
記住我






Exercise for people living with and beyond cancer is recommended by the American College of Sports Medicine, American Society of Clinical Oncology,1 and American Cancer Society2 to manage the side effects of treatment and improve overall health. However, there are a lack of effective strategies to translate these recommendations into clinical practice and implement physical activity and exercise programming for people living with and beyond cancer.3 Barriers to engaging in exercise for people with a cancer diagnosis include common side effects of treatment, such as fatigue and uncertainty about safety.
Among individuals previously diagnosed with cancer, including women with ovarian cancer, it is frequently observed that they do not meet the recommended levels of physical activity.4,5 Compared with more common types of cancer such as breast cancer, there is limited research on exercise as part of supportive care for women living with and beyond ovarian cancer,6,7 yet these women report wanting information and access to exercise programming.5
Observational data also suggest that women living with and beyond ovarian cancer are at a higher risk of falls.8 In population-level data from a province in Canada, women with a prior diagnosis of ovarian cancer were more likely to have been admitted to the hospital at least once for a fall compared with age-matched controls who underwent other types of gynecological surgery (eg, hysterectomy), which strongly suggests these falls are driven by factors other than age or menopausal status.8 In older adults, exercise programs focused on fall prevention have been shown to reduce the risk of falls by 17% to 35%.9,10 However, the potential of tailored exercise programming to reduce the risk of falls for women living with and beyond ovarian cancer has not been explored to date. Developing feasible, accessible, and cost-effective supportive care programming to improve overall physical function and quality of life, as well as reduce fall risk for women living with and beyond ovarian cancer is an emerging research priority. Furthermore, virtual delivery of group-based supervised exercise could increase the reach of programming by reducing barriers that have been reported with in-person programming, such as living too far from available programs, lack of transportation options, lack of access to appropriate exercise facilities,11 and discomfort crowded environments, such as a public exercise facility.12 The purpose of this study was to assess the feasibility of a virtually delivered, group-based, supervised exercise program for women living with and beyond ovarian cancer to inform the implementation of exercise programming as part of supportive cancer care.
METHODS Trial DesignParticipants completed an individual in-person assessment at baseline, at the midpoint of the program (6 weeks) and at the end of the program (12 weeks) to collect physical outcome measures. Participants also completed questionnaires electronically using REDCap database (Vanderbilt, USA) (or a paper version) at the time of each physical assessment, as well as 12 weeks after program completion (24 weeks postbaseline).
ParticipantsParticipants were recruited through medical oncologists and nurse practitioners at BC Cancer Vancouver and BC Cancer Surrey, or self-referral in response to study recruitment advertising (eg, flyers, social media posts, laboratory Web site). Individuals were eligible if they met the following criteria: female; between 40 and 75 years; within 1 year of completion of primary chemotherapy treatment (oral or maintenance therapy) for ovarian cancer without known recurrence; had not experienced 2 or more falls in the prior 6 months; had access to a smartphone, tablet, laptop, or desktop computer with a camera and microphone; had access to a reliable Internet connection; and were able to read and speak English. Baseline physical activity levels were not an exclusion criteria. Interested individuals underwent eligibility screening by phone with a study team member. After obtaining informed consent, participants were booked for a baseline assessment.
InterventionThe BE-BALANCED program was a 12-week group-based virtual program comprised 75-minute supervised exercise sessions (up to 60 minutes of supervised exercise and 15 minutes of education) (see Supplemental Digital Content Appendix 1, available at: https://links.lww.com/REHABONC/A63 which demonstrates BE-BALANCED program). Sessions were delivered twice weekly by a clinical exercise physiologist with training in exercise oncology. In addition to the exercise sessions, participants were encouraged to attend 2 optional nutrition education sessions focused on healthy eating, facilitated virtually by a registered dietitian specializing in cancer care.
At the in-person baseline assessment, all participants were provided 3 Therabands (green, red, and blue) and a workbook that included the exercise program, worksheets for education topics and healthy eating information, and a weekly diary for capturing falls and independent exercise. Participants requesting assistance with using live, 2-way videoconferencing were provided a short tutorial by the research team at the baseline assessment, with the option of a practice session in advance of the program. All exercise sessions were delivered virtually using Zoom (San Jose, California). Each exercise session included a 10-minute warm-up (eg, marching, active range of motion movements) followed by a circuit incorporating aerobic movements (eg, high knees, stepping patterns) and full-body resistance exercises using body weight and/or Therabands (eg, bodyweight squats, banded chest press, banded reverse fly) along with balance exercises (eg, 1 leg balance, tandem stances). The exercise prescription for the circuit progressed from 2 sets (18 minutes) of moderate intensity (rate of perceived exertion [RPE] as 10-12) to 3 sets (30 minutes) of moderate to vigorous intensity (RPE as 13-15) by week 12. Following a 5-minute cooldown, core strength exercises, and full-body static stretching were incorporated. Individualized exercise modifications and progressions were provided as required to accommodate participants and aide them in reaching their target RPE. To assess if participants were meeting the exercise intensity goal of the session, participants were shown the RPE scale immediately after the circuit and directed to send their RPEs to the instructor privately in the chat function of Zoom to remove influence from other participants. For independent exercise starting in week 4, participants were asked to complete a minimum of 30 minutes of exercise, while maintaining a RPE within a range of 11 to 14. Successful attainment of both time and intensity goal was necessary to be counted as adherence for each session.
The education component included instruction on reflective (eg, benefits of physical activity) and self-regulatory processes (ie, goal setting, self-monitoring, action planning, overcoming barriers) from the multi-process action control framework13,14 to assist in the long-term adoption of positive exercise behavior. Reflective and regulatory strategies are a significant predictor of physical activity adoption and action control, respectively.14 Each week the instructor facilitated a 15-minute group discussion in advance of the exercise program. The topics included: (1) introduction to the program, (2) fall safety during exercise, (3) benefits of exercise for survivors of cancer, (4) importance of balance training, (5) self-monitoring intensity, (6) goal setting, (7) action planning, (8) overcoming barriers, (9) healthy eating for exercise, (10) exercise after the program, and (11) community resources. Finally, the Zoom meeting link was opened 15 minutes before the start of class and participants were encouraged to join for an informal social check-in to foster connections with peers and develop group dynamics, which historically are an important element of in-person programming.15
In addition to the supervised virtual exercise sessions, participants were asked to complete 1 session per week of the BE-BALANCED exercise program independently, starting in week 4. Instructions for independent exercises were included in the workbook along with links to prerecorded exercise videos created by the instructor. Participants were asked to record independent exercise sessions in an exercise log and submit weekly via e-mail for review by study staff. After the BE-BALANCED program was completed, participants were encouraged to continue exercising in a self-directed manner.
The primary focus of the optional nutritional sessions was to educate participants on healthy eating habits, with an emphasis on adopting a whole food, plant-based diet. Key elements included promoting the consumption of vegetables, fruits, whole grains, legumes, lentils, nuts, and seeds, along with foods rich in essential nutrients necessary for muscle function, strength, and optimal bone mass (eg, plant-based protein, calcium, vitamin D). In the first 60-minute session (week 3), the dietitian reviewed healthy eating habits and resource materials provided in the workbook; the second 60-minute session (week 8) served as a check-in to address participant questions and share recipes. The resource materials were shared with participants regardless of whether they attended the sessions.
Primary OutcomesThe primary outcome was the feasibility and evaluated using specific a priori targets for accrual (100% of recruitment target); attendance (>70% of sessions attended out of 24 total supervised group exercise sessions); adherence (met exercise target >70% of supervised group exercise session); adherence to independent exercise session (met exercise target >70%); attrition (<30% withdrawal), safety (no serious adverse events related to the intervention), and fidelity of group belonging (score of >15 in a standardized questionnaire16). Adherence for both the supervised and independent sessions was assessed separately by the percentage of sessions in which participants achieved the target exercise intensity (measured by self-reported RPE).
Secondary OutcomesSecondary outcomes were assessed at baseline, the midpoint (6 weeks), end of the program (12 weeks), and follow-up (24 weeks; patient reported outcomes only). Objective assessments were collected at in-person visits to evaluate the preliminary efficacy of the BE-BALANCED program. Participants completed the Functional Reach Test,17 Short Physical Performance Battery (SPPB),18 and elements of the Senior Fitness Test19: 8-foot Timed Up and Go test20; 30-second bicep curls; and 6-Minute Walk Test (6MWT).21,22 Anthropometrics included body mass index (kg/m2) and both waist and hip circumferences (cm). The in-person objective assessments were not repeated at 24 weeks to reduce the patient burden of another in-person visit. Health-related quality of life was assessed using RAND Short Form Health Survey (SF-36).23 Depression and anxiety were assessed using the Hospital Anxiety and Depression Scale.24 Usual physical activity was assessed using the Godin Leisure Time and Exercise Questionnaire (modified GLTEQ).25 Dietary intake was assessed using the 26-item Dietary Screening Questionnaire.26 In addition, each week, participants were asked to complete a falls diary to capture whether they experienced any falls,27 and this was collected weekly by the research team.
Tertiary OutcomesParticipant satisfaction was assessed using a satisfaction questionnaire and a purposive sample of participants also completed an optional semistructured interview, conducted by a team member not involved in the program. Participants rated their satisfaction with intervention components, including the ease of accessing the virtual sessions, comfort and confidence with technology, and the behavioral regulation strategies provided to increase motivation to exercise28,29 to gain additional insights to refine the intervention for future delivery.
Sample SizeThe planned sample size of 30 participants was based on previous research on feasibility and pilot studies that suggested that the optimal sample size to evaluate a primary aim of feasibility ranges from 24 to 30 participants.23,25,30,31 To achieve this sample size, we planned to run 3 to 5 pilot groups with 6 to 10 participants per group.
Statistical AnalysesAssumptions of normality and equal variance required for a parametric test were tested for all variables. For variables that did not meet these assumptions, the data were transformed into logarithmic and squared variables to check if the distribution would change. As no such difference was found for change over time (baseline, 6 and 12 weeks), nonparametric Friedman's analysis of variance (ANOVA) test was used to assess the differences in both objective and patient-reported outcomes across time points. As appropriate, post hoc tests were performed using the “Related Samples” option in SPSS Statistics (IBM, Armonk; version 28), followed by the “All Pairwise” comparison method for related samples and Friedman's 2-way ANOVA by rank. Effect size was calculated as Kendall's W value. Furthermore, a Wilcoxon signed rank test was conducted to compare patient-reported outcomes at 12 and 24 weeks to determine if the implementation of the BE-BALANCED program, which encourages participants to continue exercising in a self-directed manner after the intervention, maintained self-reported physical activity levels. Finally, difference in estimated daily intake over time was calculated for each participant for fruits, vegetables, dairy, calcium, added sugars, whole grains, and fiber, and Wilcoxon signed rank test was used to determine the median estimated change in intake. The significance level was set at P < .05 for all tests.
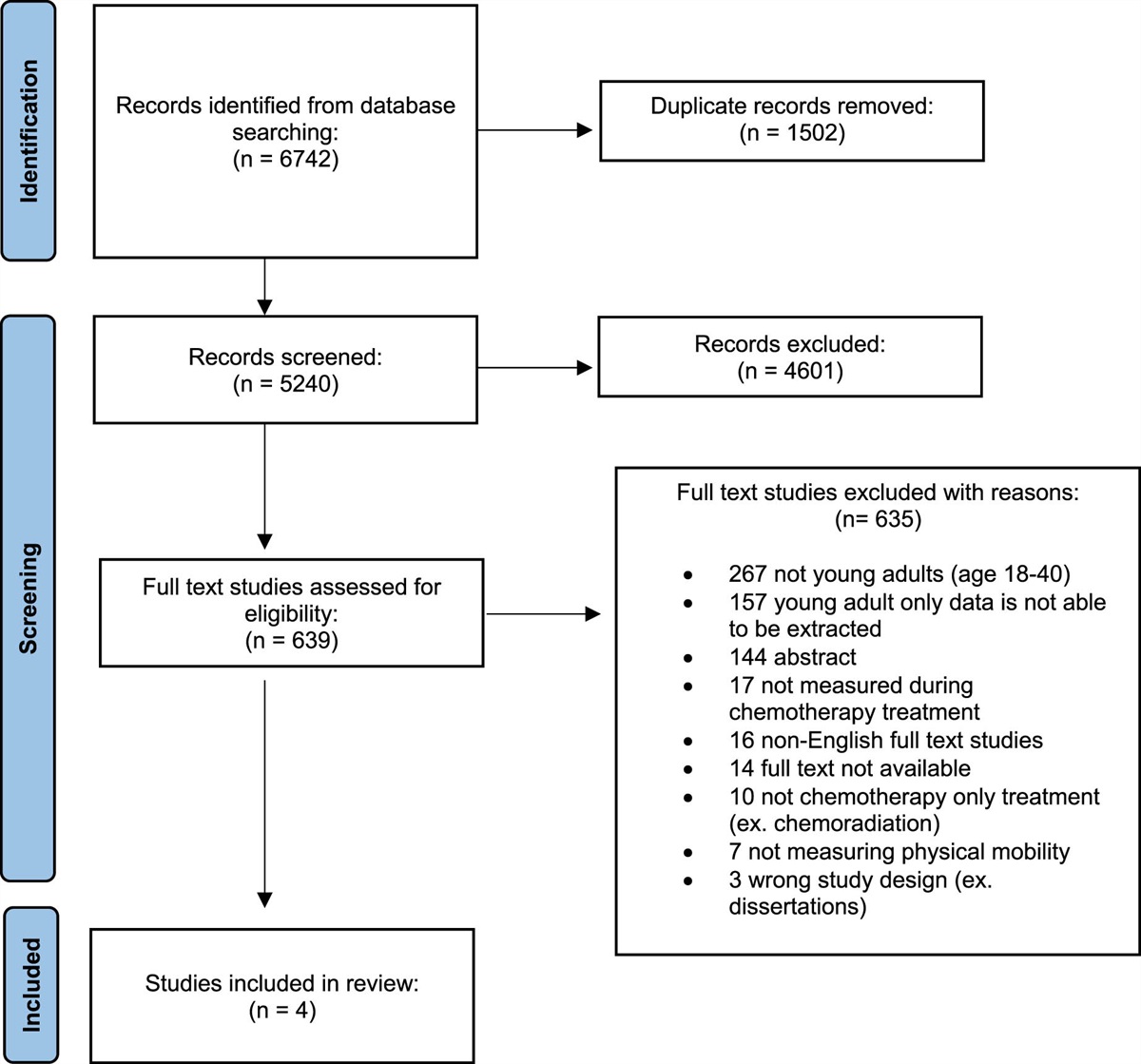
RESULTSOf the 44 individuals referred to the BE-BALANCED program, 40 were screened, 16 were eligible, and 14 enrolled in the program (Figure). The mean age was 59 ± 8 years, with a range of 45 to 71 years (Table 1). Most participants were White (55%), had completed at least some postsecondary education (90%), and were married (82%). Employment status was varied, with 45% working (part or full time), 27% retired, 18% unemployed, and 9% on sick leave/disability. All participants had received surgery and chemotherapy.
 Fig.:
Fig.: Consort flow diagram showing the progress of participants through the study.
TABLE 1 - Participant Characteristics of Participants Who Completed the Intervention (N = 11)a Characteristic Number of Participants Percentage of Participants Age (y) 40-49 1 9 50-59 5 45 60-69 4 36 >70 1 9 Cultural and racial backgrounds Chinese (eg, Chinese, Taiwanese) 2 18 South Asian (eg, Bangladeshi, Punjabi, Sri Lankan) 3 27 White (Caucasian) 6 55 Highest education Some college 1 9 Bachelor's degree 5 45 Master's or higher 5 45 Employment status Working full time 1 9 Working part time 2 18 Self-employed 2 18 Unemployed 2 18 Sick leave/long-term disability 1 9 Retired 3 27 Marital status Married or common law 9 82 Separated or divorced 2 18 Stage of cancer diagnosis Stage I 1 9 Stage II 3 27 Stage III 3 27 Stage IV 3 27 Do not know 1 9 Ovarian cancer treatments Surgery 11 100 Radiation therapy 1 9 Chemotherapy 11 100aIn some cases, not exactly 100% due to rounding.
The feasibility goal was not met for recruitment (100%). Only 14 participants enrolled in the study, representing 47% of the accrual target, during the 20-month duration of the study. The feasibility goal for attrition was met (<30%); 3 individuals dropped out of the intervention, for a 21% rate of attrition. One withdrawal was due to a recurrence, while no reason was provided for the other 2. The feasibility goals were also met (>70%) for attendance to the supervised virtual group exercise sessions (mean = 84% ± 19%; range 39%-96%) and adherence to the exercise prescription in the supervised virtual group exercise sessions (mean = 78% ± 19%; range 39%-96%), along with fidelity of group belonging (>15) (mean = 18% ± 4%; range 5%-20%). Reasons for missed supervised virtual exercise sessions or missed exercise prescription target are provided in Table 2.
TABLE 2 - Reasons for Missed Attendance and Exercise Adherence Attendance Reasons Missed Session Number of Sessions (Percentage of Missed Sessions) Number of Participants Cancer treatment- related side effects 5 (10) 2 Conflicting appointments 11 (22) 7 Emotional reasons 15 (29) 4 Family obligations 2 (4) 2 Illness unrelated to treatment 8 (16) 4 Injury unrelated to treatment 2 (4) 2 Other 2 (4) 2 Technology 1 (2) 1 (<1%) Travel 4 (8) 1 Work 1 (2) 1 Exercise Adherence Reasons Missed Target RPE Number of Sessions (Percentage of Missed Sessions) Number of Participants Emotional reasons 1 (6) 2 Exercise class was too easy 5 (29) 2 Fatigue 1 (6) 1 Illness unrelated to treatment 1 (6) 1 Injury unrelated to treatment 1 (6) 1 Intensity intentionally lower by instructor 3 (18) 2 Left early (conflicting appointments) 3 (18) 3 Other reasons 2 (12) 2Abbreviation: RPE, rate of perceived exertion.
The most common reasons for participants missing sessions (attendance) were: emotional reasons (29%), conflicting appointments (22%), and nontreatment-related illness or injury (16%) (Table 2). The 15 sessions missed due to emotional concerns were reported by 4 individuals; 3 of whom withdrew from the study, following missed sessions, and 1 refrained from further participation in the exercise program following missed sessions, citing feeling overwhelmed and self-conscious on camera, but still completed end of study assessments. In terms of exercise adherence, the primary reasons for missing the targeted intensity were: “Exercise class was too easy” (29%), “intensity intentionally lowered by instructor” (18%), and “left early due to conflicting appointment” (18%). Two participants found 1 or more of the exercise sessions too easy and for 2 participants the intensity was purposefully lowered by the instructor for 1 or more sessions for a total of 3 sessions with a prescribed reduction.
For independent exercise, the feasibility goal (>70%) was not met with the mean adherence of 57% ± 38% (0%-100%). The feasibility goal for the optional nutrition education session was met (>70%) for session 1 (mean = 82% ± 40%; range 0%-100%), and almost met for session 2 (mean = 70% ± 48%; range 0%-100%). There were no serious adverse events related to the supervised or independent exercise sessions.
Secondary OutcomesFor objective physical function outcomes, there were significant improvements from baseline to 12 weeks in gait speed (+0.32 m/s, P < .01), but this did not meet the minimal detectable change (MDC) of 0.72 m/s32; 30-second bicep curls (+4.0 repetitions, P < .01), achieving the MDC of 2.3 repetitions33; 6MWT (+58.1 m, P = .01), achieving the minimal clinically important difference of 54 m34,35; and 5 repetitions of chair stand test (–3.8 seconds, P = .01), achieving the MDC of 2.5 seconds36 (Table 3).
TABLE 3 - Feasibility, Physical Function, and Patient-Reported Outcomes: Change Over Time Feasibility Outcomes (n = 11)a A Priori Target Result Feasibility Achieved Accrual 100% 37% No Attendance >70% 84% Yes Adherence virtual sessions >70% 78% Yes Adherence at home session >70% 57% No Attrition <30% 21% Yes Safety None None Yes Group belongingness >75% 90% Yes Physical Measure (n = 10)b Baseline 6 Wk 12 Wk Change Baseline to 12 Wk P Effect Sizec Body weight (kg) 62.3 62.7 62.3 0 .717d 0.033 Body mass index 24.3 24.8 24.2 –0.1 .905d 0.010 Waist circumference (cm) 86.9 86.5 82.8 –4.1 .670d 0.040 Hip circumference (cm) 98.8 97.8 101.2 +2.4 .020d,e,f 0.390 Gait speed (m/s) 1.1 1.3 1.4 +0.32 .009d,e 0.469 Chair stand (s) 12.6 9.1 8.8 –3.8 .025d,e,g 0.370 Biceps curls (repetitions) 12.5 15.0 16.5 +4.0 .005d,e 0.538 6-Min Walk Test (m) 539.7 574.8 597.8 +58.1 .045d,e 0.310 Timed up and go (s) 5.9 5.8 4.3 –1.6 .273d 0.130 Reach test (in) 12.1 12.5 15.5 +3.4 .097d 0.259 Balance score 4.0 4.0 4.0 0 .368d 0.100 SF-36 Item (n = 11) Baseline 6 Wk 12 Wk P Change Baseline to 12 Wk Effect Sizec 24 Wk 12 vs 24 Wk P Physical functioning 75.0 80.0 75.0 .622d 0 0.043 75.0 0.835h Role limitation physical health 50.0 25.0 50.0 .641d 0 0.040 75.0 0.546h Role limitation emotional 100.0 100.0 66.7 .959d –33.3 0.004 100.0 0.518h Energy/fatigue 55.0 60.0 55.0 .488d 0 0.065 50.0 0.878h Emotional well-being 72.0 80.0 76.0 .036d,e +4.0 0.302 72.0 0.893h Social functioning 50.0 75.0 75.0 .315d +25.0 0.105 62.5 0.914h Pain 67.5 57.5 77.5 .918d +10.0 0.008 67.5 0.501h General health status 50.0 55.0 55.0 .903d +5.0 0.009 65.0 1.000h HADS (n = 11) Baseline 6 Wk 12 Wk P Change Baseline to 12 Wk Effect Sizec 24 Wk 12 vs 24 Wk P Score for anxiety 6.0 6.0 7.0 .809d +1.0 0.019 6.0 .686h Score for depression 3.0 4.0 4.0 .513d +1.0 0.061 4.0 .721h Modified Godin (n = 11) Baseline 12 Wk P Change Baseline to 12 Wk
留言 (0)