Pediatric tuberculosis (TB) is both underdiagnosed and overdiagnosed, which makes accurate estimates of the disease burden difficult [1]. The manifestations are different from adult TB; children develop more extra-pulmonary disease and much less often, contagious pulmonary disease. In small children, the interval between infection and disease is weeks to months and is considerably shorter than in adults where it could be in years. These differences and the pauci-bacillary nature of disease in children makes the approach to diagnosis, treatment and prevention of TB in children necessarily unique that requires special attention [2]. In this issue of IJP focusing on pediatric TB, important aspects such as the epidemiology, newer advances in the diagnosis, current treatment approaches including shortened treatment regimens for drug sensitive TB and that for drug resistant TB, sequelae after TB treatment and preventive treatment have been dealt with by experts.
The article on the current epidemiology of tuberculosis describes the global and Indian trends in tuberculosis, especially that in children who contribute to 5.7% and 3% of the total burden of drug susceptible and drug resistant TB respectively. The adverse impact of the COVID-19 pandemic resulting in delayed diagnosis and a reversal in the gains achieved before the pandemic are also described. It also delves into the risk factors for TB exposure, infection and disease and addresses some of these preventable or modifiable factors such as malnutrition, alcohol use, smoking, diabetes and HIV [3].
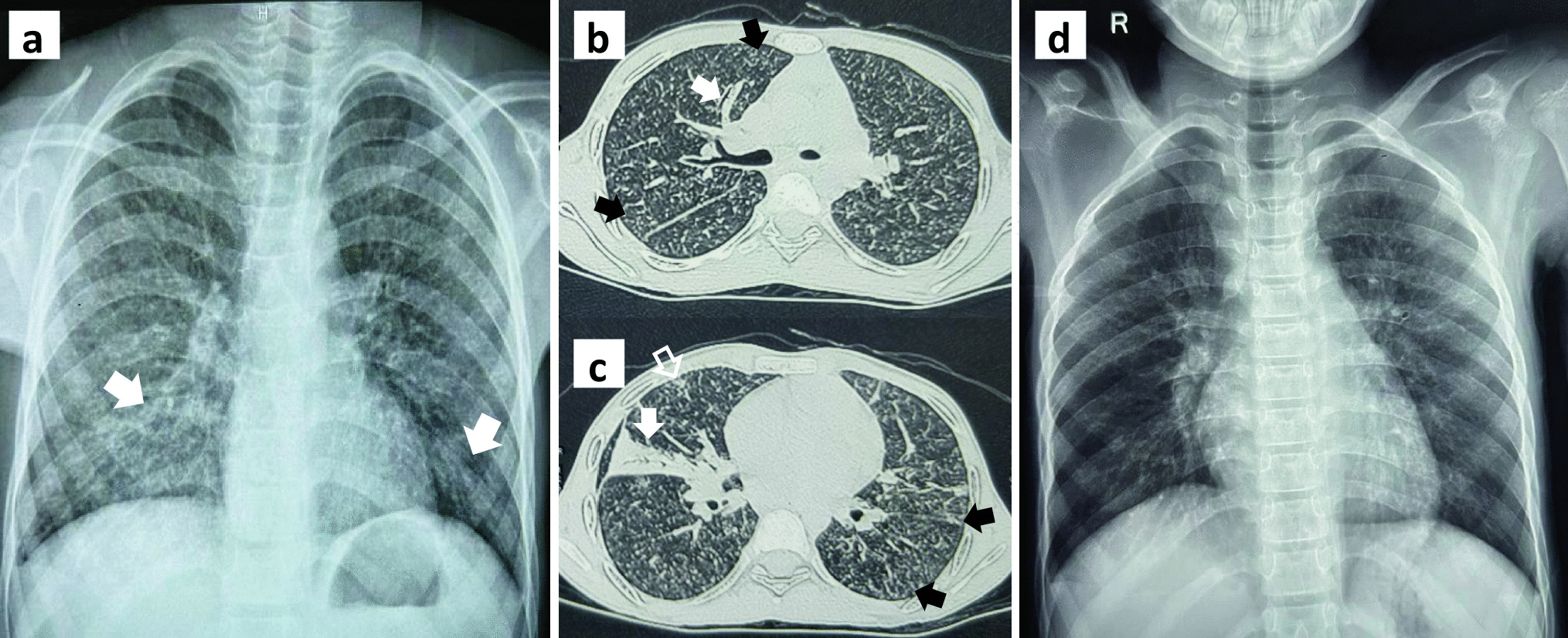
The diagnosis of pediatric TB is challenging due to many reasons such as, the spectrum of disease being age dependent with the younger children often presenting as paucibacillary intrathoracic or disseminated disease with non-specific signs and symptoms, the effect of BCG and environmental mycobacteria on the interpretation of the tuberculin skin test (TST) to diagnose infection, the difficulty in the interpretation of chest radiographs for features pathognomonic of TB and the complexities in collecting specimens for microbiological diagnosis when there is low bacillary load [4, 5]. The article on ‘What is new in the diagnosis of childhood tuberculosis?’ explores the newer modalities that attempt to fill some of these gaps in the diagnosis of pediatric TB. The use of C-Tb skin test as an advancement to overcome the pitfalls of traditional TST in diagnosing TB infection; the advancements in the field of radiology in reading of Chest X-rays and CT scans using Computer Assisted Detection (CAD) software, the use of ultrasound as a point of care test in aiding with the diagnosis of TB and the use of MRI and PET scans; the use of urinary lipoarabinomannan (LAM) especially in HIV affected individuals; the advances is sampling methods to obtain appropriate representative samples such as nasopharyngeal aspirate, gastric lavage, stool, oral swabs or mask samples for the diagnosis of pediatric TB; the recent advances in the molecular techniques including newer sequencing techniques and the use of biosignatures such as transcriptomic profiles are discussed in detail [6].
The treatment of pediatric TB is determined by the type of TB disease (with longer duration required in meningeal and osteoarticular disease) and the susceptibility pattern of the Mycobacterium tuberculosis in the affected child. The weight based dosing requiring multiple tablets, the palatability of the drugs, the difficulties in maintaining compliance for at least 6 mo and the adverse effects of the drugs push clinicians and researchers to evaluate simpler regimens with shorter durations without compromising cure or increasing rates of drug resistance. The article on shortened treatment regimens for drug sensitive TB explores these options especially those approved by the World Health Organization (WHO) for use such as the 2HRZE+2R regimen for non-severe drug sensitive TB, 2HPZM+2HPM for >12 y and >40 kg without evidence of extrapulmonary TB and 6HRZEto for children with tuberculous meningitis [7]. The treatment of drug resistant TB has undergone significant changes over the past decade with the advent of newer drugs such as Bedaquiline and Delamanid and their availability for use in children. The article on drug resistant TB describes these recent developments including the current classification of 2nd line anti-tuberculous drugs as per the WHO, the general principles and considerations while treating children with drug resistant TB, the use of 9–12 mo standardized regimens for treatment of RR/MDR TB, the considerations for individualized regimens especially in whom standardized regimens are not suitable, duration of treatment and the adverse effects of drugs. The role of microbiological confirmation of drug resistant TB has been suitably emphasized in the article [8].
Most TB programs define cure as resolution of symptoms along with microbiological and radiological clearance and do not capture the sequelae following TB disease. The socio-economic burden of TB disease and sequelae following pulmonary TB and extrapulmonary TB especially CNS, spine, abdominal osteoarticular, skin and urogenital disease in children are often not considered and deserve special attention as they contribute considerably to the disability adjusted life years (DALY). These aspects are dealt with in a separate article that highlights the sequelae related to the type of TB disease including the clinical manifestations, risk factors and its treatment [9].
Prevention is always better than cure. It is unfortunate that TB preventive treatment (TPT) is underutilized even when there is sound evidence to show that it can prevent disease in individuals who are infected and in exposed contacts who are at high risk of disease such as children <5 y of age and immunosuppressed individuals. The article on TPT describes its historic perspectives, the scientific rationale for its use, the different categories of people for whom TPT is applicable, the standard Isoniazid regimen and the other regimens for drug susceptible TB, the regimens for drug resistant TB and the contra-indications for TPT [10].
In summary, the series of articles will give the readers an updated comprehensive overview of the different aspects of pediatric TB including its epidemiology, TB prevention and post treatment sequelae and the nuances and challenges in the diagnosis and management of clinical disease including that of drug resistant TB.


留言 (0)