroup analysis showed a statistically improvement in MIP for IMT + EMT (n = 162, MD = 9.78, 95%CI: 5.96-13.60, p <0.00001, I2 = 1%) and IMT (n = 147, MD = 11.60, 95%CI: 8.15–15.05, p<0.00001, I2 = 11%) (Fig. 3). Similarly, the subgroup analysis also displayed a statistically increase in MEP for IMT + EMT (n = 162, MD = 11.61, 95%CI: 3.80–19.43, p = 0.004, I2 = 66%) and IMT (n = 147, MD = 7.06, 95%CI: 3.50–10.62, p = 0.0001, I2 = 0%) (Fig. 4). Sensitive exclusion analysis suggested that no study significantly affected the pooled results of MIP for IMT+EMT and IMT. However, the pooled result of MEP for IMT + EMT wasnot statistically significant through excluding the study of Messaggi-Sartor et al [48]. There was no statistically significant difference between IMT + EMT and IMT in improving MIP (p = 0.49) (Fig. 3) and MEP (p = 0.30) (Fig. 4).
Effect of respiratory muscle training on pulmonary functionSix studies [6, 43,44,45,46,47] measured the results about pulmonary function. These studies all analyzed FVC and PEF. Five studies reported FEV1 except for the study of Gu et al [45]. The pooled data suggested that RMT pr
留言 (0)