
記住我









Data were collected as part of the Ontario COVID-19 and Kids Mental Health longitudinal study, a research collaborative of four established research cohorts with pre-existing participant bases: two clinically-referred pathways (i.e., MH, neurodevelopmental disorders diagnoses [NDD]) and two community-referred pathways. Clinical cohorts consisted of children who had been referred to an outpatient psychiatry clinic at a tertiary children’s hospital in Toronto, and/or participants of the Province of Ontario Neurodevelopmental Disorder network, for children with NDDs. The community cohort consisted of children and families recruited through an urban science museum. Detailed descriptions of the cohorts, consent, and participation processes of the larger project are provided elsewhere [12]. The present study included a subset of children ages 6 to 12 years to align with those of the matched resources or interventions. All participants provided informed written consent/assent to participate in the current study. The study was approved by the institutional research ethics boards at all participating institutions.
Study processThis study occurred in two phases [1]: profile generation and [2] electronic matching.
Phase 1: profile generationMH data were collected between February and August 2021, using the standardized measures below. When multiple assessments for an individual child were available, the most recent data were used to generate MH profiles. Using latent profile analysis (LPA) across the larger Ontario COVID-19 and Kids Mental Health longitudinal project (n = 1,608), five child MH profiles were indicated based on depression, anxiety, hyperactivity, inattention, and irritability scores (Table 1, Supplementary Table 1, Supplementary Fig. 1). Profiles were generated prior to the first study timepoint (Time 1).
Table 1 Child mental health profiles and matched mental health online resourcesPhase 2: electronic match processThree hundred families from the larger Ontario COVID-19 and Kids Mental Health longitudinal project were randomly selected to participate in the present study, and 292 families consented. Online surveys were distributed to parents at three time points (Fig. 1), using REDCAP electronic data capture tools [13, 14].
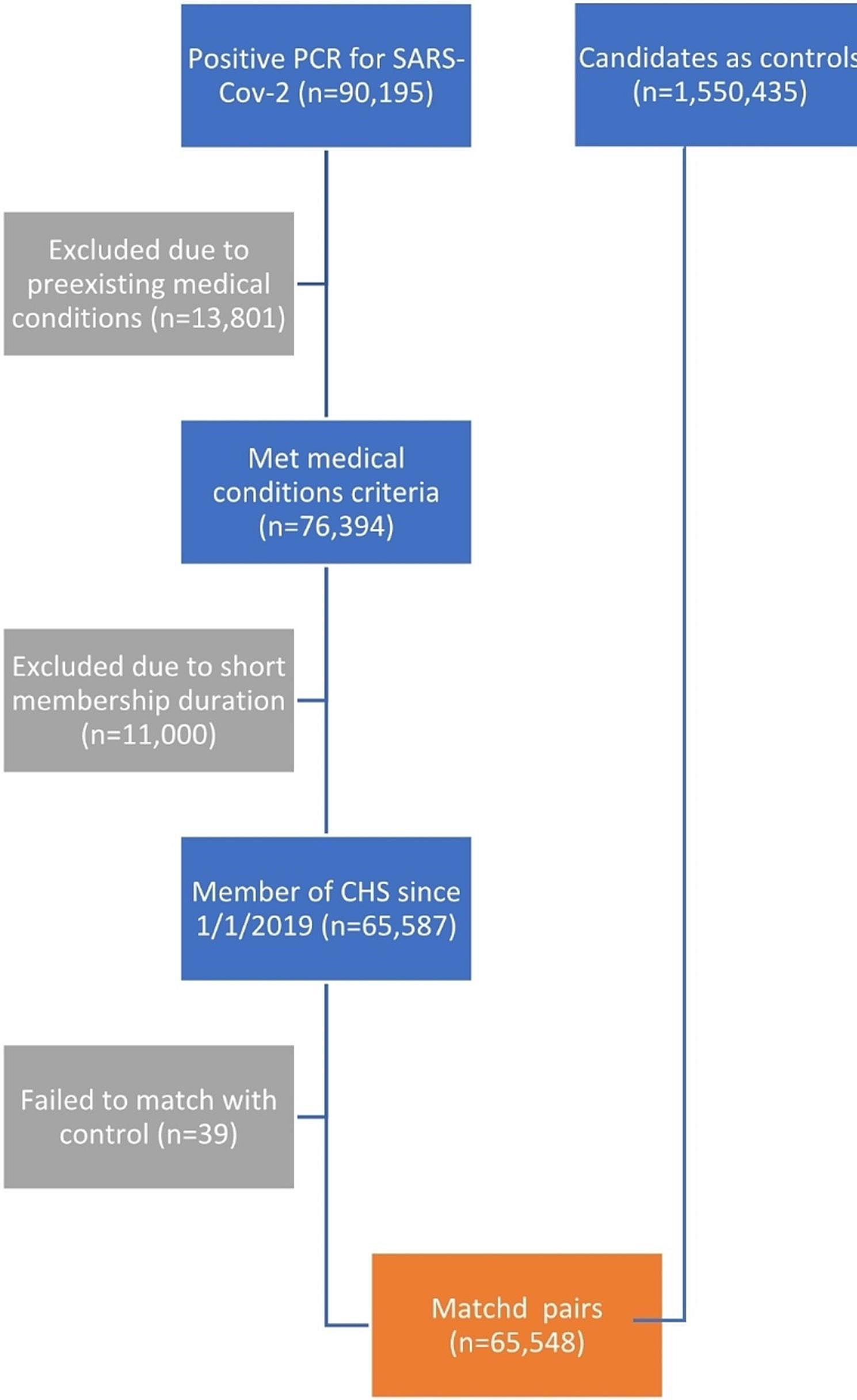
Fig. 1
Overview of the electronic match process
At Time 1, parents were provided with a brief explanation of how their child’s profile was created and that a virtual MH resource would be offered based on this profile. Parents completed the Time 1 survey, regarding their perception of the feasibility of an electronic matching process, prior to receiving the virtual MH resource.
Following completion of the Time 1 survey, parents received their child’s matched virtual MH resource with a brief description of the resource. The resources provided for each MH profile are described in Table 1. Following receipt of the matched resource and description (Time 2), parents completed a second survey about their perceptions of the electronic match and the matched virtual MH resource (i.e., satisfaction with the electronic match process, perceived reasonability and satisfaction with the matched virtual MH resource). Following the Time 2 survey, parents were provided with access to either the resource package (Average and Low Symptoms profiles), or with the contact information for enrollment in the matched resource (Internalizing, Externalizing, and High Symptom profiles).
One month after completion of Time 2, a further study follow-up (Time 3) was conducted to measure uptake of the matched resource.
MeasuresDemographic measuresChild age, sex at birth, ethnicity, pre-existing MH/NDD diagnosis, and family annual household income were collected.
Child MH measuresDepression was measured with the Major Depressive Disorder subscale of the Revised Child Anxiety and Depression Scales-Parent Version (RCADS-P) and t-scores were computed [15]. Anxiety was measured with the 9-item Generalized Anxiety Disorder subscale (GAD-9) of the Screen for Child Anxiety Related Disorders (SCARED) instrument [16, 17]. Hyperactivity and inattention were measured with the respective subscales of the Strengths and Weaknesses of Attention-Deficit/Hyperactivity Disorder Symptoms and Normal Behavior Scale (SWAN) [18]. Irritability was measured with the 6-item subscale from The Irritability and Dysregulation of Emotions Questionnaire (TIDES) [19].
Parent MH measuresParents’ self-reported depression and anxiety symptoms were assessed with the 8-item version of the Patient Health Questionnaire (PHQ-8) and the Generalized Anxiety Disorder-7 (GAD-7) measure, respectively [20, 21].
Feasibility measuresThe four-item Acceptability of Intervention Measure (AIM) and the Intervention Appropriateness Measure (IAM) measures [22] were combined following principal components analysis to assess the perceived reasonability of the electronic match process and virtual MH resource. Mean composite scores were computed for all measures. Perceived satisfaction with the electronic match process was assessed using the 7-item Program Feedback Scale and the 8-item Client Satisfaction Questionnaire for Internet-based Interventions (CSQ-I) [23, 24]. The Readiness for Therapy Questionnaire (RTQ) was adapted to assess how ready parents were to undertake actions for their child’s intervention [25]. Further details about the reasonability, satisfaction, and readiness for therapy, including psychometrics in the current sample, are included in the Supplementary Methods.
Uptake of virtual MH ResourceParents were asked to report the extent to which they participated or intended to participate in the virtual MH resource matched to their child [1]: enrolled (completed resource, or signed up and completion of resource in progress) [2], waitlisted for resource [3] considering enrollment but not signed up and [4] will not enroll (no intention).
Data analysisPhase 1: child MH profilesLPA was used to identify child MH profiles across the larger Ontario COVID-19 and Kids Mental Health longitudinal project (n = 1,608). LPA is a data-driven technique that identifies latent subgroups within a sample, based on similar responses to a set of continuous variables. The LPA was conducted with MPlus using full information maximum likelihood estimator. Variances were constrained to be equal across profiles, and covariances between profiles were constrained to zero. LPAs computed posterior classification probabilities that indicated a child’s probability of being assigned to each profile with the aim of achieving a minimum probability of 0.80 [26]. Further details regarding profile assignment are provided in the Supplementary Methods.
Phase 2: completion at each time pointPotential factors that predict Time 1 completion were tested using logistic regression. These factors included child’s assigned profile as well as demographic variables: age, sex at birth, ethnicity, household income, and pre-existing MH/NDD diagnosis. There were four dummy-coded variables for profile, with the Average Symptoms profile serving as the reference group for all four dummy variables. Subsequent logistic regression examined whether demographics, perceived reasonability, or satisfaction at Time 1 predicted completion at Time 2. Further logistic regression examined whether demographics, perceived reasonability and satisfaction at Time 2, readiness for therapy at Time 2, or the matched virtual MH resource at Time 2 predicted uptake of the virtual MH resources at Time 3.
留言 (0)