
記住我





A total of 10,579 physicians were invited to participate in the survey. Of those, 1242 physicians responded to the invitation. Of the physicians who responded, 272 were not eligible because they did not qualify, 4 did not provide informed consent, 24 were excluded because the predefined quota for their specialty had been met, and 329 did not complete the screening questions. The remaining 613 physicians completed the questionnaire (200 surveys from France, 103 from Germany, 100 from Poland, 110 from Spain, and 100 from the Netherlands) and are included in this analysis. The overall response rate was 5.8% (613/10,579), though participation was capped once the target sample size in each country was reached.
Of the 613 physicians who completed the survey, the distribution by medical specialty for all countries combined aligned with predefined minimum recruitment targets (general practice: 30%; gynecology: 19%; urology: 15%; oncology: 11%; and dermatology: 11%). There were also at least five endocrinologists and psychiatrists for each country. Characteristics of participating physicians are given in Table 1. Most physicians characterized their practice as either office based (46%) or a university/research-oriented/teaching hospital (33%). Most physicians in this study had been practicing for over 10 years (81%), and only 4% reported that they had been practicing for 5 years or less. Sixty-five percent of the physicians identified as male.
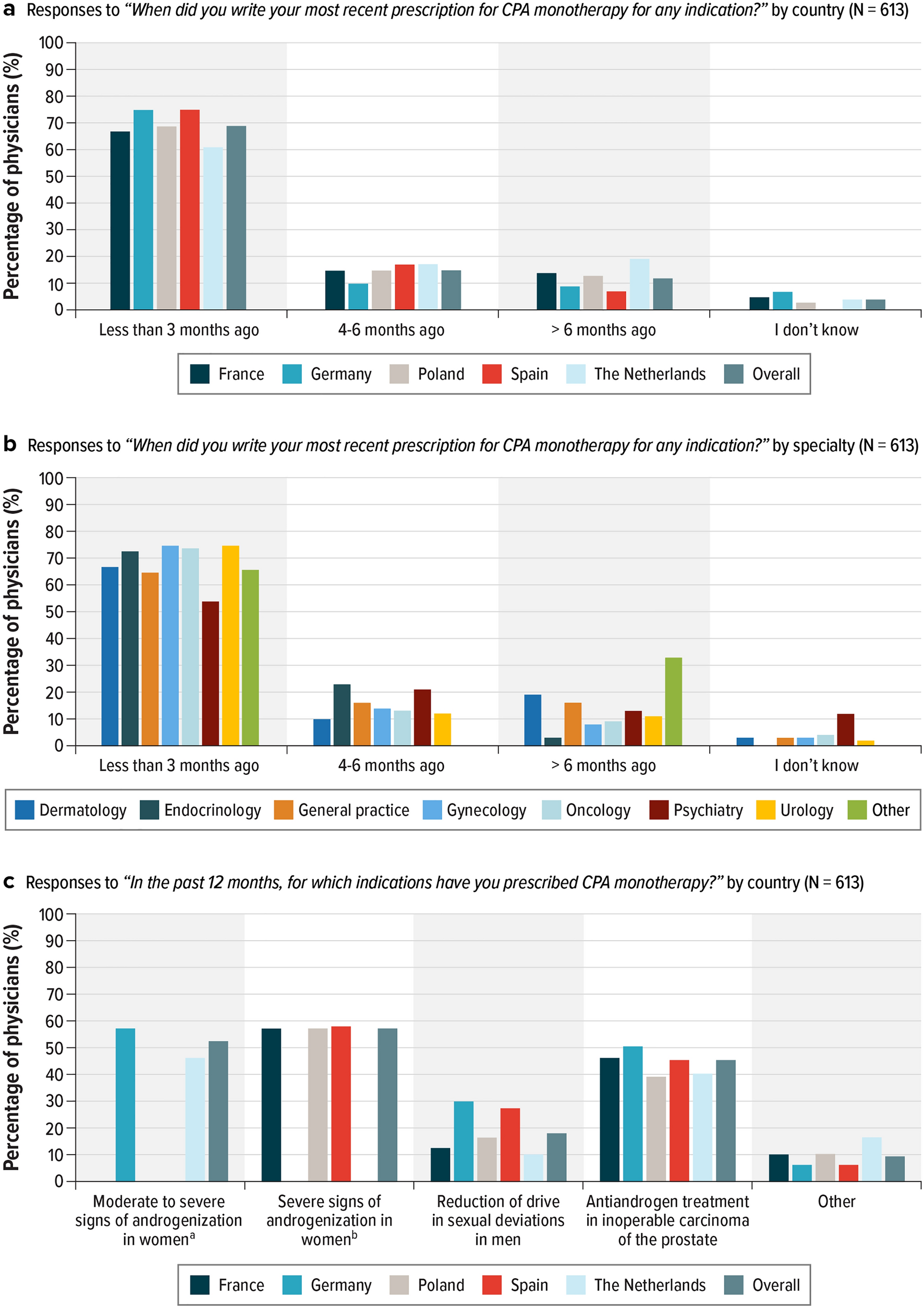
Table 1 Physician and practice characteristics3.2 Physicians’ Experience Prescribing CPA MonotherapyWhen asked when they had last prescribed CPA monotherapy for any indication, 69% of all physicians in the survey responded that they had written a prescription for CPA monotherapy within the previous 3 months, with 25% indicating they had prescribed it within the previous month. Results were broadly similar across individual countries; the percentage of prescriptions in the past month was lowest in the Netherlands (17%) and highest in Spain (36%) (Fig. 1A). Gynecologists (75%) and urologists (75%) were the specialties with the highest percentage of members who had written prescriptions within the previous 3 months, followed by oncologists (74%) and endocrinologists (73%); the lowest percentage was found among psychiatrists (54%) [Fig. 1B]. Physicians prescribed CPA monotherapy most commonly for androgenization in women (with a range from 46% in the Netherlands to 58% in Spain), followed by inoperable carcinoma of the prostate (ranging from 39% in Poland to 51% in Germany). These trends were consistent across the studied countries (Fig. 1C).
Fig. 1
Physician’s experience prescribing CPA monotherapy. A Responses to “When did you write your most recent prescription for CPA monotherapy for any indication?” by country (N = 613). B Responses to “When did you write your most recent prescription for CPA monotherapy for any indication?” by specialty (N = 613). C Responses to “In the past 12 months, for which indications have you prescribed CPA monotherapy?” by country (N = 613)
3.3 Knowledge of IndicationsPhysicians’ knowledge of indications for CPA monotherapy was dependent on specialty. Specialties most often reporting that they had prescribed CPA monotherapy either for “moderate to severe” or “severe signs of androgenization in women” (wording depended on the approved indication in each country) in the previous 12 months were as follows: gynecologists (95%), dermatologists (90%), endocrinologists (87%), and general practitioners (63%). Among this group, 88% of participants selected at least one correct response when asked when 10 mg or 50 mg doses of CPA monotherapy should be prescribed for moderate to severe signs of androgenization in women. More physicians chose “when no satisfactory results have been achieved with other treatment options” (73%) than “when no satisfactory results have been achieved at lower dose CPA-containing products” (40%), both of which were correct responses to this question. However, when asked to respond to “After using CPA monotherapy at a dose of 10 mg (in Germany and the Netherlands only, where this dosage is available as per country label) or 50 mg (in France, Poland, and Spain only, where this dosage is available as per country label) and achieving clinical improvement of moderate to severe signs of androgenization, the patient can continue using CPA monotherapy at this dose for as long as it is necessary,” only 34% of physicians correctly answered that this was a false statement, with a range from 15% in Germany to 50% in France. Gynecologists had the highest proportion of specialists correctly identifying this as false (41%); endocrinologists had the lowest proportion (27%).
Only 18% of physicians reported that they had prescribed CPA monotherapy for the reduction of sexual deviations in men, ranging from 10% in the Netherlands to 30% in Germany. Physicians who reported that in the previous 12 months they had prescribed CPA monotherapy for a reduction of sex drive in men with sexual deviations were asked when CPA monotherapy should be prescribed for this purpose in men, and 56% correctly answered that this should be done “when other interventions are considered inappropriate.” Psychiatrists (63%) and urologists (60%) had the highest percentage of correct responses to this question, as might be expected for the indication.
Forty-five percent of physicians had prescribed CPA monotherapy as antiandrogen treatment for inoperable carcinoma of the prostate in the past 12 months, with a range from approximately 39% in Poland to 51% in Germany. Seventy-five percent of these physicians correctly answered that “The use of CPA monotherapy for the treatment of inoperable prostate carcinoma and LHRH (luteinizing hormone-releasing hormone) flare remains unchanged per the summary of product characteristics (SmPC)” was true; the proportion of physicians answering this question correctly was highest among oncologists (78%), followed by urologists (74%) and general practitioners (71%).
3.4 Knowledge of Updated Safety Information for CPA MonotherapyAcross all countries, 43% of physicians correctly identified that a special warning and precaution about meningioma on the prescribing label for CPA monotherapy was updated in 2020. Those in France (63%) and Germany (50%) were most aware of this change (Fig. 2A). The proportion of physicians who reported they did not know what special warning and precaution was added ranged from 21% in France to 49% in Poland. Physicians specializing in gynecology (62%) and endocrinology (60%) had the highest awareness of the changes in the label regarding meningioma with use of CPA monotherapy; oncologists (30%) had the lowest awareness (Fig. 2B).
Fig. 2
Knowledge of CPA monotherapy warning label. Responses to “What special warning and precaution was recently added in 2020 to the prescribing label for CPA monotherapy?” (N = 613). A By country. B By specialty. *Correct response is marked with an asterisk
3.5 Knowledge of MeningiomaPhysicians were asked to identify clinical signs and symptoms of meningioma from a list of seven signs and symptoms, all of which were correct (Fig. 3). The list included the following, with the overall percentage of physicians selecting each in parentheses: headaches that worsen with time (92%), changes in vision (90%), seizures (84%), hearing loss or ringing in the ears (82%), loss of smell (81%), memory loss (73%), and weakness in extremities (72%). Overall, physicians’ knowledge of the clinical signs and symptoms of meningioma was high, with 98% of physicians correctly selecting at least one response and 66% of physicians correctly identifying all seven responses. Knowledge of the signs of meningioma was highest in Poland, where 100% of physicians selected at least one correct answer and 80% correctly identified all seven signs and symptoms (Fig. 3A). By physician specialty, dermatologists had the highest proportion who identified all seven signs and symptoms (78%), followed by psychiatrists (73%), oncologists (71%), general practitioners (67%), gynecologists (58%), and endocrinologists (50%) (Fig. 3B).
Fig. 3
Knowledge of the clinical signs and symptoms of meningioma. Responses to “Which of the following may be clinical signs and symptoms of meningioma?” (N = 613). A By country. B By specialty. *Correct response is marked with an asterisk
Most physicians were familiar with dose modulation guidelines to reduce the risk of meningioma with CPA monotherapy, and 74% correctly indicated that patients using CPA monotherapy should be monitored for meningioma. Approximately 85% of physicians correctly stated that CPA monotherapy should be prescribed at the lowest effective dose. Across all countries in the study, 75% of physicians correctly identified that the risk of meningioma increases with increasing cumulative doses of CPA monotherapy, and 73% correctly identified that if a patient treated with CPA monotherapy is diagnosed with meningioma, treatment with all CPA-containing products must be permanently stopped (Fig. 4A).
Fig. 4
Familiarity with risks from CPA monotherapy. Responses to “Please indicate whether each of the following statements about CPA monotherapy is true or false.” (N = 613). A By specialty. B By country. *Correct response is marked with an asterisk
As with knowledge of indications, there was some variability in the knowledge of meningioma related to CPA monotherapy across physician specialties. In most specialties, over 70% of physicians correctly answered that the risk of meningioma increases with increasing cumulative CPA doses and that if a patient receiving CPA treatment develops meningioma, CPA treatment must be permanently stopped. However, oncologists were an outlier: only 56% and 47% of oncologists, respectively, provided the correct answer to these questions. Across all physician specialties, oncologists had the lowest proportion of correct responses to questions regarding meningioma related to CPA monotherapy. Only 17% of oncologists correctly identified the statement “CPA monotherapy may be used in patients with a history of meningioma under carefully controlled conditions” as false. This question had a low correct response percentage overall, with only 39% of physicians indicating that CPA may not be used in patients with a history of meningiomas (Fig. 4B). Gynecologists had the highest correct response percentage (57%).
留言 (0)