
記住我



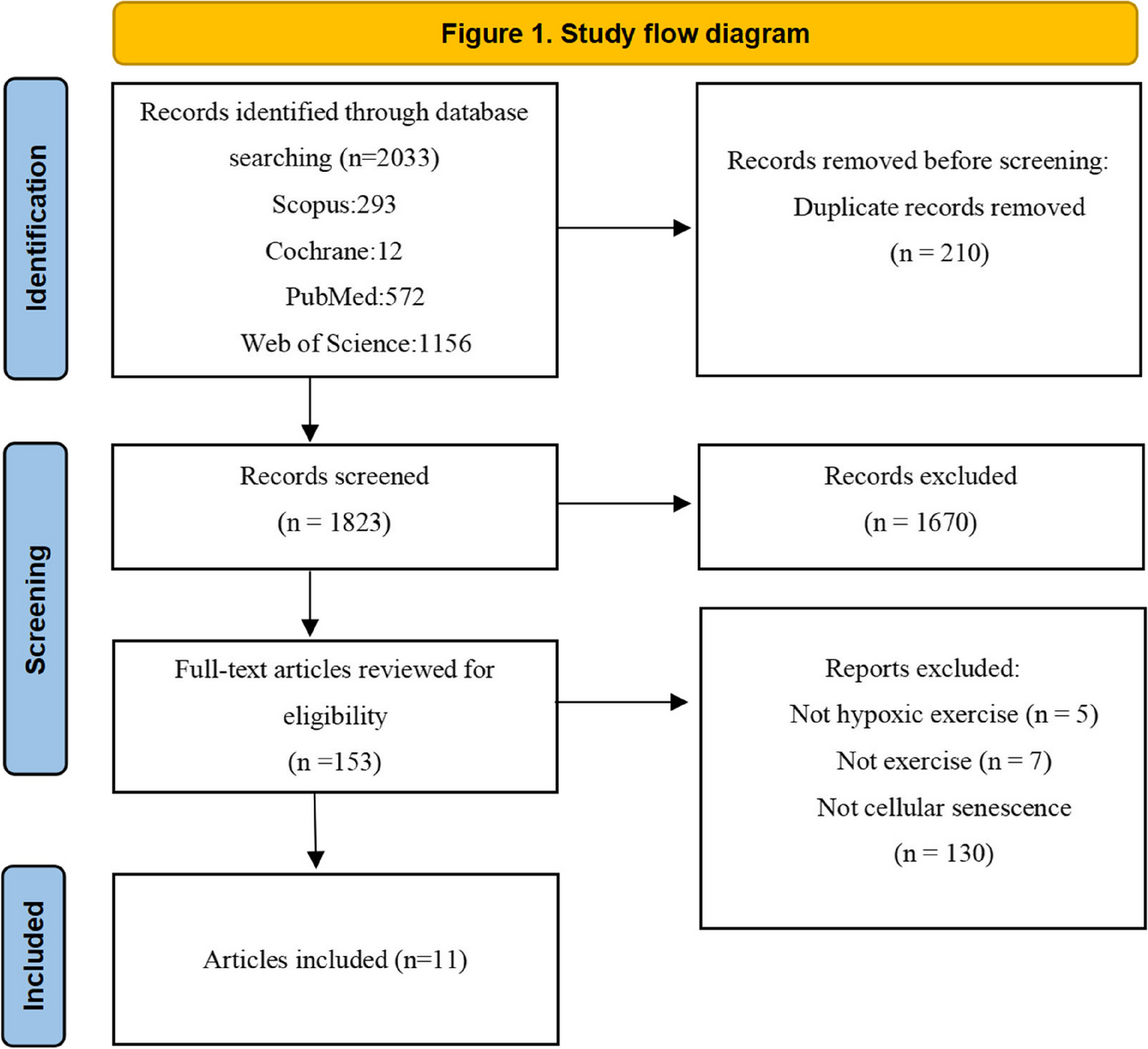
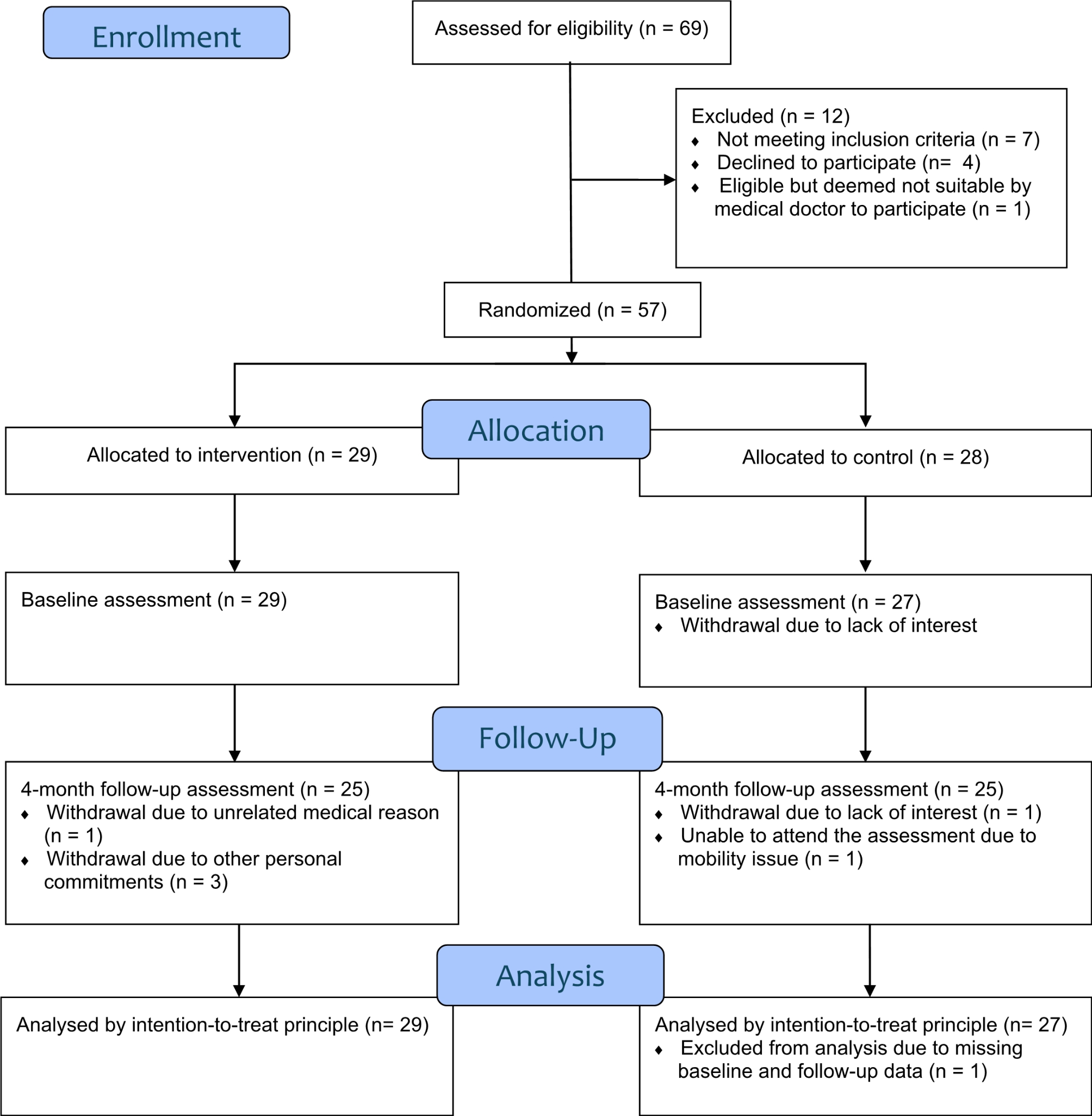




After an online advertisement, seventy-three older adults volunteered to participate in this single-blind randomized controlled study. At the time of recruitment, the subjects were included whether they were between 65–85 years old and autonomous in activities of daily living. Moreover, the following exclusion criteria were considered: (i) non-corrected sight disorders, (ii) neurological disorders, (iii) regular assumption of drugs that can interfere with normal cognitive functioning (e.g., antidepressants, antipsychotics, anxiolytics, assumption of psychotropic drugs), and (iv) other pathologies that contraindicate physical activity practice. Before enrolment, all the subjects were screened through a telephone interview according to inclusion and exclusion criteria. Eleven out of seventy-three were not eligible for the study. Thus, sixty-two older adults were enrolled in the study. For further inclusion in data analysis, subjects had to complete at least 21 out of 24 training sessions. Finally, fifty-seven subjects completed the whole experiment (Fig. 1). Three subjects discontinued participation in the study for medical disorders unrelated to the intervention; one did not complete the testing sessions, and one withdrew for personal reasons.
Fig. 1
Flow diagram of the study participants
Study designThe experimental protocol received approval by the ethical committee and adhered to the principles of the Declaration of Helsinki. All the subjects, after being informed about the methods of the study, gave their written informed consent and were free to renounce the study at any stage. A researcher not involved in the study and unaware of the aims randomly assigned subjects to two intervention groups (i.e., involved in the exercise program) and a control group (CTRL) with no exercise intervention. A block randomization was used for subjects’ allocation.
The stable (ST) group performed the training program over stable surfaces while the unstable (UNST) group over unstable surfaces. Furthermore, subjects were blinded to the differences between the two training programs.
In this single-blinded randomized controlled study, both intervention groups received 24 training sessions of 45 min each, twice a week for 12 weeks. The program was administered in the same gym for the ST and UNST groups. The three groups were tested at the baseline (T0), after six weeks (T1), and after twelve weeks (T2). Subjects participated in an evaluation session consisting of functional, dynamic balance, and isometric strength assessments. The experimental design is sketched in Fig. 2.
Fig. 2
Overview of the experimental design. T0, T1 and T2 represent the time points of the assessments within the 12-week interventions
Training programThe training intervention was exclusively administered to ST and UNST groups, while CTRL did not receive any intervention. The training sessions were scheduled on two non-consecutive days within the same week. Subjects were randomly assigned to one out of four sports scientists involved in the study, who trained the subjects for the whole training program. Moreover, within training sessions, each sports scientist trained a maximum of two subjects. Each training session started with a 10-min warm-up, including joint mobility exercises of the lower and upper limbs (e.g., twisting/tilting of the trunk), walking gaits (e.g., on toes, on heels, heel-toe walking), and preliminary strength exercises (e.g., throwing, lifting, or moving lightweights). At the end of each session, a 5-min cool down was performed with stretching exercises. Warm-up and cool-down were standardized for both intervention groups. The 30-min central part of the training was differentiated between the ST (Table 1) and UNST (Table 2) groups, and the exercises were divided into two sessions within the same week. In detail, on the first day (training A for ST group and training C for UNST group) of the week, the following exercises were performed: hip abduction, hip flexion, balance exercise, crunch, and squat. Then, on the second day (training B for ST group and training D for UNST group) of the week, leg press, hip adduction, hip extension, calf, and supine bridge were performed. Both ST and UNST groups exercised the lower limb muscles (i.e., hip, knee, and ankle muscle groups) using mainly resistance from a Leg press machine (Technogym, Cesena, Italy), Thera Bands® (Akron, OH, United States) with different stiffness, and ankle braces (XMB002, Chinesport, Udine, Italy) with different loads. The UNST group exercised using different unstable grounds that were introduced as unpredictable disturbances: foam pad (Airex®, Sins, Switzerland), gymnastic balls (Ledragomma Srl, Osoppo, Italy) of different sizes, and balance discs (Ledragomma Srl, Osoppo, Italy). All the subjects exercised with the intensity gradually progressing over the 12 weeks using training levels of increasing difficulty (Tables 1 and 2). Subjects were asked to perform three sets of 10 to 15 repetitions for each exercise at a self-determined “moderate” intensity (i.e., 12/14 out of 20) according to the Borg Scale [3]. Subjects were questioned every session, and the trigger for progression was a perceived exertion of 8/10 out of 20 (i.e., “somewhat light”). Hence, except for balance exercises with a fixed progression, the sports scientist gradually adjusted intensity as subjects’ abilities changed throughout the program.
Table 1 Training exercises and volume of the group training over stable surfaces (ST)Table 2 Training exercises and volume of the group training over unstable surfaces (UNST)MeasurementsGlobal Physical Activity Questionnaire (GPAQ-2)At the beginning of the study (T0), the GPAQ-2 was administered to estimate the daily physical activity level [20]. With 16 items, GPAQ-2 covers several physical activity components: intensity, duration, and frequency. It assesses the three domains in which physical activity is performed: (i) occupational physical activity, (ii) transport-related physical activity, and (iii) physical activity during discretionary or leisure time. The sum of the total Metabolic Equivalent (MET) minutes/week of activity was computed for a typical week in each domain.
Dynamic postural balance assessmentDynamic balance control was assessed with an innovative, electrically driven movable platform (EnginLAB s.r.l., Padova, Italy) already presented elsewhere [18]. The movable platform, controlled via software (RTC-9000, EnginLAB s.r.l., Padova, Italy), allowed programming an unexpected perturbation of the base of support, acting on the displacement and the ramp rate of the platform. For the present study, the displacement was set to 50 mm, and the ramp rate was 100 mm/s. The direction of the motion was forward with respect to the standing position of the subject. A force platform (AMTI BP400600, Watertown, MA, USA) was screwed over the movable plate to calculate the Center of Pressure (CoP) trajectory during the perturbations. The CoP displacement, derived from force platforms, is considered the most reliable output for postural balance control assessment [21, 22]. The software Balance Clinic 1.4.2 allowed real-time visualization of the CoP trajectory. The sampling frequency of the force platform was set to 200 Hz. An external trigger synchronized the force platform and the movable platform. Each trial lasted 60 s, and between the twentieth and the fortieth-second, the operator randomly administered the unexpected perturbation. Out of the five trials, two no-perturbation trials were randomly administered to prevent the subject from thinking that the perturbation would have always occurred. All subjects wore a safety harness attached to an overhead frame to prevent falling in case of loss of balance due to unexpected plate shifting [18]. The safety system did not affect the posture of the subjects and let them move without any constraints in response to the sudden perturbation. For each trial, subjects were asked to stand over the movable system with arms along their sides and knees extended, gazing at a reference in front of them at 0.80 m. The feet position was recorded at T0 to replicate the same position over the force platform in the following testing sessions (i.e., T1, T2).
Upper and lower limb strength assessmentAt the beginning of the study (T0), the grip strength of the dominant hand was measured using a handgrip dynamometer (Jamar, JLW Instruments, Chicago, IL, USA) [23]. Three consecutive measurements were made with subjects seated upright and elbow flexed at 90°. The dominant lower limb strength was evaluated in the three testing sessions through an isometric maximal voluntary contraction (MVC) of the quadriceps [24, 25]. The experimental setup consisted of a custom-built chair instrumented with a uni-axial load cell (MuscleLab, Ergotest Innovation, Stathelle, Norway) positioned three centimeters above the malleolus. The subjects performed the MVC seated with the knee flexed at 90 degrees and secured to the chair with straps to minimize additional body movements. Subjects were asked to keep their hands crossed over the chest for the whole test duration. Before the test, ten submaximal contractions were performed as a warm-up. Then, three maximal trials with real-time feedback of the actual force were performed with 40 s of recovery in between. Each MVC lasted 3 s, during which the operator verbally prompted the subject to achieve the maximal effort.
Walking testsIn the Timed Up and Go (TUG) test, subjects were required to stand up from the chair, walk at the preferred pace to a cone at 3 m, turn around, and walk back to the chair to sit down [26]. The timing started at the word “Go” by the operator and stopped after the subject sat on the chair. In the 10-m walking test, subjects were instructed to walk 20 m at their preferred speed. The timing started when the subjects passed the 5-m line and stopped when they crossed the 15-m line away on the floor from the starting position. In both walking tests, three trials were performed with 30 s of recovery.
Data analysisIn the present study, the calculation of CoP parameters in the dynamic balance tests followed the procedure already presented elsewhere [18]. The perturbation point (PP) was identified as the instant the movable platform moved. The Unit Path (the mean velocity measured in cm∙s−1) and Area95 (the area of the 95th percentile confidence ellipse measured in cm2) were calculated over a 2.5-s time window after the PP. Moreover, we calculated three additional parameters (Fig. 3) to deepen the postural responses in the direction of the perturbation (i.e., posterior-anterior). The first peak (FP) represents the difference between the maximal peak reached by the anterior–posterior CoP trajectory after the PP and its mean value before the PP. The maximal oscillation (ΔCoPMax) was calculated as the sum of the absolute values of FP and the subsequent peak. The post-perturbation variability (PPV) was defined as the standard deviation (SD) of the anterior–posterior CoP trajectory over the 2.5-s time window after the PP, and it is an index of the efficiency of the subject in reducing the body oscillations immediately after the external perturbation to reach a new quiet condition [18].
Fig. 3
Graphical representation of the center-of-pressure (CoP) parameters referred to the dynamic balance assessment over the electrically-driven mobile platform. A CoP trajectory (black line) and 95th percentile ellipse (blue line) within the 2.5-s time window from the beginning of the perturbation. B CoP-related parameters referred to the anterior–posterior CoP trajectory (black line) following the electrically-driven mobile platform displacement (red line). The gray dotted line marks the perturbation point (PP); the green dotted line represents the mean value of the anterior–posterior CoP trajectory before the perturbation occurs
The handgrip test measured the isometric grip strength of the dominant hand in kilograms. On the other hand, the maximum strength of the dominant lower limb was expressed in Newton and normalized with respect to the subject’s body mass (% BM).
Statistical analysisThe a-priori power analysis calculation (G * Power 3.1.9.2 software) showed that a total sample size of 51 participants and a medium effect size (f) of 0.25 would have provided a statistical power of 0.8 with an α error probability of 0.01. The enrolment of sixty-two adults allowed the required sample size to be achieved despite five dropouts. The dropout subjects were excluded from the study and thus, were not considered in the statistical analysis. The mean value among the three trials was calculated in the dynamic balance and walking tests. Conversely, the highest value of the three trials was considered in the upper and lower limb strength. Data are presented as mean and standard error of the mean (SE). The Shapiro–Wilk test checked the normality distribution of data. The one-way analysis of variance (ANOVA) compared MET data, handgrip values, and groups’ characteristics at the baseline (T0). Then, a two-way mixed-model ANOVA for repeated measures investigated the main effects of training (i.e., T0, T1, and T2), groups (i.e., ST, UNST, and CTRL), or any interactions. In case of a statistically significant main effect or interaction, the Holm-Bonferroni post hoc test assessed the pairwise comparisons. The effect size (d) was calculated to assess the strength of potential changes following the exercise interventions (T0 vs. T2) for all variables. The magnitude of the effect size was interpreted as follows: partial eta-squared (ηp2): small ≥ 0.01, medium ≥ 0.06, and large ≥ 0.14 [27]; Cohen’s d: small (0.2 ≤ d < 0.5), medium (0.5 ≤ d < 0.8), and large (d ≥ 0.8) [28]. The significant level for differences was set to p < 0.01. JASP Software (University of Amsterdam, Amsterdam, The Netherlands), version 0.16.4.0, was used for statistical analysis.
留言 (0)