
記住我



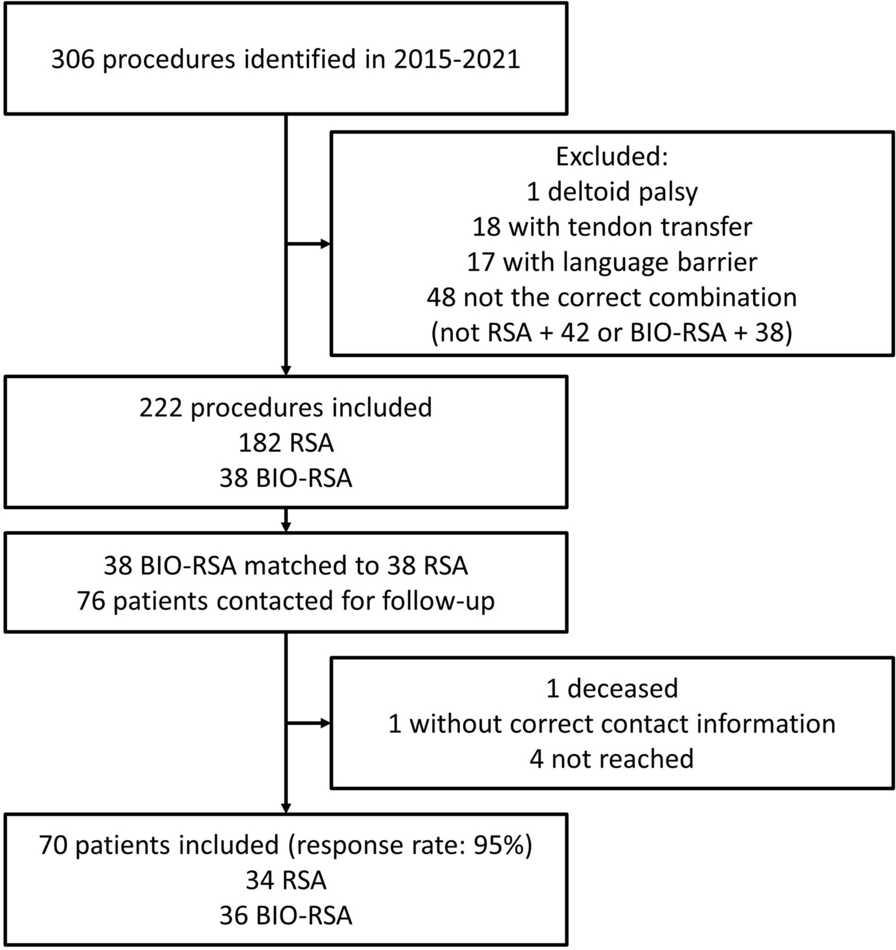





This was a retrospective observational cohort study. Patients were enrolled between July 2020 and July 2022 in an Italian outpatient clinic specializing in shoulder disease. All the manipulations were performed by the same therapist, an expert in joint manipulation.
The inclusion criteria were as follows. The patient was (1) aged < 55 years and (2) had a diagnosis of symptomatic phase III primary AC with a severe loss of shoulder ROM (severe ROM limitation was considered to be stiffness and limitations of passive shoulder lateral rotation, abduction, and internal rotation of more than 50% compared with the opposite side for at least 3 months). (3) Clinical and radiological data [magnetic resonance imaging (MRI) and X-rays] were collected that could be used to exclude patients with rotator-cuff lesions, glenohumeral osteoarthritis, and bone or cartilage lesions. (4) Patients affected by osteoporosis, as confirmed by their bone mineral density (BMD), were excluded from the study, while patients with osteopenia (i.e., with a T-score between − 1.0 and − 2.5) were included [13]. (5) Patients treated with steroid therapy for comorbidities and those who could not undergo local block anesthesia were excluded from this study. (6) There was 1 year of follow-up.
All the patients were enrolled through informed consensus and consented to the collection and processing of personal data.
Preliminary assessmentPatients underwent a general questionnaire in which we collected personal data and anamnestic information: their dominant limb, sports they used to play, comorbidities, a psychological assessment (depression, stress events, others), previous treatments, and time of pain onset.
Patients were further evaluated using the Numerical Pain Rating Scale (NPRS) and Simple Shoulder Test (SST).
The NPRS is a numerical scale from 0 to 10 in which 0 represents “no pain” and 10 represents “the worst pain ever.” The patient was asked to state the NPRS value for the pain suffered in four specific moments: during daily activities, at rest, during night-time, and after large and sudden movements [14].
The SST is scored on a multidimensional scale that corresponds to how the pain affects the loss of movement in and the strength and range of motion of the shoulder in daily life. The test is based on 12 items, each with a binary response, and the execution time is about 2 min [15].
The active ranges of motion of the affected limb and the opposite limb while standing were assessed by the physiotherapist with the goniometric technique in order to compare their progress. The participant was evaluated for shoulder elevation, abduction, external rotation with both the arm adducted and the arm abducted, and internal rotation.
To simplify the analysis, collected abduction and elevation ROM angles were categorized into numeric ranges (1: 0–30°; 2: 31–60°; 3: 61–90°; 4: 91–120°; 5: 121–150°; 6: 151–180°). Intrarotation levels were also collected and categorized into numeric ranges (1: thigh; 2: buttock; 3: lumbar-sacral joint; 4: L3; 5: T12; 6: T7).
Continuous data are shown as the mean and standard deviation. The t-test was used to compare NPRS scores, SST scores, and ROMs between the T0 and T1 evaluations. The selected threshold for statistical significance was p < 0.05.
The minimal clinically important difference (MCID) was calculated using the distribution-based method of a small effect size. All statistical analyses were performed using the SPSS version 24.0 statistical software (IBM Corp., Armonk, NY, USA).
ProcedureThe anesthetist performed ultrasound-guided interscalene brachial plexus block anesthesia in an outpatient clinic. After that, the shoulder was warmed up with a heating pad for 10 min in order to prepare the tissues for mobilization. All the procedures were performed by a single physical therapist. The operator performed an elongation of the retracted tissues through a specific progression of passive mobilizations in all three planes of movement of the glenohumeral joint, thus carrying out lysis of the capsular and extra-articular adhesions. Articular crepitus is produced by mobilization over the limits of the shrunken capsule, which is stretched and released. The manipulation consisted of glide and roll “swing” movements (the physiological movements of a healthy shoulder), avoiding translational movements, which can cause complications [16].
In the procedure used, the patient starts in the supine position on the table: the physiotherapist carries out a series of mobilizations up to an angle of 360° with a proximal solid grip. The proximal grip is used to prevent a long lever arm, which can produce shear forces on the bone, increasing the risk of fracture [17].
Similarly, in the first phase of the manipulation, rotational movements are avoided because the torsional forces generated can facilitate the onset of fracture in the presence of too many structured adhesions. Therefore, only single-plane movements are performed at the beginning. After the rupture of some adhesions, the joint backlash increases and the remaining capsular fibrosis breaks more easily: rotational movements are added from then on. The movements are performed in the following order:
1)Elevation to detach the posterior–inferior portion of the capsule (Fig. 1A).
2)Adduction in the horizontal plane to stretch the posterior portion of the capsule (Fig. 1B).
3)Extension (Fig. 1C) followed by internal rotation (Fig. 1D) to detach the posterior portion of the capsule. To perform these two movements, the patient is asked to position themselves sitting on the couch. This request is possible thanks to the type of anesthesia used and must be omitted in the case of mobilization performed under general anesthesia.
4)External rotation with the arm abducted to hold the anteroinferior portion of the capsule and extended to search for increased tissue tension (Fig. 1E).
5)External rotation with the arm adducted to hold the anterior–superior portion of the capsule (Fig. 1F).
6)Finally, the whole range of rotations is completed: external and internal.
Fig. 1
A–F Awake shoulder manipulation procedures performed by the physical therapist in order of timing
The described sequence also implies an anatomical rationale: the anterior capsule has almost double the thickness of the posterior one because of ligament thickening and thus shows higher resistance to traction. In order to reduce possible complications, we first stress the less resistant capsular portion, gaining the mobility of the posterior capsule, so that stronger manipulation to recover the stiffer anterior capsule is subsequently possible.
The treatment ends when the physiotherapist perceives that the end of the line is soft in all directions of movement; there is no mechanical stop sensation, unlike before the manipulation. The procedure is completed with a clinical assessment of bone stability: the absence of crackles, a preternatural range of motion, and glenohumeral joint dislocation.
Patients were not administered oral steroid drugs or other painkillers. After the treatment, patients were encouraged to use local cryotherapy to manage the pain and the bruising of the shoulder. Finally, patients underwent shoulder X-rays to assess possible bone lesions.
Complementary rehabilitation programOnce the joint mobilization was finished (after 10–20 min approximately), the patients were instructed and educated about the physiotherapy process that was necessary for the purpose of recovery. The rehabilitation program consisted of two aspects:
1)Passive mobilizations in all planes of movement, as performed by a physiotherapist three times per week for the first 4 weeks
2)Self-assisted treatment with active stretching exercises performed three times per day.
Every exercise was explained beforehand to each study participant.
The exercises were explained to the patients as follows:
Fig. 2
A–F Complementary home rehabilitation program assigned to all patients in the study
Assume a supine position with knees flexed and feet supported. With the help of a stick, and helping yourself with the healthy arm, elevate the affected arm as much as you can.
Variation: standing and facing a table, extend your arm by sliding your hand on the support surface (Fig. 2B).
Standing, face the wall or a door jamb with one leg front and one back. Place the hand of the affected arm on the wall and slide it gradually upwards.
Standing, with your side leaning onto the jamb of a door, place your arms along your side and bend your elbows at 90°. With the help of a stick, push the affected limb in external rotation without ever removing the elbow from your side.
Stand with your back towards the wall. With the hand of the affected arm, hook onto the edge of the wall or the door jamb and move laterally (to the right for the right arm and the left for the left arm). After reaching the maximum lateral displacement possible, you can increase the rotation by bending the knees and gliding with your back to the wall.
Variation: stand up; with the help of a towel, drag the affected arm up along the back (Fig. 2F).
Patients were interviewed at two different times during the study: the first was before the treatment (T0) and the second was 4 months after the treatment (T1). In both evaluations, the NPRS and SST were applied to the patients and the ROM was evaluated with a goniometric technique by the same therapist who performed the previous measurement. Moreover, during the latter evaluation, the patient was asked to communicate their level of satisfaction.
留言 (0)