
記住我



Boston Children's Hospital (BCH) Neonatal Intensive Care Unit (NICU) treats more than 650 patients annually and discharges about 200 infants directly home. It is one of only 2 Massachusetts NICUs designated as Level IV, treating the most difficult and medically complex infants. Many infants discharged home from the BCH NICU still have significant medical needs, including multiple medications, continuous cardiorespiratory monitoring, oxygen, feeding tubes, and other specialized equipment. Before these infants are discharged from the NICU, their parents must acquire new knowledge and skills necessary for providing basic newborn care and managing their complex medical needs. Parents receive comprehensive training on performing procedures such as managing tracheostomy tubes, ventilators, feeding tubes and pumps, administering intravenous parenteral nutrition, caring for central venous lines, administering medication(s), operating durable medical equipment (DME) and obtaining supplies, preparing special formulas, as well as navigating the healthcare system and serving as their child's advocates.
At discharge, infants and their parents have typically spent months in the NICU, surrounded by as much expertise as exists anywhere in the world. Despite extensive teaching, parents of medically complex infants have shared their experiences of encountering incredibly stressful situations in the home, ranging from difficult logistical issues to sudden life-threatening emergencies with the BCH NICU Family Advisory Committee members. In addition, results of a 2015-2016 Press Ganey survey commissioned by BCH revealed that parents gave high rankings in all areas related to the NICU stay, except for elements related to discharge preparedness. Only 71% of parents who completed the Press Ganey survey reported feeling sufficiently prepared to leave the hospital.1 This information confirmed that additional parental education and preparedness training was needed for parents to feel comfortable caring for their medically complex infants following discharge. Moreover, community visiting nurses and primary care providers (PCPs) who assume postdischarge care of these medically complex infants sometimes have limited experience with such patients. To bridge this education gap for parents and community-based providers, the NICU to Nursery (N2N) program, a standardized process for NICU discharge transition to home, was implemented.
AVAILABLE KNOWLEDGESeveral published scientific reports have documented education and preparedness issues and solutions related to parents caring for their medically complex infants after NICU discharge; thus, this problem is far from unique. Solutions proposed in the literature to address parental education and preparedness include (1) offering structured discharge teaching that begins shortly after admission, (2) using checklists and skills demonstrations for teaching, (3) carrying out systematic discharge readiness assessments to align educational needs with knowledge gaps, (4) encouraging parent self-assessments, and (5) teaching content that includes basic and specialty newborn care and home environment preparation.2–6 Smith et al3 recommends holding discharge planning meetings led by nurses to formalize the discharge preparation process. They explained that discharge planning meetings are necessary for parents to focus on discharge preparation, resulting in feeling more prepared. In a 2022 review of the literature, Griffith et al7 also endorsed the need for comprehensive, family-focused care plans for parents at discharge. Griffith states that NICU discharge planning and transition programs should outline specific goals for the infant and family to achieve, and that education be delivered face-to-face, using technology, or through home visits following discharge.7
In addition, research reveals PCPs and community visiting nurses are challenged when caring for medically complex infants who require polypharmacy, frequent care transitions, have multiorgan system disease, rare or unfamiliar diagnoses, and are technology dependent.8–10 Infants with medical complexity not only have multiple medical conditions but their conditions are also not always well understood. There are numerous published reports describing gaps in PCPs' knowledge when it comes to caring for infants with medical complexity.8,9,11 A common theme among PCPs is the need to develop care coordination skills and better communication between providers. Also, studies describe that community visiting nurses encounter similar challenges; parents report that these nurses are not always equipped to manage the needs of medically complex infants in the home.10,12
RATIONALEMost of the 650 NICU infants admitted to BCH annually are either transferred to an inpatient floor or discharged to other medical facilities to continue care as a bridge to eventual discharge home. However, about a third of these medically complex infants are discharged directly home. PCPs and community visiting nurses rarely see infants this complex. Some may be unfamiliar with managing the multiple medical needs of these NICU graduates.12 This often results in parents calling the NICU following discharge to speak with a care team member rather than speaking with the PCP or community visiting nurse. Furthermore, when parents experience difficult transitions from hospital to home, they may seek help through unplanned emergency department visits, outpatient urgent care visits, and sometimes hospital readmissions. Utilizing these already overextended services to care for these medically complex infants and their families is costly, can lead to inconsistent or unnecessary interventions, and misaligns healthcare resources and access for all.
PURPOSE AND AIMSThe purpose of the N2N program was to better prepare parents to care for their medically complex infants at home following discharge from a Level IV NICU to home and to fill the educational gaps of PCPs and community visiting nurses. Through this quality improvement pilot project, our team aimed to:
Mitigate safety risks, through parent education and other interventions, for medically complex infants transitioning from BCH's Level IV NICU to home, as measured by the educational needs identified during the N2N pre- and postdischarge assessments. Assess parent satisfaction with the N2N program as measured via parent follow-up survey. Assess PCPs' satisfaction with the N2N program as measured via PCP survey. Assess community visiting nurses' and PCPs' knowledge deficits about caring for medically complex infants, as measured by PCPs' and community visiting nurses' surveys. Develop educational materials designed to address knowledge deficits identified in aim 4 and evaluate PCPs' and community visiting nurses' engagement with this education. CONTEXTBCH is a 415-bed, Magnet-accredited, quaternary care, free-standing children's hospital. This NICU is a 4-time recipient of the American Association of Critical Care Nursing Gold Beacon Award. The BCH NICU annually cares for more than 650 local, national, and international, medically and surgically complex patients. This Level IV NICU works collaboratively with other Harvard Medical School-affiliated Level I, II, and III newborn care units to deliver neonatal and infant care within the greater Boston area.
PROGRAM DESCRIPTION AND INTERVENTIONSThe N2N program provides comprehensive discharge teaching and follow-up for eligible medically complex infants and their families discharged directly home from the NICU. A select team of 3 experienced NICU nurses led by their nursing director screened for participants, discussed the program with families, and performed predischarge and postdischarge assessments with education. Initially the predischarge assessments were conducted by one of the N2N nurses in the hospital and the postdischarge assessments following discharge were conducted in the participants' homes. However, with the onset of the 2020 Coronavirus pandemic, the project team briefly paused the program as they converted to virtual postdischarge home assessments.
Parents were eligible if they lived in Massachusetts, within 90 miles of the hospital, and there was at least 1 parent or caregiver who was English-speaking, allowing for participation if interpreter services were unavailable. Once eligibility was determined, and parents agreed to participate, an N2N nurse conducted a comprehensive predischarge assessment within 3 days of discharge. This assessment included an evaluation of parents' educational needs and vulnerabilities prior to discharge.
To mitigate safety risks, an experienced, trained nurse conducted and documented predischarge assessments covering an array of general and specific information to the infant's needs. They were able to troubleshoot potential difficulties, increasing the parents' knowledge and readiness to care for their infant once home. Educational gaps identified by the N2N nurse were intervened upon during the predischarge assessments or communicated to the direct care nurses to complete the education following the meeting.
Upon discharge, an N2N nurse coordinated with the family to conduct a follow-up home visit, usually within 7 days of discharge, in the home or virtually, to assess the environment and troubleshoot potential difficulties. When possible, postdischarge assessment of the parent's needs was completed by the same N2N nurse. During postdischarge assessments, the N2N nurses would conduct the same comprehensive evaluation to identify gaps or new information as compared with the predischarge assessment. The predischarge education was reinforced, and any new educational needs since transitioning home were addressed. The N2N nurse coached, verbally supported, and provided supplemental education and materials to parents to care for their infants. The N2N nurse documented their interventions such as the reinforcement of parent education, the mitigation of safety vulnerabilities, and sometimes recommended changes to the infant's environment. They would also verify that parents had an established plan of care and scheduled follow-up with their infant's providers, including the PCP, community visiting nurses, early intervention, DME providers, or other community services. Sometimes this would even involve making a call to the PCP. After the postdischarge assessment, the nurses would document this visit in the patient's electronic medical record, send summaries of their assessments to the PCPs, and distribute satisfaction surveys to parents and PCPs. A trained data coordinator then transferred the data from the assessment forms into a secure Research Electronic Data Capture (REDCap) database for analysis.13,14
In the months following the implementation of the N2N program, the project team conducted educational needs assessments of PCPs and community visiting nurses and developed educational videos intending to increase community providers' knowledge of caring for medically complex infants. As part of the PCPs' 8-item REDCap satisfaction survey, they were asked about gaps in knowledge for themselves and their staff when caring for medically complex infants. For the community visiting nurses, a 10-section, 104-item survey was conducted to assess their educational needs. The project team identified community visiting nurses' organizations that had previously cared for infants discharged home from the NICU and sent the assessment via e-mail to the nurse leaders of these organizations, who then distributed the assessment among their nursing staff.
The educational videos were developed and distributed by OPENPediatrics an online, free resource that allows healthcare professionals to access peer-reviewed content highlighting best practices.15 OPENPediatrics is a nonprofit, interactive digital learning platform designed to provide the best practices, teachings, and promote knowledge sharing among a global community of pediatric healthcare professionals. Video authors and speakers are subject matter experts in their respective fields. Advanced practice nurse experts developed content for the N2N program videos based on BCH policies, procedures, and guidelines. Before they are launched, all videos published on OPENPediatrics are reviewed by peer reviewers and medical/nursing education experts to ensure the accuracy of videos, assuring best practices are conveyed. Videos are reviewed every 3 years for relevancy, accuracy, and to facilitate sustainability. With each N2N video launch, announcements were sent via e-mail to PCP offices and the community visiting nurse agencies participating in the needs assessments. Recipients were asked to share the link to the educational videos with their staff.
The project team envisioned that deeper family support, through pre- and postdischarge assessments and community provider education, would improve the transition of care from hospital to home for NICU families, helping our most vulnerable patients thrive, increase satisfaction among parents and PCPs, and improve community providers' knowledge of caring for medically complex infants.
MEASUREMENT Specific Aim 1: Mitigate Safety RisksThe nurse's documentation of parents' educational needs and vulnerabilities and their interventions served as the safety risk mitigation measures.
Specific Aim 2: Assess Parent SatisfactionTo measure parent satisfaction following the postdischarge assessment, parents were provided with a 10-item satisfaction survey with Likert-scale response options (strongly disagree to strongly agree) and one open-ended item. They asked parents to complete the survey and describe their satisfaction with the N2N program.
Specific Aim 3: Assess PCPs SatisfactionTo measure satisfaction, an 8-item REDCap survey was sent to providers through e-mail or fax following the postdischarge assessment with parents to assess the PCPs satisfaction with the N2N program. The survey asked PCPs to confirm receiving the N2N program summary from the nurses and if they were satisfied with the communication they received in the summary.
Specific Aim 4: Assess Community Visiting Nurses' and PCPs' KnowledgeThe study team distributed surveys to assess and measure PCPs' and community visiting nurses' knowledge about caring for medically complex infants.
Specific Aim 5: Develop Educational Materials Designed to Address Knowledge Deficits Identified in Aim 4 and Evaluate PCPs' and Community Visiting Nurses' Engagement With This EducationAs a measure of success, the project team monitored and summarized the number of views for each OPENPediatrics video using descriptive statistics.
ANALYSISDescriptive statistics were utilized to summarize the findings for each study aim. Qualitative descriptions from open-ended question responses on satisfaction surveys are provided to exemplify outcomes.
ETHICAL CONSIDERATIONSThis quality improvement project was deemed exempt from BCH Institutional Review Board approval and oversight.
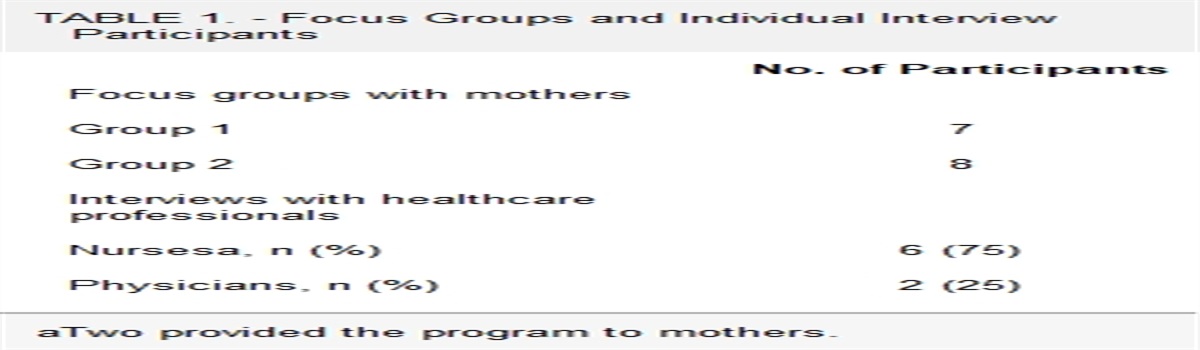
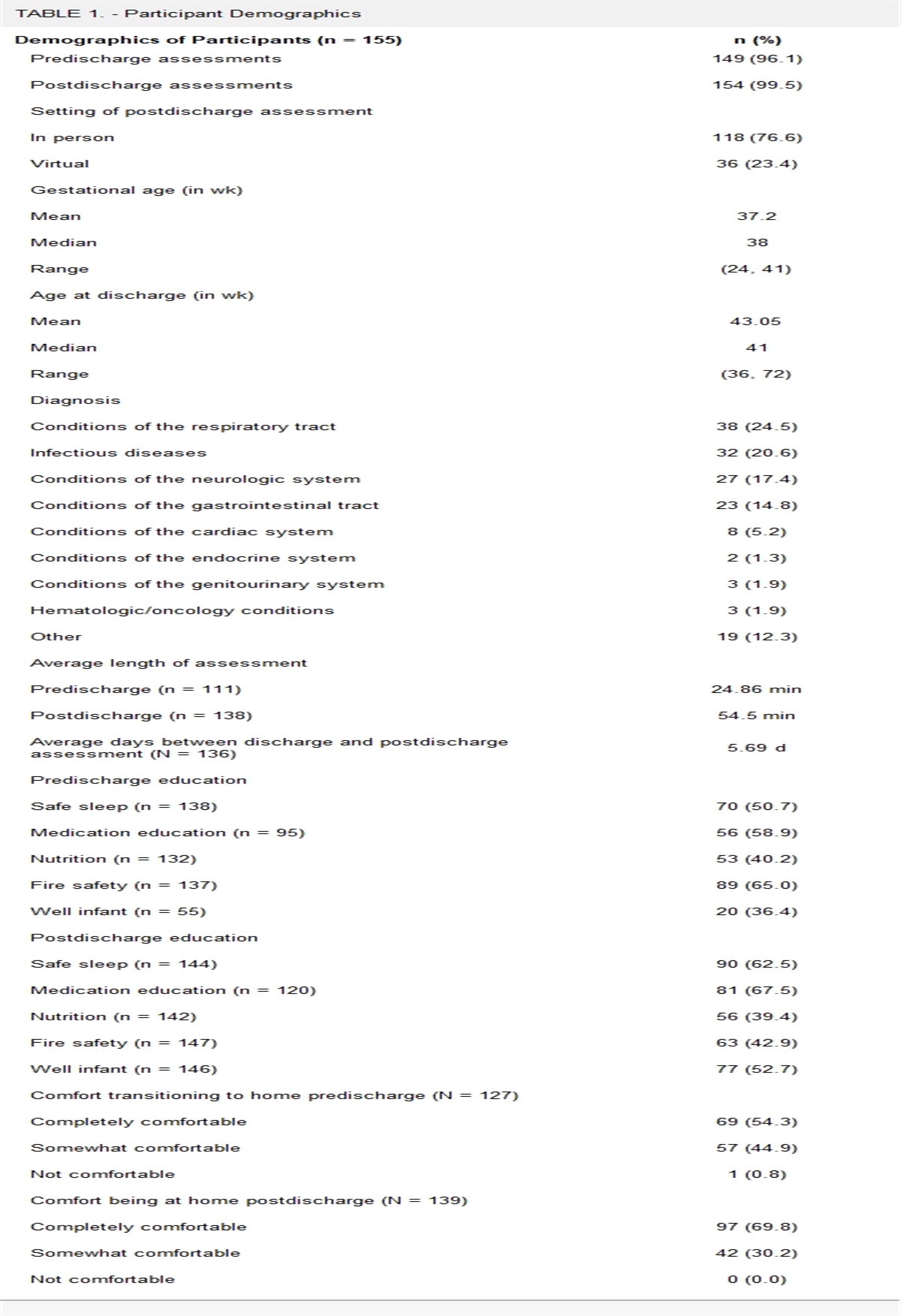
RESULTS Participant CharacteristicsA total of 155 parents participated in the N2N program between January 18, 2018, and December 26, 2020, (Table 1). There were 149 predischarge assessments and 154 postdischarge assessments. Six participants did not receive a predischarge assessment, and 1 declined a postdischarge assessment. The mean gestational age of the infants at birth was 37.2 weeks (24-41 weeks), and the mean gestational age at discharge was 43.05 weeks (36 weeks to 8 months). Discharge diagnoses of infants included conditions of the respiratory tract (24.5%), infectious diseases (20.6%), conditions of the neurological system (17.4%), and conditions of the gastrointestinal tract (14.8%). The average length of predischarge assessments were 24.86 minutes, and the postdischarge assessments lasted an average of 54.5 minutes. The average number of days between discharge and the postdischarge assessment was 5.69 days. 76.7% of postdischarge assessments were conducted in-person, and 23.4% were held virtually.
TABLE 1. - Participant Demographics Demographics of Participants (n = 155) n (%) Predischarge assessments 149 (96.1) Postdischarge assessments 154 (99.5) Setting of postdischarge assessment In person 118 (76.6) Virtual 36 (23.4) Gestational age (in wk) Mean 37.2 Median 38 Range (24, 41) Age at discharge (in wk) Mean 43.05 Median 41 Range (36, 72) Diagnosis Conditions of the respiratory tract 38 (24.5) Infectious diseases 32 (20.6) Conditions of the neurologic system 27 (17.4) Conditions of the gastrointestinal tract 23 (14.8) Conditions of the cardiac system 8 (5.2) Conditions of the endocrine system 2 (1.3) Conditions of the genitourinary system 3 (1.9) Hematologic/oncology conditions 3 (1.9) Other 19 (12.3) Average length of assessment Predischarge (n = 111) 24.86 min Postdischarge (n = 138) 54.5 min Average days between discharge and postdischarge assessment (N = 136) 5.69 d Predischarge education Safe sleep (n = 138) 70 (50.7) Medication education (n = 95) 56 (58.9) Nutrition (n = 132) 53 (40.2) Fire safety (n = 137) 89 (65.0) Well infant (n = 55) 20 (36.4) Postdischarge education Safe sleep (n = 144) 90 (62.5) Medication education (n = 120) 81 (67.5) Nutrition (n = 142) 56 (39.4) Fire safety (n = 147) 63 (42.9) Well infant (n = 146) 77 (52.7) Comfort transitioning to home predischarge (N = 127) Completely comfortable 69 (54.3) Somewhat comfortable 57 (44.9) Not comfortable 1 (0.8) Comfort being at home postdischarge (N = 139) Completely comfortable 97 (69.8) Somewhat comfortable 42 (30.2) Not comfortable 0 (0.0)During the predischarge assessments, most parents received educational interventions on fire safety (65.0%), medication education (58.9%), and safe sleep (50.7%). The most frequent educational interventions observed and reinforced at the postdischarge assessments included medication education (67.5%), safe sleep (62.5%), and well-infant care (52.7%). Of those with DME, 70.8% of parents needed additional education interventions. When nurses asked parents about transitioning to home predischarge, approximately half reported being completely comfortable (54.3%) or somewhat comfortable (44.9%). Postdischarge, the nurses asked parents about their comfort being home with their infants; most parents reported feeling completely comfortable (69.8%), and the remaining parents reported they were somewhat comfortable (30.2%).
Table 2 shows significant nurse interventions that exemplify the mitigation of safety risks, including the navigation of the healthcare system related to seizure management, securement of a feeding tube, as well as modification of anticoagulant therapy administration practices in the home.
TABLE 2. - Examples of Infant Safety Risk Mitigations Encountered by N2N Nurses Infant “Z” is a 2-wk-old former 37-wk gestation infant with seizures, discharged home following stabilization on phenobarbital. Seven days later, during an N2N postassessment, the parents reported to the nurse the infant's seizures had reoccurred and persisted despite having a recent phenobarbital dose adjustment. The N2N nurse facilitated contact with the neurologist on call and the infant was subsequently readmitted to the hospital later that day. Infant “E” was discharged home from the NICU with a tracheostomy and nasogastric tube in situ. Seven days later, during the N2N postassessment, the mother reported the nasogastric tube had fallen out 2 d ago. She was breastfeeding her infant instead of feeding through the nasogastric tube. According to the mother, she had gone to the pediatrician's office that same day and her infant was losing weight. She was having trouble navigating the healthcare system to have the small 6.5 Fr nasogastric tube replaced. Furthermore, the pediatrician prescribed the infant antibiotics for a tracheal infection. The N2N nurse intervened, helping the mother assess her infant's needs. A plan was put in place to have the nasogastric tube replaced later that day, and an order was placed with a vendor for a supply of small 6.5 Fr feeding tubes. The next day the NICU to nursery nurse followed up with the mother and confirmed the nasogastric tube had been replaced and the infant had been started on her antibiotics. Infant “F,” a former 39-wk gestation infant with a vein of Galen/straight sinus thrombus was discharged home on enoxaparin receiving weekly laboratory test results to check for therapeutic levels. During the home visit by the N2N nurse an underdosing of enoxaparin was identified when she reviewed and observed the parents preparing the injection. Outpatient pharmacies dispense prefilled enoxaprin syringes that require parents to attach a needle for injection for administration. After priming the needle there was approximately 20% less of the prescribed medication left in the syringe. The patient had a therapeutic level the day of discharge, but a subtherapeutic enoxaparin level 3 d after discharge. Upon further investigation the N2N team learned that the hospital pharmacy provides a small amount of enoxaparin “overfill” to account for needle priming to ensure accurate dosing. It was presumed that the subtherapeutic level was due to underdosing of multiple enoxaparin doses at home by parents before obtaining the outpatient enoxaparin level. In response the N2N program team established standardization for all outpatient dispensed enoxaparin that has been implemented across the institution. This new process was developed in collaboration with outpatient pharmacies to include attaching needles to each prefilled syringe and priming to the exact prescribed dose to ensure accurate home medication administration, eliminating drug loss.Abbreviations: N2N, NICU to nursery; NICU, neonatal intensive care unit.
A total of 41.9% of parents completed the parent satisfaction surveys (Tables 3 and 4). Most parents also found that the pre- and postdischarge assessment provided an opportunity to ask questions or receive clarification about their infant's care (95.4% and 93.8%, respectively). Most parents (95.4%) reported that the N2N postdischarge assessment and education interventions helped them feel more confident and knowledgeable regarding the care of their infant. Topics parents report having asked questions or received clarification about included monitoring of their infants (73.4%), supportive resources (68.8%), follow-up appointments (60.9%), medications (39.1%), and treatments (39.1%).
TABLE 3. - Parent Satisfaction With N2N Program Parent Satisfaction Disagree Agree The predischarge assessment provided an opportunity to ask questions or receive clarification about the care of my infant (N = 65) 3 (4.6) 62 (95.4) The predischarge assessment helped me consider the layout of my home related to the care of my infant (storage of supplies, safe sleep space for my infant) (N = 64) 7 (10.9) 57 (89.1) The predischarge assessment helped me feel more knowledgeable regarding the care of my infant (N = 65) 3 (4.6) 62 (95.4) The predischarge assessment helped me feel more confident regarding the care of my infant (N = 65) 4 (6.2) 61 (93.8) The predischarge assessment helped me think about the safety of my home related to the care of my infant that I had not thought about before discharge (N = 40) 8 (20.0) 32 (80.0) The postdischarge assessment helped me think about the safety of my home related to the care of my infant that I had not thought about before discharge (N = 65) 16 (24.6) 49 (75.4) The postdischarge assessment helped me consider the layout of my home related to the care of my infant that I had not thought about before discharge (N = 65) 20 (30.8) 45 (69.2) The postdischarge assessment helped me feel more knowledgeable regarding the care of my infant (N = 65) 3 (4.6) 62 (95.4) The postdischarge assessment helped me feel more confident regarding the care of my infant (N = 65) 3 (4.6) 62 (95.4) The postdischarge assessment provided an opportunity to ask questions or receive clarification about the care of my infant that I had not thought about before discharge (N = 65) 4 (6.2) 61 (93.8)Abbreviations: BCH, Boston Children's Hospital; NICU, neonatal intensive care unit.
A total of 138 unique providers were sent the provider satisfaction surveys and 20% of the PCPs completed at least 1 follow-up survey (Table 5). Of those providers, 92.6% were physicians, 3.7% were nurse practitioners, and 3.7% were nurses. Of providers who responded to the surveys, 96.3% were from a pediatric primary care office. The majority of providers (84%) found the postdischarge assessment summary report helpful. Respondents' suggestions for improvements included providing a more concise summary report, information about who pays for the program, and adding recommendations for future care to the summary report sent by the N2N nurses.
TABLE 5. - Provider Satisfaction With N2N Program Provider Satisfaction n (%) Role at the pediatric primary care office (n = 27) Physician 25 (92.6) Nurse practitioner 1 (3.7) Nurse 1 (3.7) Type of practice (n = 27) Pediatric primary care 26 (96.3) Family medicine 1 (3.7) Academic affiliate 1 (3.7) Do you recall receiving the N2N assessment summary? (n = 24) Yes 21 (87.5) No 3 (12.5) Was the N2N assessment summary helpful? (n = 25) Yes 21 (81.4) No 4 (16.0) Which of the following educational content would be beneficial for you or your staff? (n = 16) Tubes and drains 8 (50.0) Growth and nutrition 7 (43.8) Emergency response care 6 (37.5) Newborn care 5 (31.3) Respiratory assessment 2 (12.5) Neurological assessment 2 (12.5) Medication 1 (6.3) Routine healthcare 1 (6.3) Other 3 (18.8)Abbreviation: N2N, Neonatal Intensive Care Unit to Nursery.
Educational needs identified by PCPs, for themselves and their staff included care and management of tubes and drains (50%), growth and nutrition (43.8%), and emergency response care (37.5%). In addition, 20 nurses from 6 community visiting nurse agencies within Massachusetts responded to the needs assessment survey. Neonatal topics and skills community visiting nurses reported being very uncomfortable, uncomfortable, or neutral included heart murmur assessments (70%), insertion of nasogastric tubes (72.2%), and tracheostomy tube replacements (65%) as shown in Table 6.
TABLE 6. - Community Visiting Nurse Needs Assessment Uncomfortable Comfortable Newborn care (N = 20) Bathing, temperature 1 (5.0) 19 (95.0) Cord care 3 (15.0) 17 (85.0) Jaundice 4 (20.0) 16 (80.0) Sleeping patterns, developmental care 2 (10.0) 18 (90.0) Infant safety, positioning, and sleep 0 (0.0) 20 (100.0) Respiratory assessment and management (N = 20) Respiratory ratea 2 (10.5) 17 (89.5) Retractions 5 (25.0) 15 (75.0) Color 3 (15.0) 17 (85.0) Quality: stridor, rales 6 (30.0) 14 (70.0) Delivery of oxygen, nasal cannula; oxygen saturation monitoring 1 (5.0) 19 (95.0) Delivery of oxygen, CPAP, Bi-PAP 9 (45.0) 11 (55.0) 2 regulator/tank 4 (20.0) 16 (80.0) Ventilator 13 (65.0) 7 (35.0) Hand ventilation 10 (50.0) 10 (50.0) Apnea/periodic breathing monitoring 10 (50.0) 10 (50.0) Oral suctioning 2 (10.0) 18 (90.0) Nasopharyngeal suctioning 5 (25.0) 15 (75.0) Tracheostomy care, securement 7 (35.0) 13 (65.0) Tracheostomy evaluation of site, suctioning 5 (25.0) 15 (75.0) Tracheostomy HME: bathing 9 (45.0) 11 (55.0) Tracheostomy humidification 6 (30.0) 14 (70.0) Tracheostomy replacement 13 (65.0) 7 (35.0) Emergency management of tracheostomy 12 (60.0) 8 (40.0) Cardiovascular assessment (N = 20) Heart rate 1 (5.0) 19 (95.0) Heart rate monitoring 2 (10.0) 18 (90.0) Murmurs 14 (70.0) 6 (30.0) Color/capillary refill/perfusion 3 (15.0) 17 (85.0) Signs and symptoms of congestive heart failure 11 (55.0) 9 (45.0) Gastrointestinal and genitourinary assessment (N = 19) Abdominal appearance 6 (31.6) 13 (68.4) Bowel sounds 2 (10.5) 17 (89.5) Stool patternb 2 (10.5) 16 (84.2) Colostomy/ileostomy care and bag/appliance change 7 (36.8) 12 (63.2) Assessing ostomy site and skin 5 (26.3) 14 (73.7) Normal voiding pattern 1 (5.3) 18 (94.7) Circumcision 6 (31.6) 13 (68.4) Straight cath 4 (21.1) 15 (78.9) Fistula care 11 (57.9) 8 (42.1) Rectal dilations 13 (68.4) 6 (31.6) Neurological assessment (N = 19) Head circumference 4 (21.1) 15 (78.9) Fontanel 3 (15.8) 16 (84.2) Sutures 8 (42.1) 11 (57.9) Pupils 4 (21.1) 15 (78.9) Reflexes 8 (42.1) 11 (57.9) Seizure assessment 6 (31.6) 13 (68.4) Seizure management 8 (42.1) 11 (57.9) Signs and symptoms of abnormal neurologic examination, increased intracranial pressure, and shunt assessment 12 (63.2) 7 (36.8) Growth and nutrition (N = 18) Nutritional requirements 6 (33.3) 12 (66.7) Lactation, human milk/formula storage 3 (16.7) 15 (83.3) Use of expressed human milk 4 (22.2) 14 (77.8) Formula feeding 2 (11.1) 16 (88.9) Formula preparation 1 (5.6) 17 (94.4)
留言 (0)