
記住我







From April 2011 to December 2014, 110 Simpliciti prosthesis were implanted in 105 patients. During follow-up, four patients died, three patients were lost to follow-up, four patients had to be excluded from this study because of neurological illness, and one patient did not want to participate. Due to the COVID-19 pandemic in 2020, not all patients could be examined clinically, but the SSV and QDASH scores were collected from four patients in telephone interviews.
In total, follow-up of 89.1% of patients was achieved. Data from 98 (98/110) Simpliciti shoulder prostheses in 93 patients (38 men, 55 women) were evaluated for this study. Specifically, 10 HSA and 88 TSA were analyzed. The mean age at surgery was 66.7 years (32–83 years). At follow-up the mean age was 72.7 years (36–90 years). A mean follow-up of 71.5 months (49–106 months) was achieved. Patients with primary omarthrosis, posttraumatic omarthrosis, primary humeral head necrosis, secondary humeral head necrosis after fracture, omarthrosis in glenoid defect, and omarthrosis in glenoid dysplasia were included in the analysis.
Clinical and ultrasound resultsClinical results were collected for 94 shoulders. A mean active flexion of 141.4° ± 26.9° was achieved in the entire study group (HSA 132.3° ± 26.5°, TSA 142.3° ± 26.9°). The mean active abduction was 124.5° ± 30.1° (HSA 122.8° ± 25.6°, TSA 124.7° ± 30.7°) and active external rotation was possible on average up to 47.2° ± 13.4° (HSA 37.7° ± 16.8°, TSA 48.3° ± 12.6°).
A sonographic examination of the shoulder was performed on 95 shoulders and was normal without pathological findings in 79 shoulders (83.2%). A ruptured biceps tenodesis was visualized in two cases (2.1%), a partial rupture of one tendon of the RC was seen in 13 cases (13.7%; four subscapularis, seven supraspinatus, two infraspinatus), and a complete rupture of an RC tendon was detected in three cases (3.2%; two subscapularis, one supraspinatus).
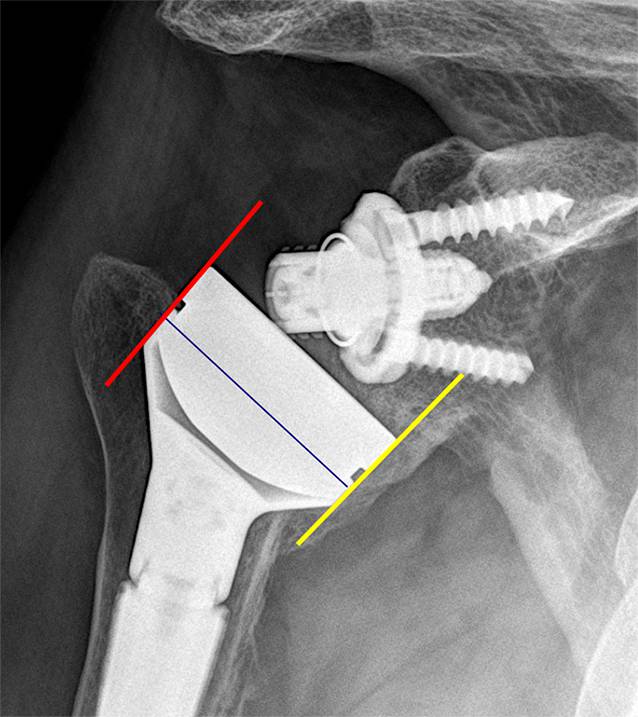
Radiographic outcomesRadiographs of 95 shoulders were evaluated in anteroposterior, axillary, and lateral views. Superior migration of the humerus, which was interpreted as a loss of the Gothic arch, was observed in 26 cases (27.4%).
None of the examined prostheses showed radiolucent lines around the nucleus or radiological signs of loosening. Bone resorption next to the nucleus occurred in 41 (41.8%) implanted prostheses. The outer edges (zones 1, 7, 8, and 14; Fig. 2) and the zones where the humeral head protrudes over the nucleus (zones S, I, D and V; Fig. 2) were mainly affected. Resorptions were found most frequently in zones S, I, D, and V (Fig. 3).
Fig. 3
Typical bone resorption (12 months postoperatively) in the outer zones where the humeral head protrudes beyond the nucleus and no force transmission to the bone can be achieved: a in anteroposterior view, zones S, I; b in axillary view, zones V, D. Circles: typical bone resorption, Arrow: edge of the collar of the prosthesis
Three patients who were initially treated with HSA showed slight central glenoid wear, but the humeral head was still well centered. As all patients showed good clinical results and subjective satisfaction, no surgical treatment was required.
The difference between pre- and postoperative COR and between pre- and postoperative ROC could only be determined if exact pre- and postoperative true anteroposterior image were available. This was the case in 61 shoulders. The postoperative COR deviated from the preoperative COR by 3.7 mm ± 1.9 mm (range: 0.3–8.2 mm). Overall, 39.3% of the measured shoulders showed a deviation of less than 3 mm. The direction of deviation was superior–medial (SM) in one case, superior–lateral (SL) in one case, inferior–medial (IM) in four cases, and inferior–lateral (IL) in 55 cases. The postoperative ROC was on average 3.2 mm ± 1.3 mm larger than the preoperative ROC.
No significant correlation between the deviation in COR and ROC nor clinical scores from the study collective could be demonstrated (p > 0.05).
ScoresThe SSV was collected from 98 shoulders and was 86.1% ± 16.0% in the entire collective (HSA 78.5% ± 17.7%, TSA 87.0% ± 15.3%), without significant differences between HSA and TSA (p = 0.112).
A valid QDASH score was obtained from 88 patients. The QDASH score averaged 11.7 ± 13.8 points in the entire collective (HSA 21.6 ± 15.6 points, TSA 10.4 ± 13.2 points). There was a significant difference in QDASH between the HAS and TSA groups (p = 0.015).
The CS was collected for 93 shoulders. The mean CS for the entire cohort was 75.4 ± 10.9 points (HSA 70.4 ± 10.4 points, TSA 76.0 ± 10.8 points), without a significant difference between the HSA and TSA groups (p = 0.221). Preoperative CS was available for 86 patients. A case-by-case comparison between preoperative and postoperative CS was carried out for 82 patients. In the entire study collective, the operation showed an average improvement of the CS of 43.8 ± 11.7 points from 32.2 ± 10.4 points preoperatively (p ≤ 0.05). In HSA, the CS increased by 42.1 ± 15.0 points from 28.3 ± 12.6 preoperatively (p ≤ 0.05), and in TSA, from 32.7 ± 10.1 by 44.1 ± 11.3 points (p ≤ 0.05).
The nCS was collected from 93 shoulders postoperatively. The overall nCS reached 89.7% ± 12.4% (HSA 82.1% ± 13.5%, TSA 90.7% ± 12.0%). A significant difference between HSA and TSA was determined (p = 0.039).
All collected scores are summarized in Table 1.
ComplicationsThere were no intraoperative complications. No postoperative infections were detected, and no neurological complications related to the operation were observed.
One patient sustained a traumatic undisplaced fracture of the tuberculum majus 18 months postoperatively, which could be treated conservatively. Three patients developed a secondary frozen shoulder, which was treated with arthroscopic 360° arthrolysis. All three patients were symptom-free after arthrolysis. In one patient, a periprosthetic subcapital fracture of the humerus caused by a fall was treated with an angle-stable plate osteosynthesis around the prosthesis ex domo. Two patients had radiological signs of glenoid loosening. In one of these cases revision to a reverse shoulder prosthesis (RSA) was performed. At revision the Simpliciti prosthesis was still well fixed.
One patient treated with HSA suffered from glenoid wear and hereby irritation with a metal suture anchor placed in the glenoid before the prosthetic implantation occurred and a revision to RSA was performed. Three weeks after the implantation of the prosthesis, one patient had a serious fall downstairs due to an epileptic seizure with tearing of the entire greater tuberosity. At revision the Simpliciti was stable despite only the inferior half of the nucleus being within the humeral bone. Both of these patients were excluded from the study because no data on the original Simpliciti could be collected.
The complication rate in the collective was 7.1% (7/98). The revision rate was 5.1% (5/98) including three arthroscopic releases, one osteosynthesis of a periprosthetic fracture, and one conversion to RSA. There was not a single case of revision due to loosening of the Simpliciti prosthesis.
留言 (0)