
記住我









This study is a retrospective comparative research effort in which all patient names have been anonymized. Since the anonymized data cannot reveal the identity information of the patients, informed consent is not required. The Human Research and Ethics Committee of CQMU had approved this study (NO: 2022-K525).
DesignThe study utilizes the electronic medical record system of CQMU to extract data according to predefined variables. It then investigates the relationship with ECT effectiveness using logistic regression model analyses, controlling for confounding variables.
ParticipantsAll participants were psychiatric inpatients 18 years old or younger at CQMU, with discharge dates between December 31, 2016, and June 30, 2021 (n = 2231).
Inclusion criteria(1) Receiving ECT. (2) Meeting the diagnostic standards in ICD-10, such as F32.2 (Severe depressive episode without psychotic symptoms) and F32.3 (Severe depressive episode with psychotic symptoms). (3) Clear suicidal intention or attempt, as indicated by the Columbia Suicide Severity Rating Scale (C-SSRS).
Exclusion criteria(1) Diagnoses including F00-F09 (Organic mental disorders), F10-F19 (Mental and behavioral disorders resulting from psychoactive substance use), F20-F29 (Schizophrenia), F30–F31.9 (Manic episode, Bipolar affective disorder), F70–F79 (Mental retardation). (2) Absence of Clinical Global Impressions–Improvement scale (CGI-I) score.
Grouping standardsEmploying the CGI-I score at discharge for evaluating overall efficacy as the basis for division, and first defining overall efficacy as: (1) Positive response: CGI-I score 1 (very much improved) or 2 (much improved). (2) Negative response: 3 (Minimally improved), 4 (No change).
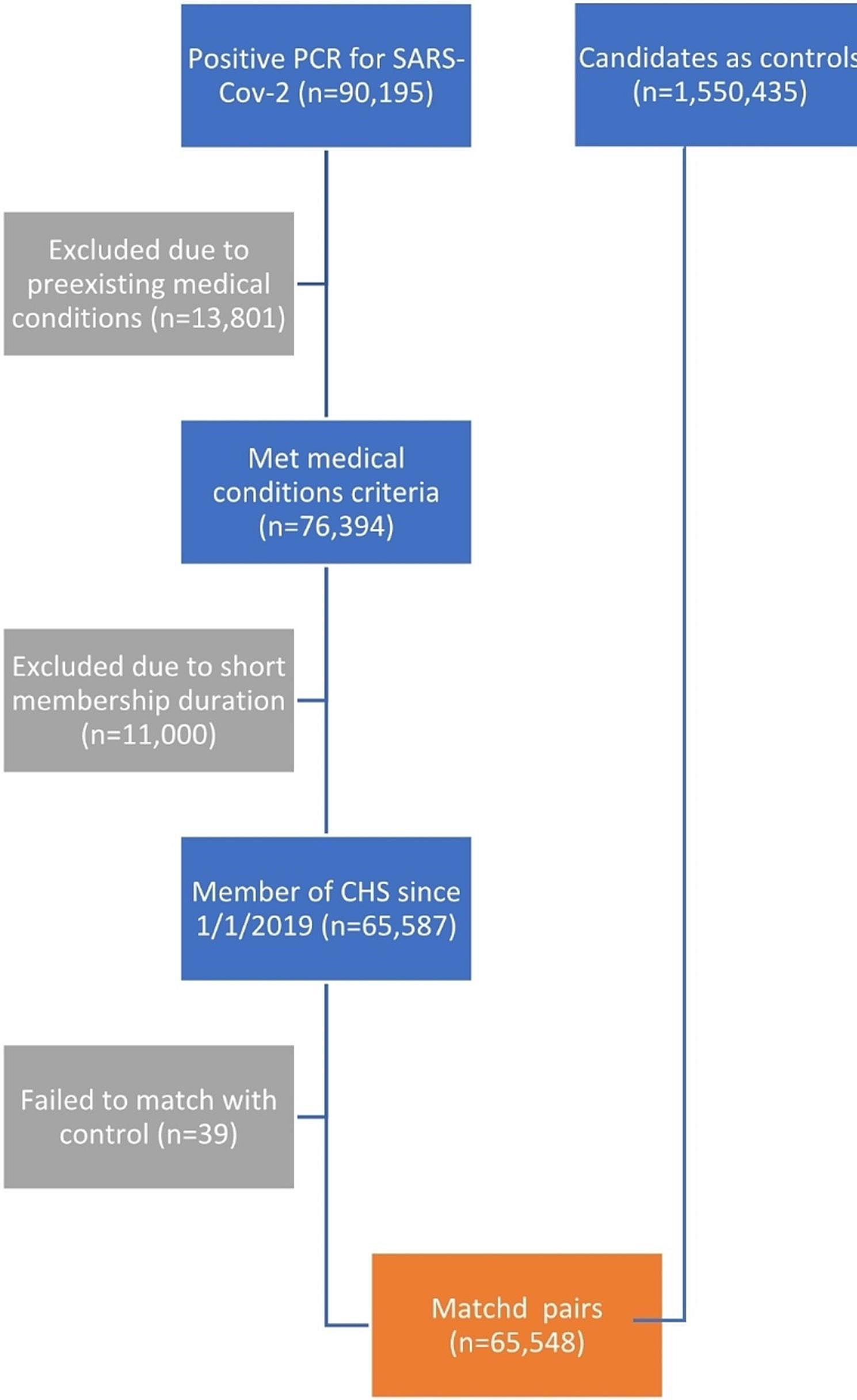
Patients were then categorized into effective and ineffective groups according to the CGI-I positive or negative response, and other variable data were extracted from medical records. The procedure is illustrated in Fig. 1.
Fig. 1 Variables and measuresDemographic variables
Variables and measuresDemographic variablesAge, gender, family history of psychiatric illness, family history of suicidal deaths. Family history is confined to two families and three generations, with only relatives definitively diagnosed with psychiatric illness assessed as positive.
Disease variablesDisease duration, psychotic symptoms, suicide attempts within the last month, hospitalizations at CQMU, hospitalizations at other psychiatric hospitals, Hamilton Depression Rating Scale (HAMD) score, Hamilton Anxiety Scale (HAMA) score, psychiatric comorbidities. Disease duration is the time from initial depression symptoms to current admission. The evaluation of psychotic symptoms is limited to whether they were present during the current hospital stay. Suicide attempts within the last month refer to the actual number of intentional actions taken to end one’s life but survived in the month prior to admission [22]. HAMD and HAMA scores are ratings at the time of admission.
Medication treatment variablesAntidepressants, doses of antidepressants, fluoxetine equivalent dose, antipsychotics, doses of antipsychotics, olanzapine equivalent dose, mood stabilizers, sedative-hypnotics and other anti-anxiety drugs. Medication treatment encompasses the entire inpatient treatment period, besides mood stabilizers, they are prohibited from use during the ECT sessions period and are only prescribed in the discharge prescription after the ECTs. All medication treatment variables are selected at the time of discharge, and the units are consistently measured in mg. The doses of antidepressants and antipsychotics are converted to fluoxetine equivalent dose [23] and olanzapine equivalent dose [24, 25], respectively, to ensure comparability. The transformed variables were not entered into the statistical analysis.
Variables of ECT treatmentECT sessions, severe side effects of ECT, previous ECT treatment history. ECT sessions were provided for the duration of the current hospitalization, without maintenance ECTs. Severe side effects of ECT are defined as those that substantially affect function, manifest clear signs upon physical examination, and necessitate intervention.
Other variablesDays hospitalized.
Electroconvulsive therapyAll patients and their lawful guardians voluntarily accepted electroconvulsive therapy after being fully informed about the risks and benefits. The lawful guardians then completed the signing of the informed consent document. Prior to treatment, all physicians in the patient's medical team conducted a pre-treatment discussion to evaluate the indications and contraindications for ECT. The patient retains the right to demand the cessation of electroconvulsive therapy at any time.
All ECT sessions were modified and conducted using the Thymatron DGx system (SomaticsLLC, Lake Bluff, IL, USA), following a brief pulse pattern with bitemporal electrode placement. The initial electrical dose was determined by the formula age * 0.7, with subsequent electrical volumes titrated by 5% in response to seizures [26]. The standard treatment frequency is two or three times a week. However, if urgent needs arise or a patient gives informed consent, the first week will have four ECT sessions, then revert to the standard frequency.Anesthesia and muscle relaxation were induced using propofol (1–1.5 mg/kg) and succinylcholine chloride (0.5–1 mg/kg), with atropine administered to regulate heart rate when required.
Statistical analysesData analysis was conducted using IBM SPSS Statistics 25.0. Categorical variables were described using percentages (%), and continuous variables were represented by either Mean (SD) or Median (IQR), based on conformity with normal distribution. Comparisons between groups were made using Chi-square tests, independent samples t-tests, or Mann–Whitney U tests. The outcome, CGI-I positive or negative response, was utilized as the dependent variable, with 0 for a positive response and 1 for a negative response. Logistic regression analyses were employed to assess factors associated with ineffectiveness in ECT treatment for adolescents with severe depressive episode and suicidal behavior, calculating Odds Ratios (OR) and 95% Confidence Intervals (95% CI). Due to the absence of equivalent dose conversion formulas for duloxetine and vortioxetine, their missing values were imputed using the median fluoxetine equivalent dose.
Various models were applied:
The unadjusted model assessed four variables concerning ECT treatment and days hospitalized.
Model 1 evaluated ECT treatment and demographic factors, excluding severe side effects of ECT, and days hospitalized, and included 6 variables.
Model 2 added disease variables to Model 1, excluding the same variables as in Model 1, involving 14 variables.
Model 3 combined Models 1 and 2 with medication treatment variables, excluding mood stabilizers and those omitted in Models 1 and 2, included 20 variables.
All models classified ECT sessions instances in intervals of 4 as ordinal rank variables and encoded them as nominal categorical dummy variables to specifically study their correlation with the dependent variable (details in Table 3). Subgroup analysis divided age at the median into a dichotomous variable, and in conjunction with gender, partitioned the data into four distinct stratified subsets. Each subset was analyzed according to Model 3’s parameters to validate the result stability. Statistical findings were deemed significant with P < 0.05 (2-tailed). Regarding omitted variables, days hospitalized and severe side effects of ECT may act as mediating variables, potentially influenced by ECT sessions.
留言 (0)