
記住我
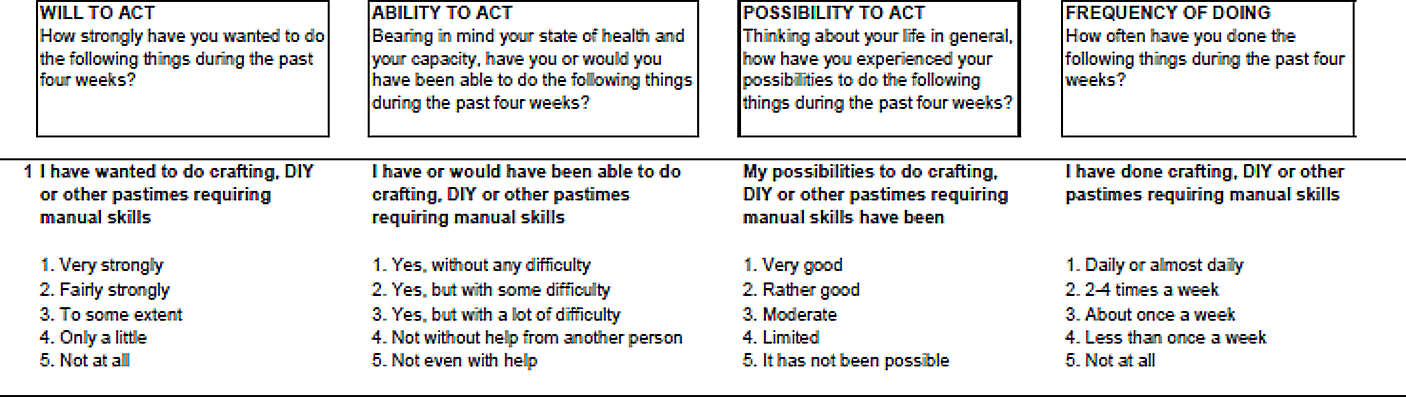




The original UJACAS comprised 17 items to be self-assessed regarding goals, ability, opportunity, and activity, operationalised as four sub-scales (see Fig. 1). The items addressed the following, with abbreviation in parenthesis: Crafting or do-it-yourself (Crafting & DIY), Artistic pursuit (Artistic pursuit), Participating in events (Events), Enjoying nature (Nature), Keeping physically fit (Physically fit), Exercising the mind (Exercise mind), Using computer or pad (Use computer/pad), Supporting or helping others (Support others), Maintaining social relationships (Social relationships), Making new acquaintances (New acquaintances), Taking responsibility in one´s own life (Promote own life), Taking responsibility for societal or communal matters (Public matters), Make one´s days interesting (Interesting days), Maintaining or improving the cosiness of one´s home (Make home cosy), Taking care of appearance (Appearance), Ensuring financial affairs are in order (Financial affairs), and Furthering matters according to faith or world view (Faith or worldview).
Fig. 1
Example from the English version of UJACAS first item (Crafting & DIY), with four subscales and response options
Using a five-point Likert scale, participants were asked to rate their answers in the light of the latest four weeks. Response options are worded to suit each item, starting with the alternative representing the highest level of active ageing, in descending order. To calculate a sum score, the response option representing the highest level are assigned 4 points, and the lowest response option is assigned 0. With 17 main items and four subscales, a total of 68 sub-questions adds up to a sum score of 0-272. A higher sum score indicates a higher level of active ageing. A maximum of two missing values are allowed for each subscale, or eight for the total sum score (Rantanen et al., 2019).
Project ContextThis study was performed in the context of the Prospective RELOC-AGE project targeting older adults aged 55 + considering relocation, with active ageing as one of the outcomes. The full scope of RELOC-AGE is available at ClinicalTrials.gov NCT04765696 and in a study protocol (Zingmark et al., 2021).
Study DesignThis study was performed in three phases with different samples. Following the translation of UJACAS from Finnish to Swedish, Phase 1 took place during September to November 2020, with a research team addressing semantic equivalence and a user panel with representatives for the target population addressing content validity. Phase 2 took place during November 2020 to January 2021. Data quality and reliability were assessed in a test-retest involving a convenience sample of people aged 55+. Phase 3 was initiated in April 2021 when the baseline started for the Prospective RELOC-AGE project (Zingmark et al., 2021). In all, the RELOC-AGE data included in this paper was collected from September 2020 until October 2021.
Participants and RecruitmentIn phase 1 the research team addressing semantic equivalence involved some of the co-authors of this paper (FN, MZ, MG, TR, and SI), representing occupational therapy as well as gerontology expertise on junior and senior levels. To assemble the user panel, we used our collected personal networks. The inclusion criteria were age 55+, interest in the concept of active ageing and related research and being a fluent Swedish speaker. Nineteen persons who we knew met these criteria were approached by email and six answered and were included. This was considered an appropriate number of participants for the selected analysis (Polit & Beck, 2006). Women represented half of the user panel (N = 3 women), and mean age was 73 years.
For phase 2, the inclusion criteria were age 55 + and a postal address in Sweden. Exclusion criteria were cognitive impairments and/or insufficient language skills to give informed consent and/or participate in telephone interviews, as assessed by first author who has 15 years of experience working with individuals with different cognitive impairments. Also, living in residential care was an exclusion criterion. Information about the study including an invitation to participate was sent to a contact person or board member of senior citizen associations. Of thirteen contacted, eight associations agreed to inform about the study through their newsletters and email communication to members. First author was contacted by 66 persons who wanted to participate, but two chose later to withdraw their participation. Another individual was excluded due to cognitive difficulties apparent during the first interview; despite the interviewer repeating both the purpose of the study and the current item question several times, concerns remained whether the respondent knew which question was being discussed. Thus, 63 persons gave their answers on both occasions, with approximately 13 days in-between. Characteristics of the phase 2 respondents collected: 2/3 were women (N = 42), mean age was 75 years (range 61–92) and almost half of the respondents (47%) had a university education of 3 years or more.
For phase 3, participants responding to the Prospective RELOC-AGE web survey were invited to additional data collection by telephone including UJACAS (Zingmark et al., 2021). In all, 1,412 individuals agreed to participate in telephone interviews. Due to administrative reasons, only 1,011 respondents could be invited. Of those, 820 (81%) participated. Half of the included respondents were women (N = 415; 50.6%), mean age was 70 years (SD = 7.6). For detailed information of the respondents of phase 3, see Table 1.
Table 1 Characteristics of respondents, study phase 3Data CollectionIn phase 1 the user panel received the UJACAS, a response envelope, and a questionnaire based on the principles of CVI as described by Polit and colleagues (2007). The user panel was instructed to read through the items and use the questionnaire to write down any comments, and to rate each item on a scale from 1 to 4. A higher rating indicated understandability and relevance. Replies were sent back within two weeks.
The respondents in phases 2 and 3 received a postal letter with the UJACAS, and information to go through it and answer as much as possible before a telephone call to register their responses. For phase 2, respondents received two copies and were instructed to throw away the filled-out UJACAS immediately after the first telephone call (T1). A second telephone call was scheduled approximately two weeks later (T2), and the respondents were asked to fill out the second copy of UJACAS the day before. All data in phase 2 were collected by the first author using the same UJACAS version as the respondents. The mean time to complete the questionnaire via telephone was 22 min (range = 9–70 min; SD = 11 min) T1, and 13 min (range = 3–55 min; SD = 8.5 min) for T2.
In phase 3, data were collected by telephone calls made by two experienced occupational therapists, one of which being the first author collecting approximately 300 of the respondents’ answers. Also, two occupational therapy program students collected 200 of the answers. Prior to data collection, all staff involved received information about the instrument and the specific item meanings, also a written summary to use as a tutorial during the telephone calls. The students were offered regular guidance to deal with any issues that might arise during the data collection. The responses to UJACAS were documented directly into a web platform set up for Prospective RELOC-AGE.
Assessing Semantic Equivalence and Content Validity (Phase 1)Semantic equivalence was assessed after a professional translation of the Finnish original instrument to English and Swedish. To compare between languages the research team as described above, were involved in discussions about the phrasing and underlying meaning of the items in an iterative process. The instrument creator (TR) had some linguistic proficiency in Swedish and contributed to the comparison between languages and clarified the underlying ideas of the UJACAS. To further assess how the phrasing was perceived by the users, a user panel was instructed to rate each item for understandability (Is the item easy or hard to understand?) and relevance (Is the item relevant to describe active ageing?), and also write down any comments they had regarding specific items and the UJACAS in its entirety. Semantic equivalence was considered established when consensus was reached, after iterative discussions that were documented and analysed consecutively.
Based on the user panel ratings, content validity was evaluated using content validity index (CVI) for both individual items and total scale (Polit & Beck, 2006; Polit et al., 2007). For individual items a sum score of the ratings divided by the number of raters generated a mean score. Based on the mean score of items, scale CVI Average was calculated for the total scale. A higher CVI value indicated a higher rating of content validity. Responses in the comment fields were sorted by similarities and differences and used for fine-tuning of the phrasing of the individual items.
Data Analyses Concerning Data Quality, Floor and Ceiling Effects, Test-Retest Reliability, Internal Consistency and Construct Validity (Phase 2 and 3)Imputation for missing answers in the UJACAS was applied using the following formula: (sum score / sub-questions responded to) × sub-questions offered (Rantanen et al., 2019). Floor and ceiling effects were described on the subscale and total score levels using cut off vales 15–20% as described by Hobart and Cano (2009).
The test–retest reliability of the subscales and total scale was assessed using the intraclass correlation coefficient (ICC) (Koo & Li, 2016). Based on the 95% confident interval, ICC values were interpreted as poor (< 0.5), moderate (between 0.5 and 0.75), good (0.75–0.90), and excellent (> 0.90). ICC estimates and their 95% confidence intervals were calculated based on a single rater, absolute-agreement, 2-way mixed-effects model.
Internal consistency reliability was assessed using Cronbach’s alpha, interpreting values > 0.70 and corrected total-item correlation of the sub-questions > 0.3 (Hobart & Cano, 2009; Streiner et al., 2015) as acceptable. The standard error of measurement (SEM) was calculated and complemented with a 95% confidence interval (Hobart & Cano, 2009).
To evaluate convergent and discriminant aspects of construct validity, three hypotheses were pre-defined based on previous research (Baker et al., 2003; Bombak, 2013; Rantanen et al., 2019, 2021) and clinical reasoning. Addressing convergent validity, Pearson correlation was used (Streiner et al., 2015). We hypothesized that a higher level of active ageing was expected to correlate significantly with: (1) Self-Rated Health assessed with the 1-item question from the SF-12 scale (Jenkinson et al., 1997), “In general, would you say your health is…” (5 response options ranging from poor to excellent). (2) Life-Space Mobility Assessment, Swedish version (Fristedt et al., 2016) questions 4 and 5, whether respondents during the previous 4 weeks had been outside their neighbourhood, town, or beyond town. For each level, respondents indicated how often (< once per week; 1 to 3 times per week; 4 to 6 times per week; every day), and whether they needed a technical device/assistance (sum score = (4 × LS4 score) + (5 × LS5 score), ranging from 0 to 36). Higher scores indicated greater life-space mobility. Correlation values were considered as weak between 0.1 and 0.3; moderate between 0.4 and 0.6); strong between 0.7 and 0.9 and perfect at 1.0 (Akoglu, 2018). Addressing discriminant validity, Mann Whitney U test was used to differentiate UJACAS sum scores between persons who have had been diagnosed with clinical depression and those who had not, assessed with the question “Have you been diagnosed with clinical depression”, (Yes, during the last 12 months; Yes, but not during the last 12 months; No, never). As the risk of relapse of depression is high (Burcusa & Iacono, 2007; Luijendijk et al., 2008).
two groups were created, those who answered they had had depression at any point, and those who answered they had not. We hypothesized that a lower level of active ageing was expected among persons that had previously been diagnosed with clinical depression.
P-values < 0.05 were considered statistically significant. All statistical analyses were computed using IBM SPSS statistical package version 27.
Table 2 Analyses in the three study phases
留言 (0)