
記住我


A key hallmark of cancer is the ability to sustain unlimited cell division—a trait in which telomeres play a pivotal role.1 Located at the chromosomal termini, telomeres are composed of approximately 5–10 kilobases of repetitive, G-rich, DNA bound by the shelterin protein complex, thereby functioning to stabilise and protect the ends of the chromosomes.2 During cell division, telomeric DNA is progressively lost predominantly due to the inability of DNA polymerase to fully replicate the ends of linear DNA (ie, the end-replication problem).3 In normal cells with intact cell cycle checkpoints, moderate telomere loss results in either cellular senescence or apoptosis. In contrast, incipient cancer cells commonly bypass these checkpoints, leading to critical telomere shortening which, in turn, instigates cancer-promoting chromosomal instability.4 In order to continue to proliferate, most cancers maintain their telomeres via the telomere synthetic enzyme telomerase, the expression of which is normally stringently repressed in somatic cells. However, a subset of cancers lacking telomerase maintain their telomeres by engaging the alternative lengthening of telomeres (ALT) pathway.
First discovered in yeast, where rare colonies survived deletion of the yeast telomerase gene by using homologous recombination (HR) to maintain their telomeres,5 ALT is now an established telomere maintenance mechanism in human cancers.6 ALT is maintained through a homology-directed DNA repair mechanism.7 Similar to break-induced replication (BIR), this aberrant process results in dramatic cell-to-cell telomere length heterogeneity and rampant chromosomal instability.8 ALT has been reported to be present in 5%–10% of all cancers found throughout the body.9 While ALT can infrequently arise in carcinomas, ALT is particularly enriched in cancers with a neuroepithelial or mesenchymal origin.9 10 Genetic alterations in chromatin remodelling proteins, notably in the ATRX/DAXX histone chaperone complex that deposits H3.3, have emerged as a distinctive characteristic of human ALT-positive cancers.11–14 These loss-of-function mutations usually lead to loss of nuclear protein expression; thus, immunohistochemistry has been used clinically as a surrogate for the presence of inactivating mutations in multiple tumour types.11 15 While the vast majority of ALT-positive cancers and cell lines have lost either functional ATRX or DAXX predominantly through missense or truncating mutations,13 inactivating mutations in H3F3A, SMARCAL1 and SLX4IP have been uncovered.16–18 In addition to its essential role in maintaining cancer cell telomeres, ALT has prognostic value in certain cancer types and may be a potential target for anti-cancer therapies. Here, we discuss the underlying molecular mechanism of ALT and how identifying and/or targeting the ALT pathway may be useful in the clinic.
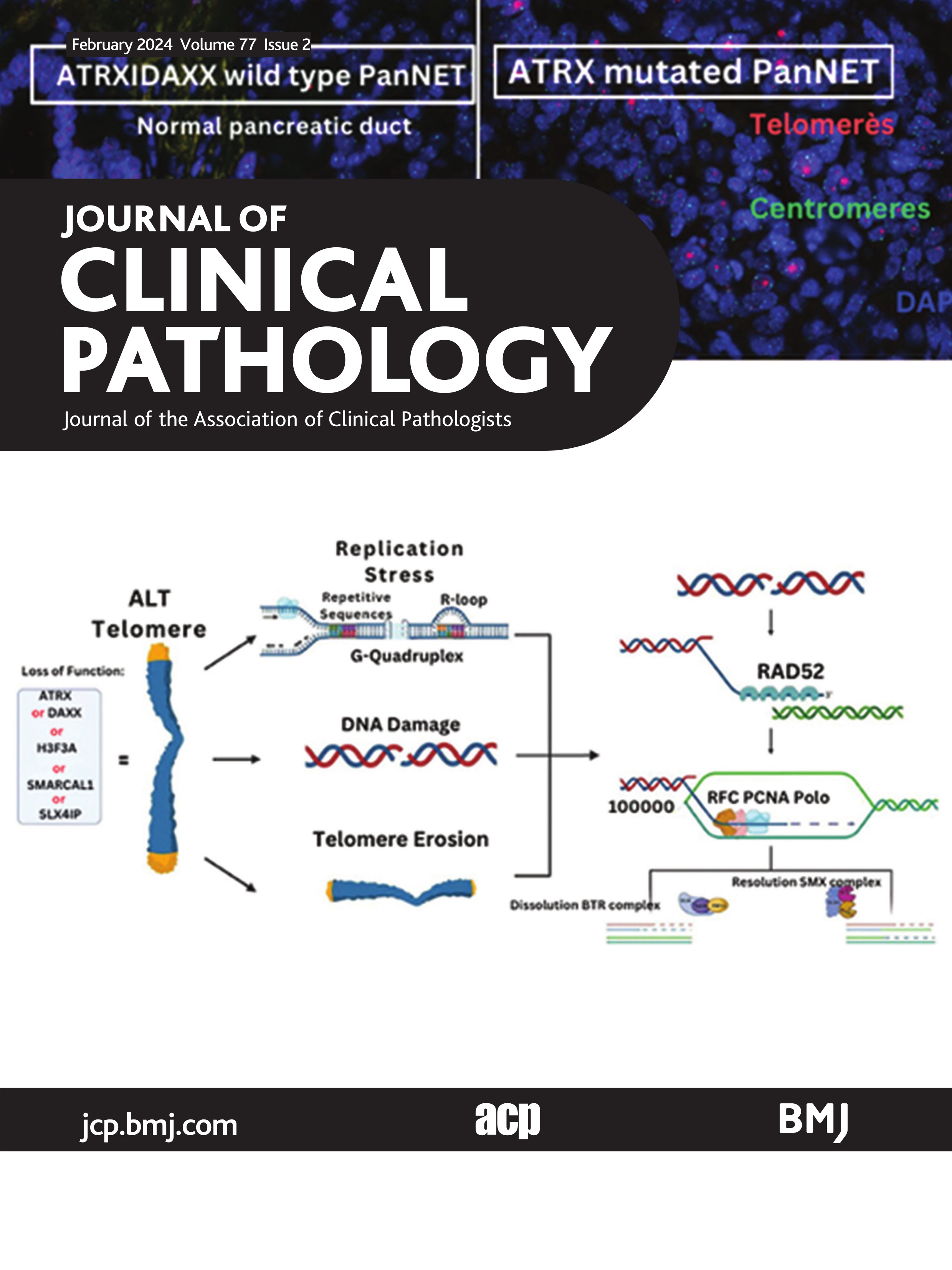
ALT mechanismThe ALT pathway co-opts DNA damage repair through HR to promote telomere elongation. As highlighted in figure 1A, it has been proposed that telomere elongation during ALT is triggered by spontaneous double-stranded DNA (dsDNA) damage, chronic replication stress and/or simple telomere erosion.19 20 Replication stress at the telomere is caused by a variety of physical impediments to the DNA polymerase including repetitive DNA sequences, G-quadruplexes and RNA–DNA hybrids.21 In addition, replication stress is exacerbated at ALT as a result of mutations in chromatin remodelling enzymes and DNA damage repair factors (ATRX, DAXX, SMARCAL1, SLX4IP) that lead to aberrant telomeric chromatin structure and altered DNA damage repair kinetics.11 12
 Figure 1
Figure 1 Break-induced replication mediates the extension of ALT telomeres. (A) Functional loss of either ATRX, DAXX, H3F3A, SMARCAL1 or SLX4IP is common in ALT-positive cancers. In the absence of telomerase, ALT extension is stimulated by either spontaneous double-stranded DNA (dsDNA) damage, chronic replication stress or telomere erosion. The unresolved replication stress or telomere erosion can devolve into dsDNA damage. (B) These dsDNA gaps are processed by nucleases to generate a 3′ single-stranded DNA (ssDNA) overhang. RAD52 will bind to the 3′ ssDNA and facilitate a homology search with other telomeric sequences. Binding of the 3′ ssDNA to homologous telomeric DNA will generate a D-loop structure. This D-loop structure will recruit the break-induced replication (BIR) replisome which consists of PCNA–RFC–Polδ. Following Polδ-mediated extension, the D-loop intermediate structure is processed by either the dissolution or resolution pathways. Dissolution produces telomere extension, a lack of cross-over events, and is mediated by the BTR complex. Resolution does not produce telomere extension, may lead to cross-over events (ie, only cross-over events displayed here), and is mediated by the SMX complex. Created with BioRender.com. ALT, alternative lengthening of telomeres.
Irreversibly stalled replication forks are enzymatically cleaved generating one-ended double-stranded DNA breaks (DSBs). These DSBs can then trigger repair via a type of HR described as BIR.22 The BIR pathway that occurs at ALT is thought to vary from canonical BIR in that ALT BIR relies on the recombinase RAD52, whereas canonical BIR relies on the RAD51 recombinase.23 RAD52 has been shown to bind to resected 3′ single-stranded DNA (ssDNA) overhang and to stabilise this HR intermediate structure.24 As shown in figure 1B, the RAD52 bound 3′ telomeric overhang facilitates annealing to a homologous telomeric sequence and generates a local displacement loop (D-loop). This D-loop structure facilitates the assembly of the BIR-associated replisome that at its core includes PCNA–RFC–Polδ where the PolD3 subunit of Polδ is necessary for ALT BIR-mediated telomere extension.25 Following Polδ-mediated extension, the D-loop structure is processed either through dissolution or resolution. Dissolution is mediated by the BLM helicase, which acts as a scaffold for the assembly of topoisomerase IIIα (Top3A) and RMI1/2 and leads to the formation of the BTR complex. Dissolution by the BTR complex leads to telomere extension without crossover events. In contrast, resolution is mediated by SLX4 which acts as a scaffold for the SLX1 and MUS81 nucleases creating the SMX complex. Resolution by the SMX complex can promote crossover events even in the absence of telomere elongation.26 Together, ALT BIR can not only promote telomere elongation but also recombination.25
ALT detection and prevalence in cancerClinically, the presence of ALT can be detected in tissue through a number of different assays. Notably, these assays assess ALT-specific molecular characteristics, including the presence of striking cell-to-cell telomere length heterogeneity and large ultrabright nuclear foci of telomeric FISH signals marking ALT-associated telomeric DNA in interphase nuclei. One highly sensitive and specific assay for detecting ALT in archival tissue specimens is the telomere-specific FISH assay.27 As shown in figure 2, ALT-positive cases can be identified by the presence of large, ultrabright intranuclear telomeric foci that can often co-localise with PML to form so-called ALT-associated PML bodies, as well as revealing dramatic heterogeneity in telomere lengths. Conversely, ALT can be identified by detecting partially single-stranded telomeric DNA circles (C-circles) that are byproducts of aberrant DNA damage repair processes.28 29 However, this assay is relatively labour intensive, and in contrast to the telomere-specific FISH assay, the tissue architecture is not preserved.
 Figure 2
Figure 2 Telomere-specific FISH demonstrating ALT-negative and ALT-positive PanNETs. Left panel: representative example of a PanNET that is wild type for ATRX and DAXX and ALT-negative. Right panel: representative example of a PanNET that contains an inactivating ATRX mutation and is ALT-positive. The distinctive large, ultrabright intranuclear foci of telomere FISH signals (red) mark the ALT-associated telomeric foci. A defining feature of ALT is the presence of these ALT-associated telomeric foci in ≥1% of the cancer cells. A pan centromere-specific FISH probe (green) is included as a hybridisation control. Original magnification×400. ALT, alternative lengthening of telomeres; PanNETs, pancreatic neuroendocrine tumours.
Using these assays, ALT has been identified in 5%–10% of all cancers. However, as shown in table 1 which is adapted and updated from MacKenzie and colleagues,10 ALT is greatly enriched in certain cancer types, including complex karyotype sarcomas (eg, leiomyosarcoma, osteosarcoma, liposarcoma, liposarcoma, undifferentiated sarcoma) and central nervous system tumours (isocitrate dehydrogenase (IDH)-mutant astrocytoma). While many cancer types display ALT at a low frequency (<1%),9 other specific cancer types that are enriched for ALT, include pancreatic neuroendocrine tumours (PanNETs), neuroblastoma and chromophobe hepatocellular carcinoma (HCC).30–33 Known and validated gene mutations associated with ALT in human cancers (ATRX, DAXX, SMARCAL1 and SLX4IP) are virtually mutually exclusive with alterations known to reactivate telomerase, including activating TERT promoter mutations (C228T and C250T) and TERT gene rearrangements.34 Interestingly, there are certain cancer types that appear not to use the ALT pathway for telomere maintenance. For example, primary adenocarcinomas of the prostate, pancreas and lung are always ALT-negative,9 thereby suggesting these cell types either cannot tolerate the presence of an ALT-associated mutation, or at least these mutations and subsequent ALT activation does not promote a growth advantage in the cancer cells. In summary, while the prevalence varies widely, ALT is the predominant telomere maintenance mechanism in specific cancer types and in some cases presents with distinctive morphological features (eg, chromophobe HCC).32 33
Table 1Representative cancer types enriched for the ALT pathway
ALT as a diagnostic and/or prognostic biomarker in cancerWhile cancer type-dependent and context-dependent, ALT-positive cancers are challenging to treat because these cancers generally portend a poor clinical prognosis, and unfortunately occur in cancer types that currently lack targeted therapies. While ALT-positive cancers present with a lower tumour burden, these cancers are associated with rampant chromosomal instability. Interestingly, a molecular progression model for PanNETs has been proposed in which mutations in ATRX or DAXX occur first, followed by ALT activation and CENP-A mislocalisation at centromeric sites, thereby leading to non-random chromosome mis-segregation and complex karyotypes. Whether this phenomenon is conserved in other ALT-positive cancers remains unanswered.35
ALT status can potentially serve as a diagnostic and/or prognostic marker, helping clinicians’ diagnosis and ultimately predict the behaviour and aggressiveness of certain cancers to help guide decision-making regarding treatment options. For example, the presence of ALT (or ATRX/DAXX protein loss by immunohistochemistry) is highly specific to PanNETs compared with pancreatic neuroendocrine carcinomas (PanNECs) and other neuroendocrine tumours found throughout the body. Thus, ALT status may provide diagnostic information to help distinguish between PanNETs and PanNECs, as well as determine pancreatic origin for metastatic neuroendocrine tumours in the setting of an unknown primary.15 30 Likewise, ATRX protein loss is used clinically to diagnose common tumour entities of the central nervous system, in particular IDH-mutant astrocytoma.36 In these tumour types, ATRX protein loss strongly correlates with the presence of ALT; thus, ALT may serve as a potential diagnostic marker in this setting.
As a prognostic marker, the presence of ALT has been identified and independently validated as a robust prognostic biomarker in large cohorts of primary PanNETs.37–40 In a recent international cohort study of 561 patients with a non-syndromic, non-functional PanNET without distant metastases at surgical resection, ALT was an independent prognostic biomarker for worse recurrence-free survival.30 Likewise, in terms of prognostication in adult diffuse gliomas, ATRX mutations (and ALT activation) are almost exclusively present in IDH-mutant astrocytoma (often co-occurring with TP53 mutations). This subgroup has an intermediate prognosis; a better prognosis when compared with oligodendrogliomas that are IDH-mutant and 1 p/19q co-deleted (TERT promoter mutated/ATRX wild type), but a worse prognosis when compared with IDH-wildtype glioblastoma (TERT promoter mutated/ATRX wild type).41 Similarly, a systematic review of eight studies consisting of 551 patients (226 ALT-positive) with a diverse group of sarcomas showed that ALT is independently associated with an increased risk of death, even after adjusting for potential confounding variables.42 In contrast, chromophobe HCC is greatly enriched for ALT (87%–92%), but displayed a similar overall and recurrence-free outcome compared with conventional HCC (2.2%).32 Thus, in certain cancer types, ALT is a strong prognostic marker (eg, PanNETs and sarcomas), although context matters (eg, different molecular and/or morphological subtypes). These data support the notion that ALT should be considered for a precise prognostic stratification and design of potential therapeutic strategies. Incorporating ALT into routine clinical flow is feasible and inexpensive, particularly with new technological developments.15 43
Therapeutically targeting the ALT pathwayCurrently, there are no clinical trials that specifically target ALT limiting treatment options for patients with ALT-positive cancers. Targeting members of the BIR pathway has been an attractive approach to therapeutic development (figure 3A). Given the importance of RAD52 in BIR at ALT, inhibition of RAD52 would appear to be an ideal candidate. RAD52 knockout mice are viable and have no age-associated defects suggesting that inhibition of RAD52 would have limited off-target effects in normal cells.44 However, inhibition of RAD52 may promote compensation by RAD51-mediated BIR.22 BIR can stimulate telomere extension events via the Polδ polymerase however, Polδ is essential for lagging strand synthesis during DNA replication. As a result, inhibition of this subunit would likely present with widespread off-target effects.45 However, recent studies have demonstrated that the FANCM helicase interacts with the BTR complex and functions to stimulate BIR-mediated telomere extension events by the PCNA–RFC–Polδ core complex.20 46 Moreover, disruption of the FANCM–BTR interaction or loss of FANCM function induces cytotoxicity exclusively in ALT cancer cells. Thus, the development of small molecule inhibitors of FANCM may provide an opportunity to specifically target the ALT pathway (figure 3A).
 Figure 3
Figure 3 ALT-specific therapeutic targets. (A) The ALT-mediated BIR pathway may be targeted through inhibition of the recombinase RAD52, thereby preventing the homology search necessary for telomeric extension. Co-inhibition of the canonical HR recombinase RAD51 is proposed to prevent compensatory mechanisms. In addition, the helicase FANCM interacts with the BTR complex to drive ALT extension. Disruption of the FANCM–BTR interaction and/or inhibition of FANCM has been shown to induce ALT-specific cytotoxicity. (B) ALT cancers have a high prevalence of functional mutations in either the ATRX or DAXX gene. Therefore, synthetic lethality of ALT cancer cells may occur by inhibiting compensatory pathways like ABL1/c-JUN (ie, ponatinib), ATR, WEE1 or SMARCAL1. Created with BioRender.com. ALT, alternative lengthening of telomeres; BIR, break-induced replication; HR, homologous recombination.
Given the prevalence of mutations in ATRX or DAXX in ALT-positive cancers, the identification of synthetic lethal vulnerabilities may provide an opportunity to target ALT (figure 3B). In fact, a recent study identified the small molecule inhibitor ponatinib as a candidate for ALT synthetic lethality.47 Ponatinib is a receptor tyrosine kinase inhibitor (RTKI) that was suggested to modulate the ABL1/c-JUN signalling axis exacerbating replication stress in ATRX-deficient ALT-positive cells. As a result, treatment with Ponatinib reduces ALT cell viability. Likewise, ATRX-deficient ALT-positive cells were sensitive to loss of the replication stress kinase ATR, the checkpoint kinase WEE1 and the DNA damage repair enzyme SMARCAL1. Depletion of either ATR, WEE1 or SMARCAL1 had little effect on the viability of non-ALT cells, but led to a decrease in viability in ALT-positive cancer cells.48–50 In addition, the efficacy of ATR inhibitors as a monotherapy or in combination therapy is currently being tested in patients with defined loss-of-function mutations in ATRX or DAXX (eg, NCT04170153, NCT05687136). These enzymes represent the most recent targets considered within the ALT pathway. However, expanding this list of candidate targets will require a deeper understanding of the aetiology of the ALT pathway in cancer.
Conclusions and significanceA substantial number of human cancers engage the telomerase-independent ALT pathway to promote telomere elongation by co-opting DNA damage repair via HR. ALT-positive cancers, although cancer type-dependent and context-dependent, tend to have poor outcomes. Taken together, ALT is strongly enriched in certain cancer types, associated with specific loss-of-function somatic mutations and can be readily identified in clinical specimens. In addition to its prognostic utility, ALT may represent a tractable therapeutic target and new approaches are rapidly being developed.
Ethics statementsPatient consent for publicationEthics approvalNot applicable.
留言 (0)