
記住我

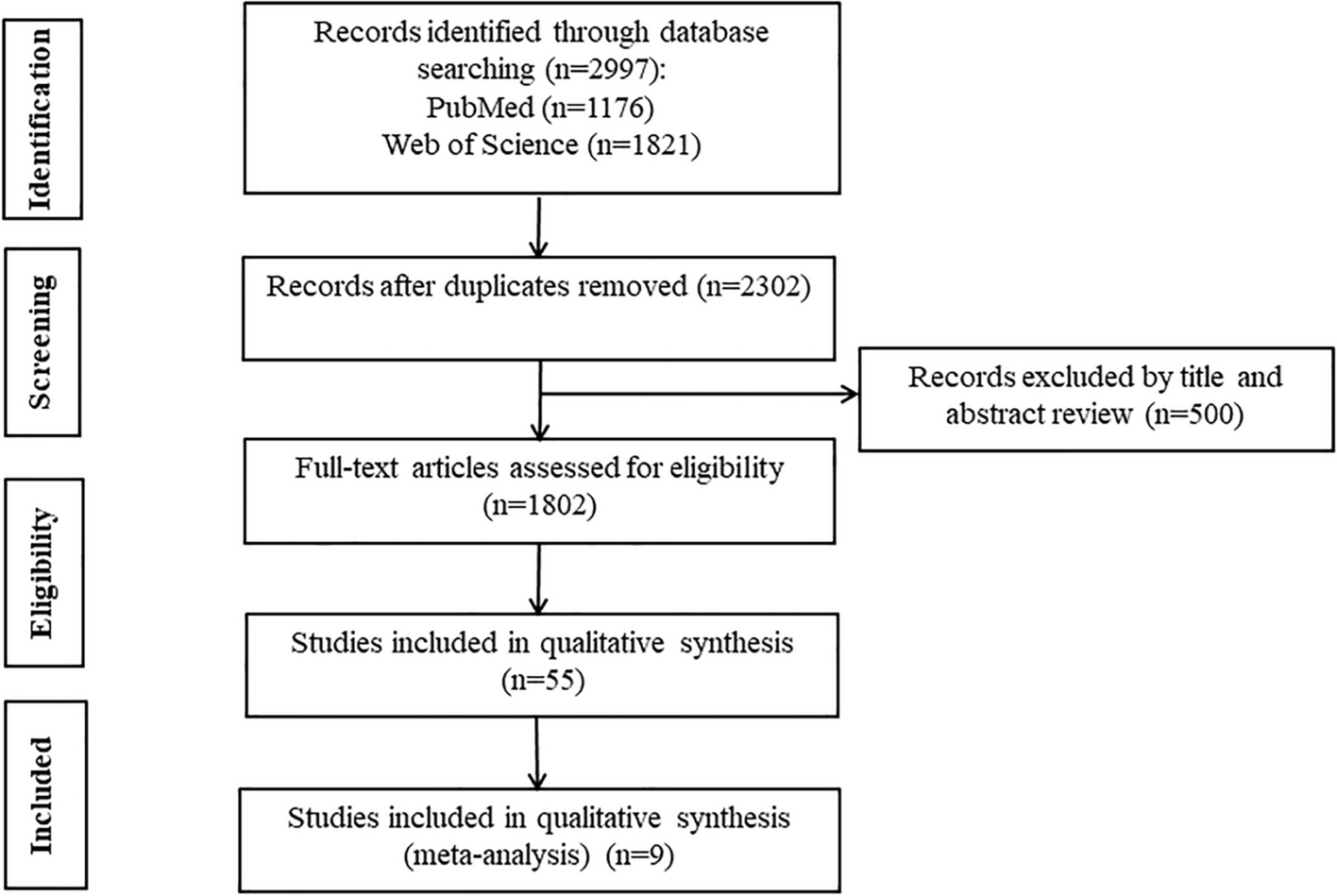






From September, 2020 to August, 2021, 44,738 patients were admitted to internal medicine department of Fuwai hospital (Fig. 1). Among them, 1638 patients were excluded due to no history of cardiovascular diseases, 2229 patients due to admission to the thrombosis department, 255 patients due to admission with VTE, 137 patients due to identification of VTE within 48 h after admission, 13,244 patients due to hospitalization less than 3 days. Finally, 27,235 patients were included. Among the cohort, 8450 individuals (31.03%) were female, with a median age of 60 (51, 67) years. Coronary heart disease (17,626, 64.72%) and hypertension (16,879, 61.98%) were the most commonly observed cardiovascular diseases, whereas heart failure (1337, 4.91%) and pulmonary hypertension (974, 3.58%) were the least common (Supplementary Table S2).
Fig. 1
Flow diagram of participant enrollment and exclusion. VTE, venous thromboembolism
During a median hospitalization of four days, 154 patients developed hospital-acquired VTE, whereas 27,081 patients did not. Among patients who developed hospital-acquired VTE, 92 patients (59.74%) had DVT, 32 patients (20.78%) had PE, and 30 patients (19.48%) had both PE and DVT.
Incidence and distribution of hospital-acquired VTEThe incidence of hospital-acquired VTE in the total cohort was 0.57%. Of note, the ICU had the highest incidence of hospital-acquired VTE (7.62%). On the contrary, department of coronary heart disease had the lowest incidence of VTE (0.09%) despite having the highest number of admitted patients.
Comparison of patients with and without hospital-acquired VTECompared to patients without hospital-acquired VTE, patients experiencing hospital-acquired VTE were significantly older (67.17 ± 13.71 years vs. 58.41 ± 13.21 years, P < 0.001), had worse New York Heart Association function class (NYHA FC) (III/ IV 40.91% vs. 6.47%, P < 0.001) and higher D-dimer [1.95 (1.12, 3.56) ug/ml vs. 0.79 (0.61, 1.26) ug/ml, P < 0.001] (Table 1). Severe cardiac diseases were also more prevalent in patients with hospital-acquired VTE, including acute coronary syndrome, heart failure and cardiomyopathy. Besides, these patients also had more comorbidities, including respiratory failure, infection, renal insufficiency, pulmonary hypertension, obstructive sleep apnea and hepatic insufficiency.
Table 1 Demographics of patients with/ without hospital-acquired VTEThe duration of hospitalization was also significantly longer in patients who developed VTE [12 (8, 17) days vs. 4 (3, 6) days, P < 0.001], and the median time of identifying hospital-acquired VTE was the fifth day after admission. During the hospitalization, patients who developed VTE were more likely to undergo invasive procedures, including central venous catheterization (9.1% vs. 0.6%, P < 0.001), intra-aortic balloon pump (IABP) (6.5% vs. 0.3%, P < 0.001) and mechanical ventilation (7.8% vs. 2.6%, P < 0.001). Moreover, these patients had higher proportion of immobility (7.8% vs. 0.2%, P < 0.001). During the hospitalization period, patients who developed VTE were less likely to receive anticoagulants (70.1% vs. 82.6%, P < 0.001), antiplatelet agents (55.8% vs. 73.7%, P < 0.001) and statin (67.5% vs. 77.1%, P = 0.005).
Factors associated with hospital-acquired VTEUnivariable logistic regression identified that female, age, D-dimer, NYHA FC, prior VTE, infection, renal insufficiency, pulmonary hypertension, obstructive sleep apnea, valvular heart disease, chronic coronary syndrome, acute coronary syndrome, cardiomyopathy, respiratory failure, heart failure, hepatic insufficiency, immobility, atrial fibrillation, mechanical ventilation, central venous catheterization and IABP were associated with increased risk of developing hospital-acquired VTE, whereas administration of anticoagulants, antiplatelet and statin was associated with reduced risk of hospital-acquired VTE (Table 2). Multivariable logistic regression further identified that female sex, age, infection, pulmonary hypertension, obstructive sleep apnea, acute coronary syndrome, cardiomyopathy, heart failure, immobility, central venous catheter, IABP and anticoagulation were independently associated with hospital-acquired VTE (Table 3 and Supplementary Table S3). Nomogram was constructed based on multivariable logistic regression (Fig. 2). The higher the total points, the higher the risk of developing VTE. The predictive ability of novel Fuwai nomogram was high (concordance index 0.865), which was further confirmed by internal validation (bias adjusted concordance index 0.864) and calibration (Fig. 3).
Table 2 Univariable logistic analysis of risk for hospital-acquired VTETable 3 Multivariable logistic analysis of risk for hospital-acquired VTEFig. 2
Nomogram for predicting hospital-acquired VTE in patients with cardiovascular diseases. ACS, acute cardiovascular syndrome; CMP, cardiomyopathy; CVC, central venous catheterization; IABP, intra-aortic balloon pump; PH, pulmonary hypertension; VTE, venous thromboembolism. In order to calculate the probability of hospital-acquired VTE, draw a vertical line straight upward from the predictor to the points axis to obtain the value, then sum the points of each predictor, this sum on the total points axis of the nomogram corresponded with the probability of hospital-acquired VTE, which can be determined by drawing a vertical line downward. For example, for a 60-year old female patient who had received central venous catheterization and was immobile during hospitalization without other risk factors and did not receive anticoagulants, the total points (156) = female sex (12 points) + 60 years old (60 points) + immobility (64 points) + central venous catheterization (20 points), and the probability of VTE was about 15%
Fig. 3
Calibration curve of nomogram. Calibration curve indicated high accuracy of nomogram in predicting VTE
Comparison of VTE risk prediction modelsThe predictive ability of Padua model (AUC 0.786, 95% CI 0.748–0.824, sensitivity 62.34%, specificity 81.84%) (Fig. 4) was lower than that of nomogram (AUC 0.865, 95% CI 0.835–0.895, sensitivity 79.87%, specificity 80.34%) (Fig. 3). Compared with Padua model, the nomogram had significantly better discrimination ability (net reclassification index 0.052, 95% CI 0.012–0.091, P = 0.009; integrated discrimination index 0.020, 95% CI 0.001–0.039, P = 0.051). Decision Curve Analysis demonstrated that the nomogram had better performance of risk prediction than Padua score (Fig. 5).
Fig. 4
Receiver operator characteristic curve of Padua score and Fuwai nomogram. AUC, area under curve; 95% CI, 95% confidence interval
Fig. 5
Decision curve analysis of Padua score and Fuwai nomogram. In the context of decision curve analysis, the x-axis illustrates threshold values for risks of VTE, whereas the y-axis denotes the net benefit for different cutoffs of primary endpoint risk. The greater the deviation of prediction models from the grey line and the horizontal black line, the greater the corresponding net benefit. The Fuwai nomogram demonstrated the larger net benefit across the range of risk of hospital-acquired VTE compared with Padua score. As the guideline suggested, Padua score was categorized two categories. Low risk is defined as Padua score < 4 points, high risk is defined as Padua score ≥ 4 points, in line with 9th American College of Chest Physicians Evidence-Based Clinical Practice Guidelines [4]
留言 (0)