
記住我
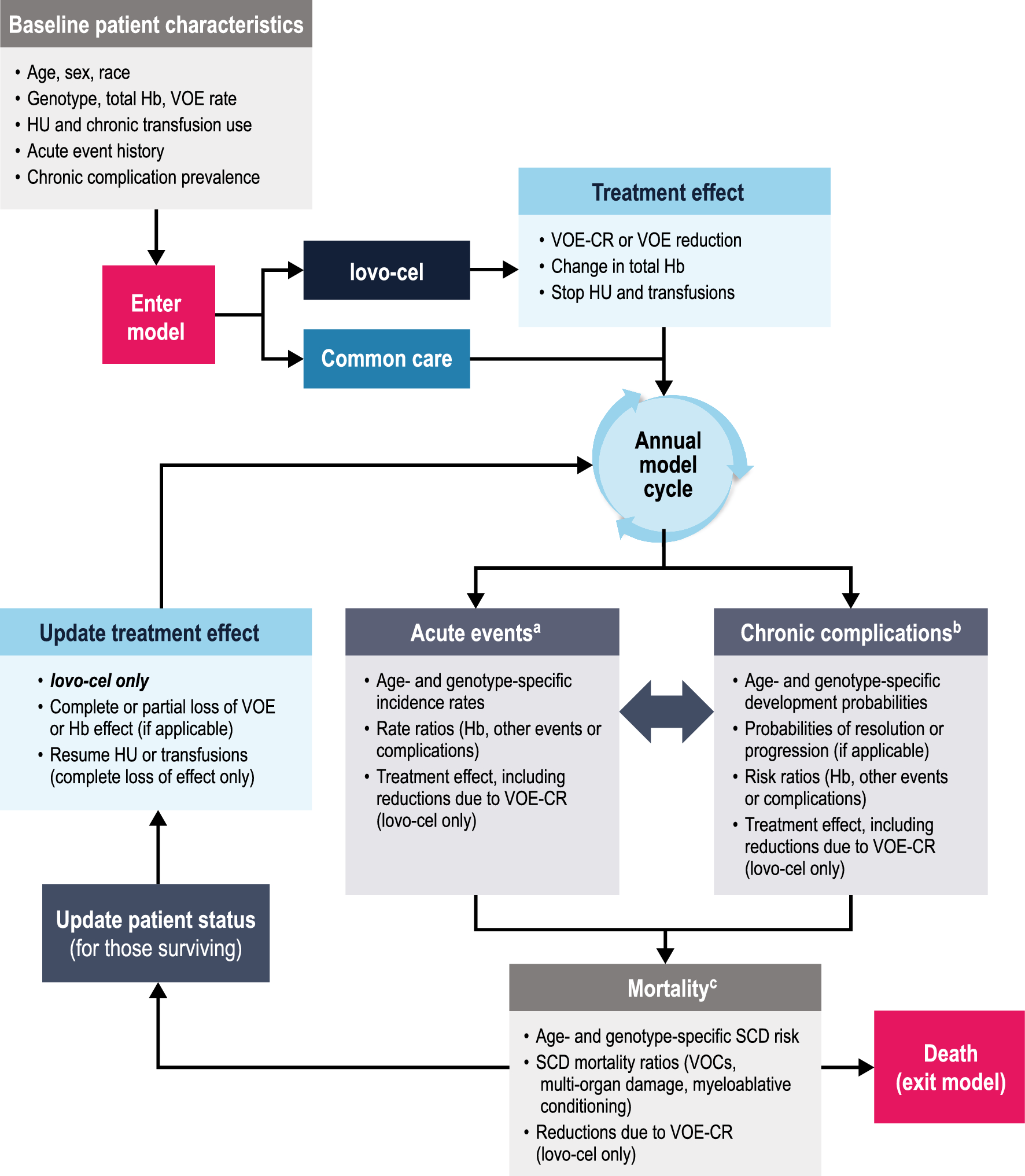
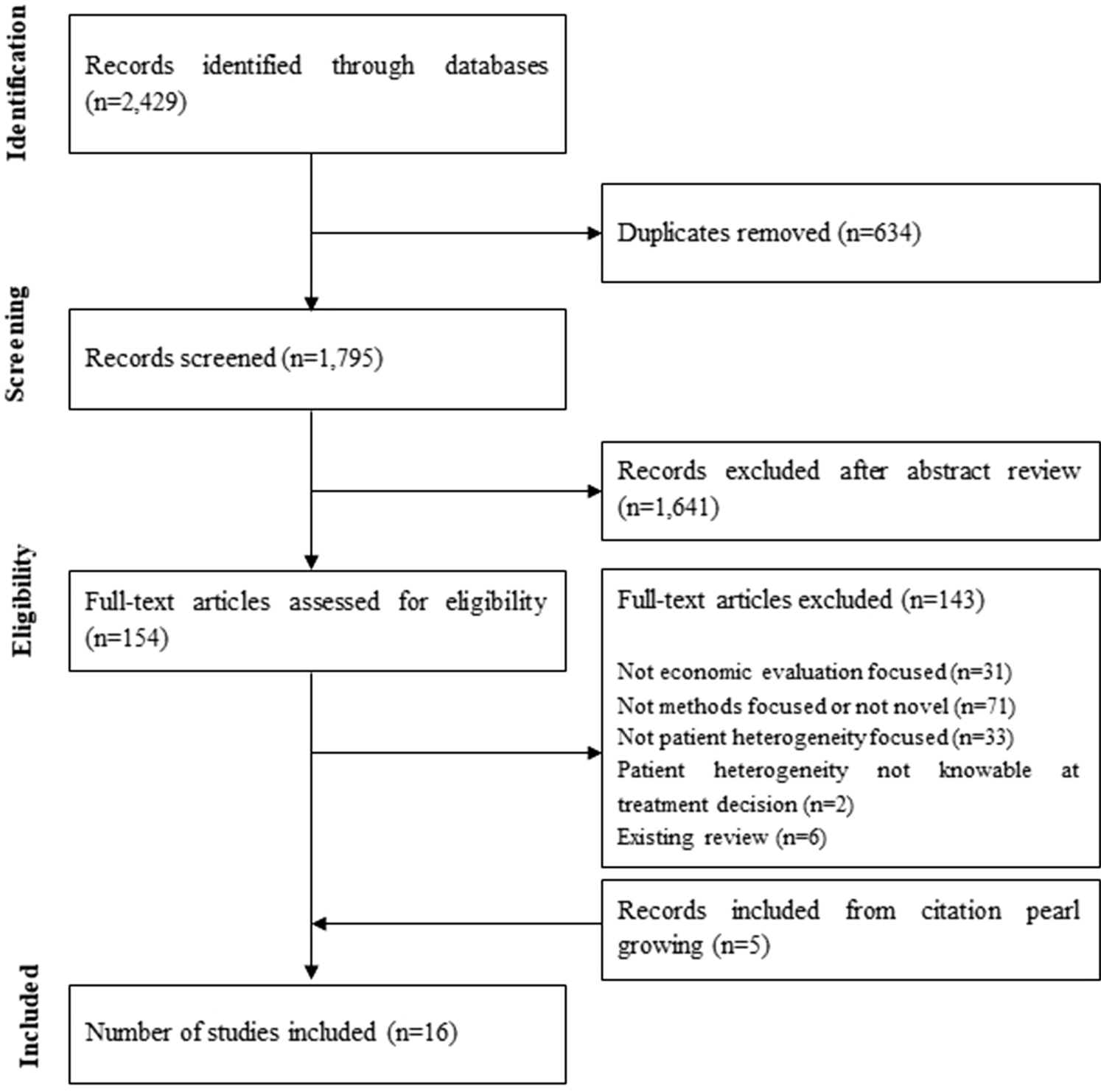

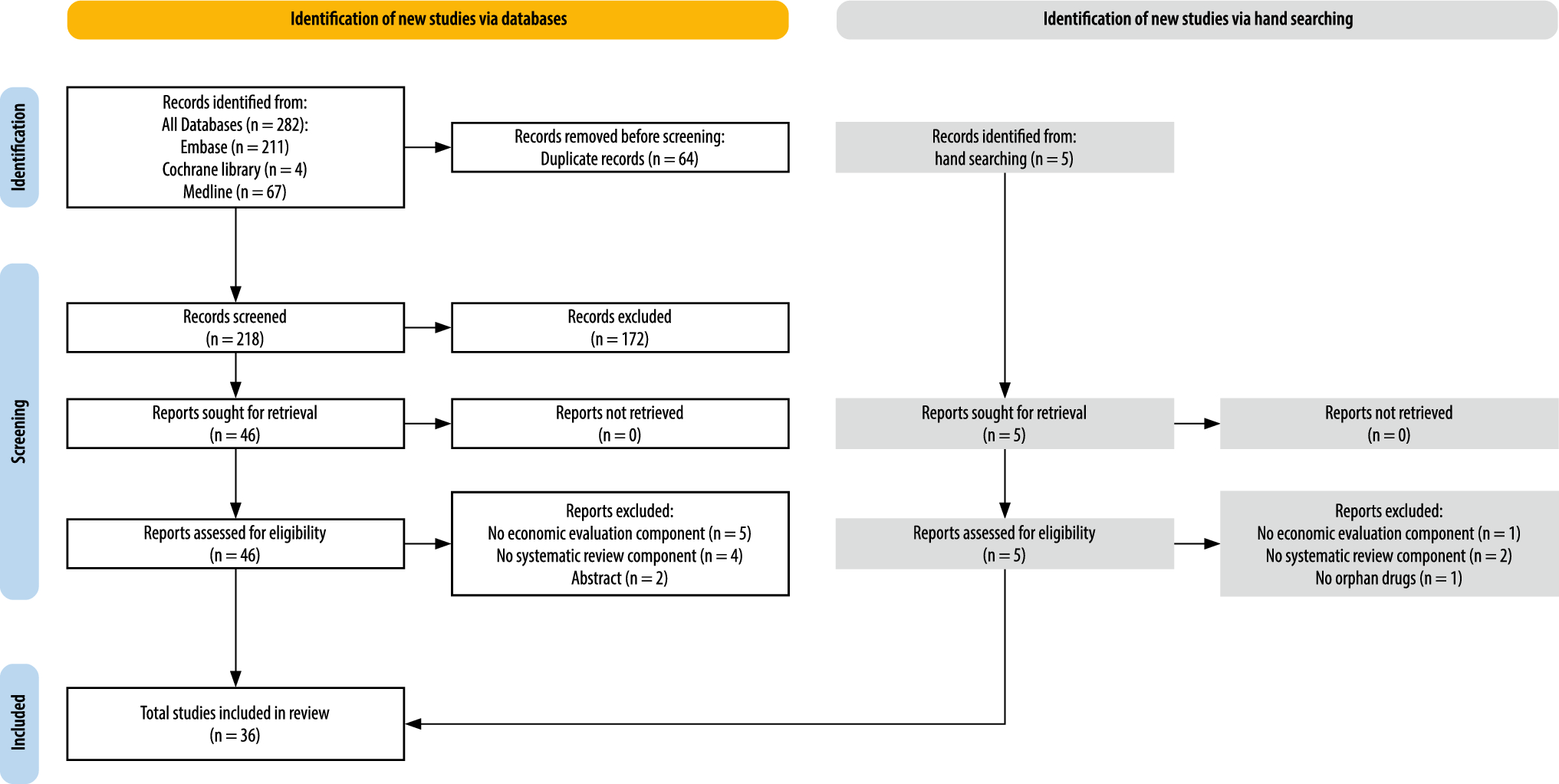
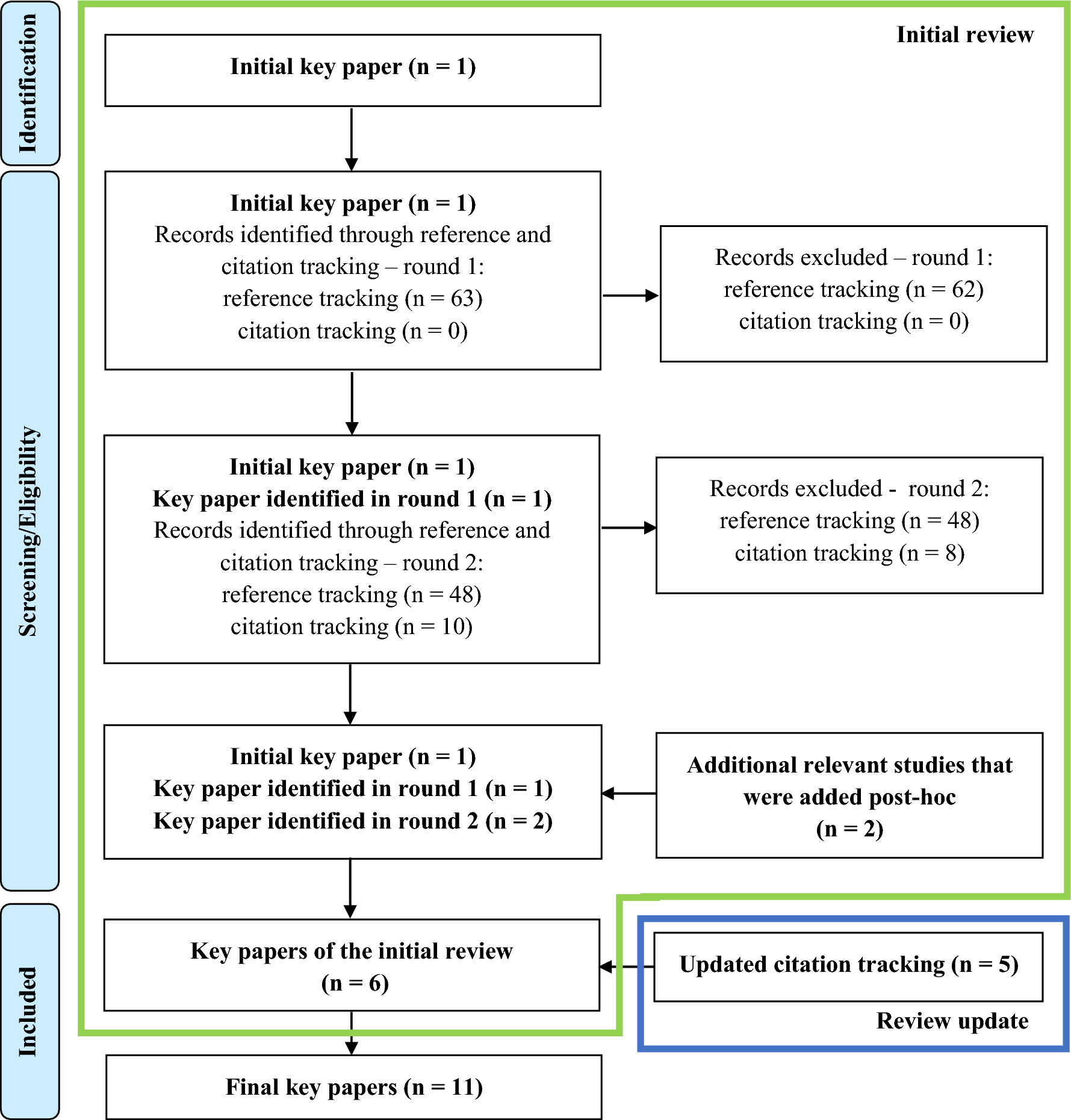

After duplicate removal, our search strategy resulted in 2314 unique records. After title and abstract screening, 99 studies were included in the full-text screening process. From these 99 studies, 20 were deemed eligible according to the inclusion and exclusion criteria and were selected for data extraction and quality appraisal. Upon further revision, two publications were deemed to be duplicate reports of the same study, and thus only one [18] was kept for data extraction and evaluation. Two further studies fulfilling the criteria were included as articles in-press [19, 20] after the search was concluded but before starting the data extraction and quality appraisal. In total, this systematic review includes 21 studies. The searching, screening and inclusion procedure is summarised in the PRISMA flowchart in Fig. 1.
Fig. 1 3.2 Quality appraisal
3.2 Quality appraisalOverall, the quality of the studies was deemed very high, with most studies obtaining above 85% fulfilment of criteria in both the Drummond and the CHEERS checklist (Fig. 2). The overall average percentages for the Drummond checklist were 90% and for CHEERS 88%. The percentages of fulfilment for each study were similar in both checklists. The item with most negative scores in Drummond was item 16 (“Quantities of resource use are reported separately from their unit costs”), while in CHEERS it was the early planning of health economic analysis. The Drummond and CHEERS assessment results can be found in Appendices 4 and 5.
Fig. 2
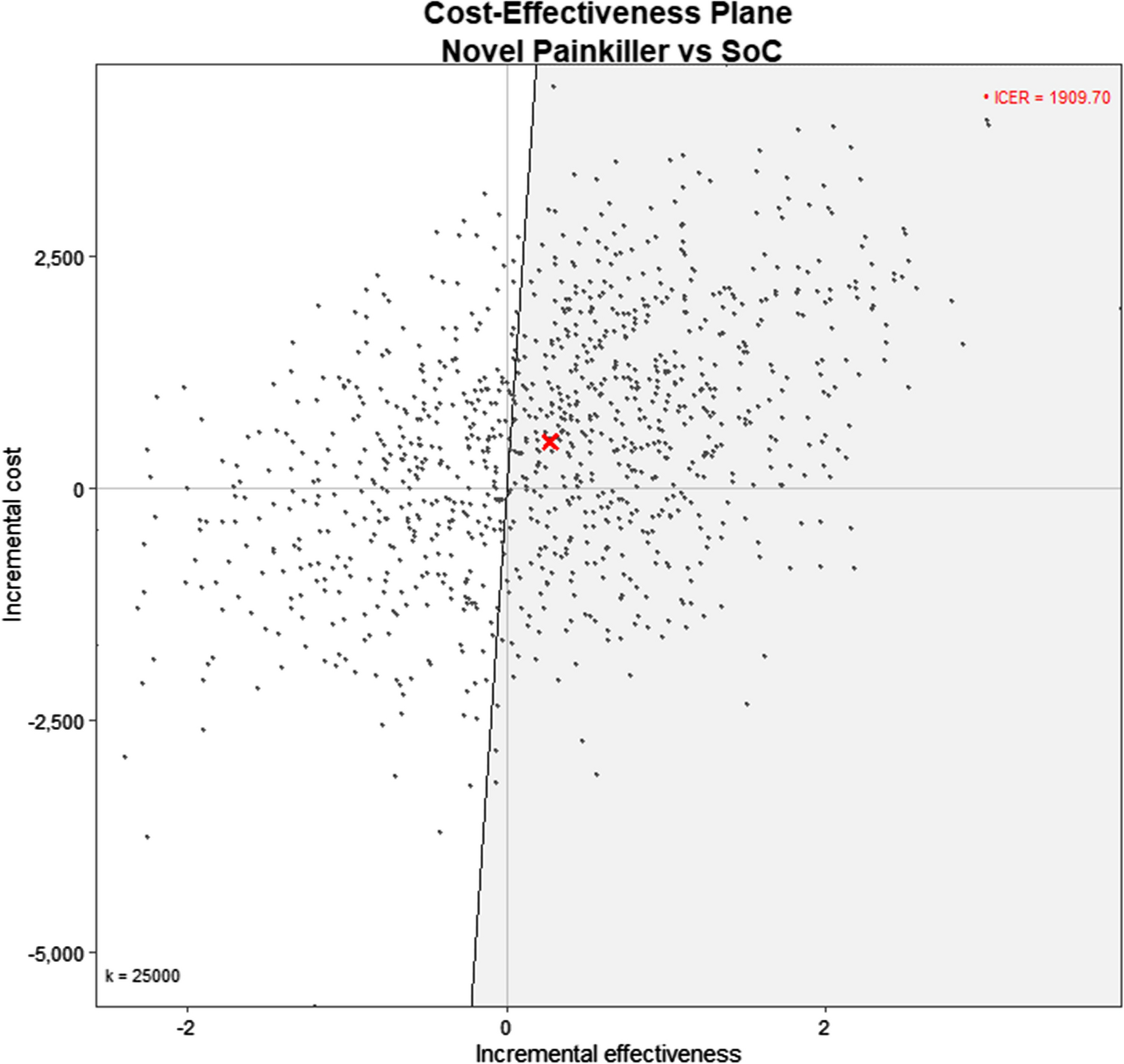
Cost-adapted results from different health strategies (healthcare perspective) presented in a common cost-effectiveness plane for costs (2022 USD) and QALYs. Strategies were included in the cost-effectiveness plane if they reported health benefits and costs per person, if costs were adaptable to 2023 USD and if the comparator was standard of care (i.e. for studies that evaluated several strategies and compared several against the next best alternative, only the one comparing against standard of care was included). Strategies that did not fulfil these criteria could not be presented in a common same cost-effectiveness plane. 1. Marang et al. [28], 2. Oliva et al. [31], 3. Nherera et al. [24], 4. Ademi et al. (2014) [20], 5. Lazaro et al. [32], 6. Kerr et al. [25], 7. McKay et al. [26], 8. Crosland et al. [30], 9. Ademi et al. (2020) [21], 10. Ontario Health [37], 11. Spencer et al. [34], 12.Marquina et al. (2021) [23], 13. Ademi et al. (2023) [18], 14. Marquina et al. (2023) [19]
3.3 General characteristics of the included studiesOf the 21 included studies, five studies were set in Australia [20, 21, 22, 23], four in the UK [24, 25, 26, 27], three in the Netherlands [19, 28, 29], two in England and Wales [18, 30], two in Spain [31, 32], two in the USA [33, 34], one in Poland [35], one in Argentina [36], and one in Canada [37]. All the studies were reported in English. All studies were published in peer-reviewed journals except the one set in Canada, which was published by Ontario’s Health Technology Assessment (HTA) agency [37]. None of the studies were set in low or middle-income countries. Most studies evaluated more than one screening strategy or different types of case ascertainment (and hence the number of strategies evaluated is larger than the total number of included studies). Of the selected studies, 17 evaluated cascade screening, either as a standalone strategy [18, 19, 22, 23, 24, 25, 28, 29, 31, 33, 37] or in combination with other strategies [26, 30, 32, 35, 36, 38]. Six studies evaluated a population-wide screening strategy [18, 21, 26, 34, 35, 36], four evaluated an opportunistic strategy (in most cases followed by cascade screening) [18, 32, 35, 38], and three evaluated a systematic screening strategy using electronic medical records [20, 27, 30]. General characteristics for the included studies are presented in Table 1.
Table 1. General characteristics of the included studiesMost of the studies (80%) used a lifetime horizon for the evaluation, while Ademi et al. [23] and Lazaro et al. [32] used a 10-year horizon, Spencer et al. [34] a 20-year, and Jones et al. [27] a 12-weeks horizon. In all. 6 studies used a decision tree for their analysis [18, 24, 27, 29, 32, 36] mostly based on life-table data, and 13 used a decision tree followed by a Markov model [19, 20, 21, 22, 23, 25, 26, 30, 33, 34, 35, 37, 38]. In addition, two studies did not describe the analytical design [28, 31]. Most studies (71%) reported cost per QALY gained as the main outcome of interest, four reported cost per life year gained (LYG) [18, 28, 29, 31] (of note, all four were published before 2010), one study reported both cost per quality-adjusted life-year (QALY) and cost per LYG as the main outcome [36], and one study reported cost per FH case detected [27]. For studies that reported QALYs, 10 studies used the EQ-5D instrument for the utility weights [19, 20, 21, 22, 23, 24, 32, 33, 37, 38]. Out of the 21 included studies, 6 included strategies focusing on children (from age 1–10 years) [19, 22, 26, 36, 38] or adolescents (16 years) [18] as their target population, and the remaining focused on adult populations.
From the included studies, only three reported the number needed to screen (i.e. the number of people that needs to undergo screening to avoid one adverse outcome).
3.4 Screening strategiesThere were four main screening strategies that were evaluated: (1) cascade screening, which involved the screening of relatives of an index case with diagnosed or suspected FH; (2) opportunistic screening, which involved offering screening to any individual with or without symptoms as they present to a health care practice or other institutions (i.e. schools) for reasons unrelated to the disease; (3) systematic screening, which usually involved screening of some form of medical records to detect potential FH cases and differs from universal screening in that a prior step trying to identify high-risk individuals is conducted before the actual FH case ascertainment; and (4) population-wide screening, which involved the screening of a whole defined segment of the population with no prior criteria for detecting high-risk individuals.
3.4.1 Casca
留言 (0)