The elbow is the second most common dislocated joint after the shoulder joint1. An elbow dislocation can be classified as simple or complex. A simple elbow dislocation (SED) is a dislocation without associated fractures2. In many SEDs, small avulsions of the medial and/or collateral lateral ligaments or the capsule are seen; these avulsions are not classified as fractures1. The elbow dislocation has an incidence of 5 to 6 per 100,000 per year, of which 74% are SEDs3,4.
The trends concerning the therapy of a SED have changed over time. Previously, nonoperative therapy consisted mainly of immobilization and casting the elbow, with relatively good long-term outcomes5. Approximately 8% of patients with SEDs may experience persistent instability after nonoperative treatment or stiffness. The latter led to a focus on short-term immobilization (<7 days) or no immobilization at all, with active movement initiated immediately after closed reduction6,7. In addition to nonoperative therapy, there is a trend toward surgical intervention for elbows with gross instability after SED8. Optimizing the treatment strategy is important as suboptimal treatment may result in pain, persistent or recurrent instability, stiffness, posttraumatic arthritis, and the need for additional surgical intervention9.
The primary aim of this study was to systematically review the literature and analyze the outcomes and complications of different treatment options for acute and persistent elbow dislocations (PEDs), including operative and nonoperative treatments with varying immobilization periods. In addition, the secondary aims were to assess the outcomes of PED and SEDs in pediatric patients. By providing a comprehensive overview of the available evidence, this systematic review offers a new perspective on treating SEDs and can assist in shared decision-making regarding treatment options.
Methods
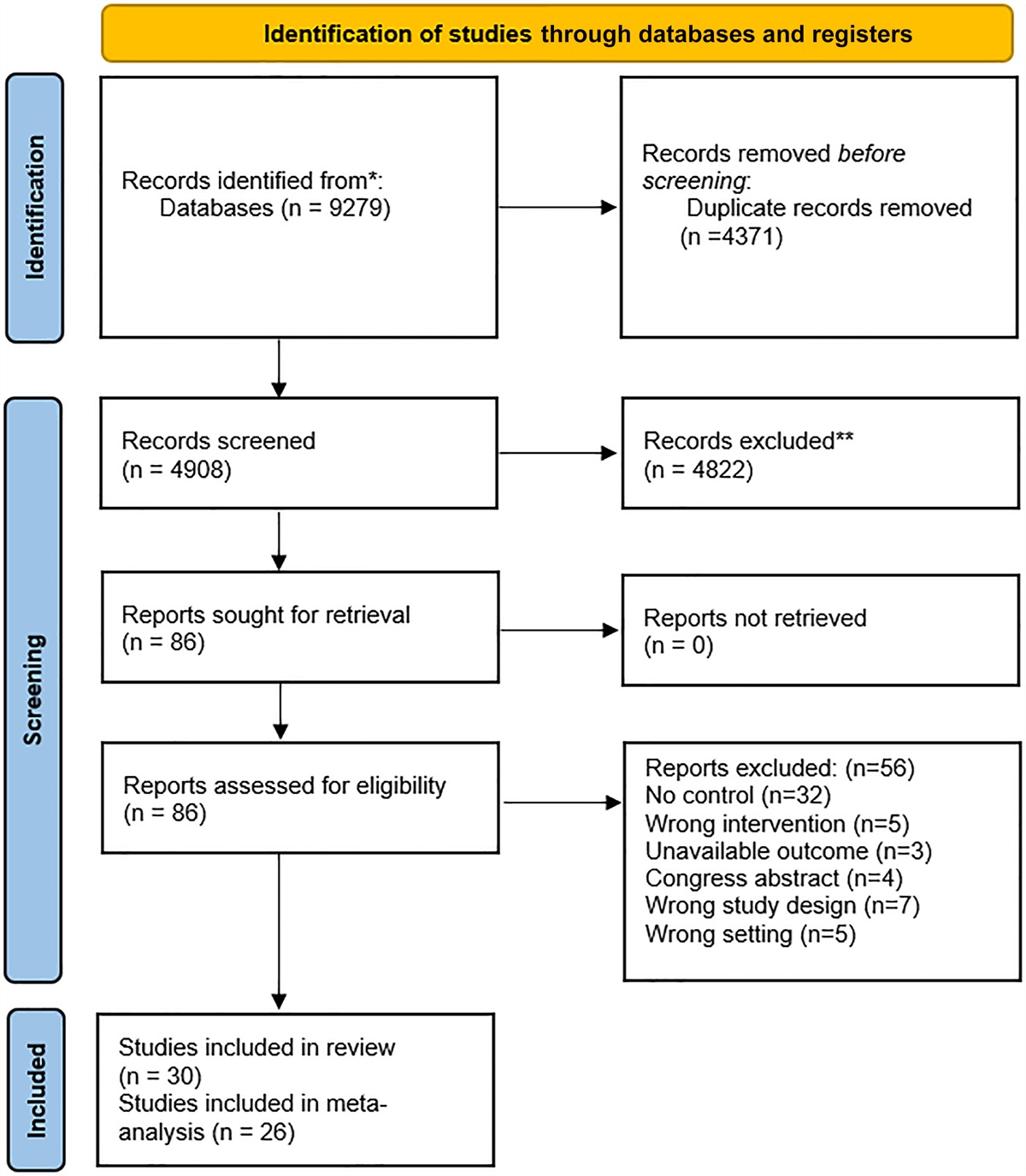
A systematic literature review was conducted according to the Preferred Reporting Items for Systematic Meta-Analyses guidelines10. The review was registered in an international prospective register of systematic reviews (PROSPERO). The protocol is registered under the following number CRD42021287756 and can be accessed electronically at http://www.crd.york.ac.uk/prospero.
Literature Search and Study Selection
A literature search was performed with the help of a clinical librarian (S.P.-V.) based on the online medical databases MEDLINE, Embase, and the Cochrane Central Register of Controlled Trials. The search strategy is presented in Appendix 1. Title, abstract, and full-text screening were performed by 2 independent reviewers (C.M.J.M.P. and H.H.d.K.) to identify potentially relevant articles. The authors independently selected articles. Studies were not blinded for author, affiliation, or source. Any disagreements were resolved by a third author (M.P.J.v.d.B.).
Inclusion and Exclusion Criteria
Articles presenting patients with a SED were eligible for inclusion. Patients with an acute or persistent total SED, without associated injuries, preexisting elbow pathology, or previous surgery in the ipsilateral elbow were included. Patients with an isolated radius dislocation were excluded. Studies were included if they were written in English, German, or Dutch; had at least 12 months of follow-up; and reported on a minimum of 5 patients. Studies had to contain at least one of the outcome parameters (patient-reported outcome measures [PROMs], range of motion [ROM], or complications) to be included. Reviews, biomechanical and cadaveric studies, expert opinions, and surgical technique articles were excluded.
Data Extraction
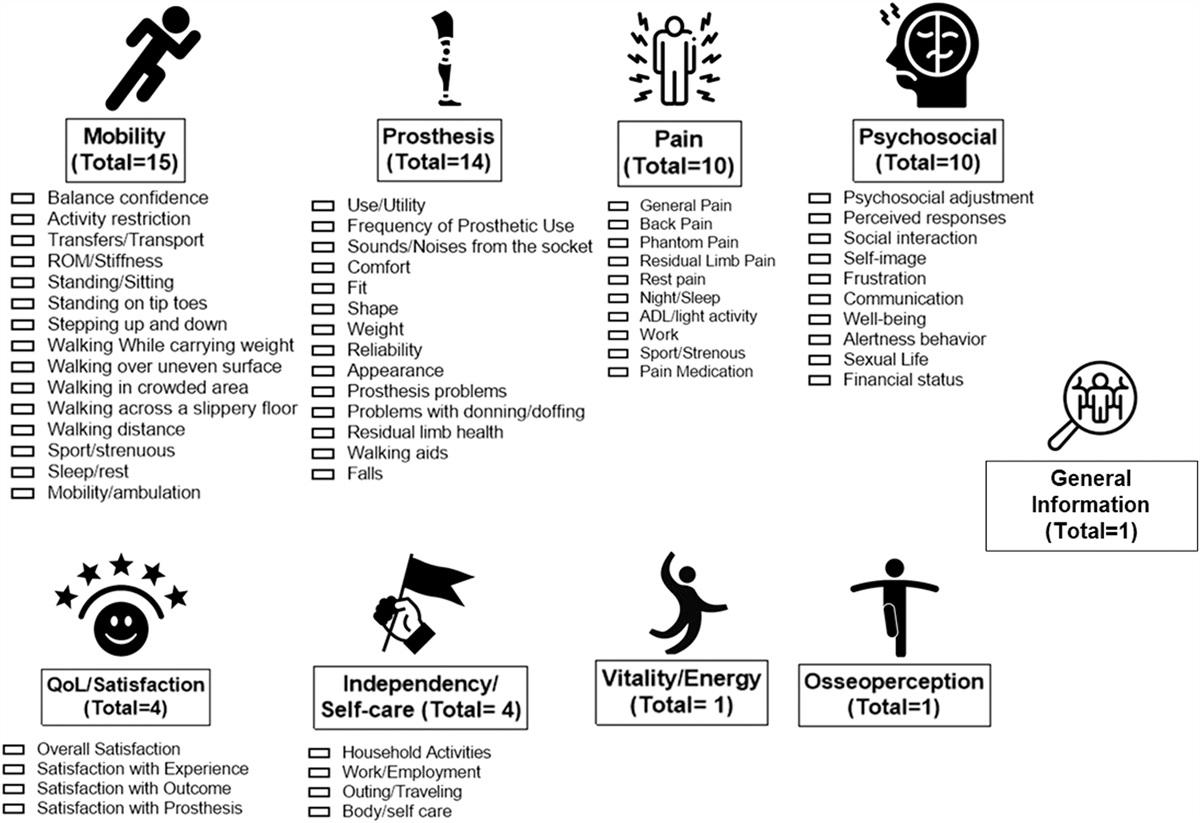
When available, the following baseline parameters were recorded: number of patients and elbows, sex, age, dominant side, and laterality of injury. Furthermore, the following intervention parameters were recorded: type of nonoperative treatment (the type of immobilization, duration of immobilization, and duration of early motion) or surgical treatment (medial collateral ligament repair and/or lateral collateral ligament repair). Relevant outcome parameters included the months of follow-up; pain score measured using the visual analog scale; continuous satisfaction rate; ROM of the elbow in flexion-extension and pronation-supination; Mayo Elbow Performance Score (MEPS); Quick Disabilities of the Arm, Shoulder, and Hand (qDASH) score; rate of return to sport; complications; and information about revision surgery or surgery after initial nonoperative treatment. The MEPS is an elbow outcome score used to test the limitations in the elbow during activities of daily living. A total score between 90 and 100 points can be considered excellent; between 75 and 89 points, good; between 60 and 74 points, fair; and <60 points, poor11. The Disabilities of the Arm, Shoulder, and Hand (DASH) score is a well-recognized instrument for measuring upper-limb function and symptoms. The qDASH score represents the disability/symptom score, which includes 11 items from the original DASH's 30 questions. This tool is performing well with strong evidence supporting reliability12. Each item of the qDASH has 5 response options (scored 1-5) used to create a summative score ranging from 0 (no disability or symptoms) to 100 (greater disability or symptoms).
Because there were many different options for the duration of immobilization and mobilization, we categorized them under treatment groups. Treatment groups consisted of early mobilization (<7 days), 1- to 3-week immobilization, ≥3-week immobilization, and surgery. The surgery group included 2 subheadings: patients who underwent surgery as their first choice of treatment or after failed nonoperative treatment and patients with PEDs. An elbow dislocation is defined as persistent when it persists for >3 weeks13. Some studies compared different groups; therefore, the different groups were collected separately when possible. The ROM flexion-extension arc was determined by subtracting ROM extension values from the ROM flexion values. Pediatric patients were also presented in Tables I and II, but Table III presents a subgroup analysis. Pediatric patients are defined as patients younger than 18 years.
TABLE I -
Outcomes of Nonoperative Treatment in SED
*
Study
Total
Adults
No. of Elbows
Mean Age (yr)
Mean Functional Outcome by Study
†
Complications, n (%)
Mean Follow-up (mo)
No. of Elbows
Mean Age (yr)
Mean Functional Outcome by Study
†
Complications, n (%)
Mean Follow-up (mo)
Early mobilization
Hopf et al., 2015
19
22
53.1
MEPS 94.1
qDASH 6.1
ROM F/E 146°
ROM P/S 165°
0 (0) minor
3 (4) major
59.6
22
53.1
MEPS 94.1
qDASH 6.1
ROM F/E 146°
ROM P/S 165°
0 (0) minor
3 (4) major
59.6
Krticka et al., 2018
20
28
48
MEPS 97
OES 46.2
qDASH 2.5
ROM F/E 132°
14 (50) minor
0 (0) major
32
28
48
MEPS 97
OES 46.2
qDASH 2.5
ROM F/E 132°
14 (50) minor
0 (0) major
32
Van Lieshout, 2020
18
48
43
EQ-5D 0.88
OES 93
qDASH 4
SF-36 PCS 53
25 (52) minor
3 (6) major
12
48
43
EQ-5D 0.88
OES 93
qDASH 4
SF-36 PCS 53
25 (52) minor
3 (6) major
12
Schnetzke et al., 2017
8
68
37.2
MEPS 94.2
ROM F/E 135°
Flexion 138°
Extension 3°
VAS 0.8
0 (0) minor
4 (6) major
40.8
68
37.2
MEPS 94.2
ROM F/E 135°
Flexion 138°
Extension 3°
VAS 0.8
0 (0) minor
4 (6) major
40.8
Beirer et al., 2018
21
10
44
ESAS 91.8
ROM F/E 140°
ROM P/S 176
0 (0) minor
1 (10) major
44
10
44
ESAS 91.8
ROM F/E 140°
ROM P/S 176
0 (0) minor
1 (10) major
44
Maripuri et al., 2007
38
22
41
DASH 2.7
MEPS 96.5
0 (0) minor
0 (0) major
1-3 wk immobilization
Ataoglu et al., 2017
22
14
OES 91
qDASH 5
ROM F/E 118
Flexion 132°
Extension 14°
2 (14) minor
0 (0) major
12
14
OES 91
qDASH 5
ROM F/E 118
Flexion 132°
Extension 14°
2 (14) minor
0 (0) major
12
Calderazzi et al., 2020
5
26
43
DASH 12.8
MEPS 93.8
6 (23) minor
0 (0) major
40
26
43
DASH 12.8
MEPS 93.8
6 (23) minor
0 (0) major
40
Maripuri et al., 2007
38
20
44.4
DASH 7.5
MEPS 90.5
0 (0) minor
1 (2) major
Cho et al., 2018
23
3
61.7
MEPS 81.7
qDASH 22
ROM F/E 130°
Flexion 133°
Extension 3°
ROM P/S 146°
Pronation 73°
Supination 73°
1 (33) minor
0 (0) major
48
3
61.7
MEPS 81.7
qDASH 22
ROM F/E 130
Flexion 133°
Extension 3°
ROM P/S 146
Pronation 73°
Supination 73°
1 (33) minor
0 (0) major
48
Kerschbaum et al., 2017
24
10
38
DASH 2
MEPS 90
OES 45
ROM F/E 145°
Flexion 145°
Extension 0°
0 (0) minor
7 (70) major
54
Willin et al., 2020
39
5
46.4
Bromberg-Morrey 94
MEPS 90
OES 55.8
qDASH 20.9
SEV 82
1 (20) minor
2 (40) major
27
5
46.4
Bromberg-Morrey 94
MEPS 90
OES 55.8
qDASH 20.9
SEV 82
1 (20) minor
2 (40) major
27
Panteli et al., 2015
43
27
41.4
1 (4) minor
0 (0) major
12
Borris et al., 1987
44
63
22.2
52 (83) minor
17 (27) major
84
Josefsson et al., 1987
45
34
39
3 (9) minor
5 (15) major
84
Bettuzzi et al., 2023
47
5
11
2 (40) minor
2 (40) major
67.2
Bua et al., 2022
41
10
11
Kim 87.5
0 (0) minor
1 (10) major
>3 wk immobilization
Sofu et al., 2016
25
12
8
MEPS 91.6
ROM: F/E 120°
ROM P/S 146°
Pronation 67°
Supination 79°
0 (0) minor
4 (33) major
46
Adaş et al., 2014
26
11
9.8
MEPS 96.8
ROM F/E 129°
Flexion 137°
Extension 8°
ROM P/S 150°
Pronation 73°
Supination 77°
0 (0) minor
0 (0) major
24.3
Van Lieshout, 2020
18
52
47
EQ-5D 0.89
OES 95
qDASH 4
SF36-PCS 53
29 (56)
2 (4) major
12
52
47
EQ-5D 0.89
OES 95
qDASH 4
SF36-PCS 53
29 (56)
2 (4) major
12
Panteli et al., 2015
43
14
35.4
0 (0) minor
0 (0) major
12
Eygendaal et al., 2000
46
31
33
25 (80) minor
45 (145) major
108
31
33
25 (80) minor
45 (145) major
108
Geyer et al., 2022
37
21
37.4
ESAS 99.4
MEPS 97.3
qDASH 7.8
ROM F/E 139
ROM P/S 180
2 (10) minor
5 (24) major
72.8
21
37.4
ESAS 99.4
MEPS 97.3
qDASH 7.8
ROM F/E 139
ROM P/S 180
2 (10) minor
5 (24) major
72.8
Pincin et al., 2022
42
18
MEPS 100
OES 47.8
qDASH 0.25
*DASH = Disabilities of the Arm, Shoulder, and Hand, EQ-5D = EuroQol-5 Dimensions, ESAS = Elbow Self-assessment Score, Kim = Kim's elbow performance score, MEPS = Mayo Elbow Performance Score, OES = Oxford Elbow Score, qDASH = Quick Disabilities of the Arm, Shoulder, and Hand, ROM F/E = range of motion flexion-extension arc, ROM P/S = range of motion pronation-supination arc, SEV = subjective elbow value, SF-36 PCS = Short Form 36 physical component summary, and VAS = Visual Analog Scale.
†Posttherapy values are presented.
TABLE II -
Outcomes of Surgical Treatment in SED
*
Study
Total
Adults
No. of Elbows
Mean Age (yr)
Mean Functional Outcome by Study
†
Complications, n (%)
Mean Follow-up (mo)
No. of Elbows
Mean Age (yr)
Mean Functional Outcome by Study
†
Complications, n (%)
Mean Follow-up (mo)
Surgery
Krticka et al., 2018
20
26
50
MEPS 87.7
OES 42.5
qDASH 8.3
ROM F/E 117°
29 (112) minor
0 (0) major
26
26
50
MEPS 87.7
OES 42.5
qDASH 8.3
ROM F/E 117°
29 (112) minor
0 (0) major
26
Micic et al., 2009
27
14
34.1
MEPS 95.4
ROM F/E 116
Flexion 130°
Extension 14°
8 (57) minor
4 (29) major
32.6
14
34.1
MEPS 95.4
ROM F/E 116
Flexion 130°
Extension 14°
8 (57) minor
4 (29) major
32.6
Adolfsson et al., 2017
28
8
54
ROM F/E 130°
Flexion 136°
Extension 6°
4 (50) minor
0 (0) major
8
54
ROM F/E 130°
Flexion 136°
Extension 6°
4 (50) minor
0 (0) major
Lee et al., 2019
29
21
45.1
qDASH 4.3
ROM F/E 134
Flexion 138°
Extension 4°
ROM P/S 163
Pronation 73°
Supination 90°
1 (5) minor
16 (76) major
43.3
21
45.1
qDASH 4.3
ROM F/E 134°
Flexion 138°
Extension 4°
ROM P/S 163°
Pronation 73°
Supination 90°
1 (5) minor
16 (76) major
43.3
Cho et al., 2018
23
17
49.5
MEPS 86.5
qDASH 8.4
ROM F/E 121
Flexion 130°
Extension 9°
ROM P/S 153°
Pronation 71°
Supination 82°
5 (29) minor
0 (0) major
57.5
17
49.5
MEPS 86.5
qDASH 8.4
ROM F/E 121°
Flexion 130°
Extension 9°
ROM P/S 153°
Pronation 71°
Supination 82°
5 (29) minor
0 (0) major
57.5
Schnetzke et al., 2017
8
50
44.4
MEPS 93.4
ROM F/E 134°
Flexion 139°
Extension 5°
VAS 1
1 (2) minor
5 (10) major
40.8
50
44.4
MEPS 93.4
ROM F/E 134°
Flexion 139°
Extension 5°
VAS 1
1 (2) minor
5 (10) major
40.8
Jung et al., 2019
30
10
30.5
MEPS 85
NRS 2
qDASH 11.4
ROM F/E 130°
ROM P/S 161°
29
10
30.5
MEPS 85
NRS 2
qDASH 11.4
ROM F/E 130°
ROM P/S 161°
29
Beirer et al., 2018
21
10
43
ESAS 91.6
ROM F/E 131°
ROM P/S 173°
0 (0) minor
3 (30) major
44
10
43
ESAS 91.6
ROM F/E 131°
ROM P/S 173°
0 (0) minor
3 (30) major
44
Jeon et al., 2008
40
12
36.2
MEPS 94.2
27.8
12
36.2
MEPS 94.2
27.8
Willin et al., 2020
39
9
57.3
Bromberg-Morrey 94
MEPS 91
OES 54.7
qDASH 9.8
SEV 85
0 (0) minor
1 (11) major
36
9
57.3
Bromberg-Morrey 94
MEPS 91
OES 54.7
qDASH 9.8
SEV 85
0 (0) minor
1 (11) major
36
Josefsson et al., 1987
45
28
36
4 (14) minor
2 (7) major
36
Geyer et al., 2022
37
23
21
ESAS 99.8
MEPS 98.7
qDASH 6.3
ROM F/E 135
ROM P/S 177
4 (17) minor
6 (26) major
58.7
23
21
ESAS 99.8
MEPS 98.7
qDASH 6.3
ROM F/E 135
ROM P/S 177
4 (17) minor
6 (26) major
58.7
Persistent
Devnani, 2004
31
7
30.1
ROM F/E 83°
Flexion 110°
Extension 27°
7 (100) minor
2 (29) major
51.4
6
39.1
ROM F/E 100°
Flexion 120°
Extension 20°
43
Mahaisavariya et al., 2005
32
21
25.9
ROM F/E 84°
1 (5) minor
0 (0) major
50.3
16
31.1
ROM F/E 87°
Salihu et al., 2021
33
49
31.9
MEPS 92.6
PSFS 9.1
ROM F/E 87°
1 (2) minor
43 (89) major
12
49
31.9
MEPS 92.6
PSFS 9.1
ROM F/E 87°
12
Kapukaya et al., 2013
13
20
20
MEPS 79.3
ROM F/E 85°
0 (0) minor
10 (50) major
39.1
4
51.8
ROM F/E 51°
46.3
Anderson et al., 2018
34
32
25
MEPS 93
ROM F/E 101°
Flexion 132°
Extension 31°
ROM P/S 121°
Pronation 71°
Supination 150°
SOD 9
1 (3) minor
0 (0) major
22
24
30.6
MEPS 91.9
ROM F/E 83°
ROM P/S 120°
SOD 9 (8.6)
20.9
Mehta et al., 2007
35
6
25.2
MEPS 81.7
ROM F/E 92°
ROM P/S 150°
18
4
30.5
ROM F/E 83°
ROM P/S 150°
21
Krishnamoorthy et al., 1976
36
8
27.5
ROM F/E 93°
Flexion 124°
Extension 31°
31.5
7
36.7
ROM F/E 103°
Flexion 135°
Extension 32°
40.3
*ESAS = Elbow Self-assessment Score, MEPS = Mayo Elbow Performance Score, NRS = numeric rating scale, OES = Oxford Elbow Score, PSFS = Patient-Specific Functional Scale, qDASH = Quick Disabilities of the Arm, Shoulder, and Hand, ROM F/E = range of motion flexion-extension arc, ROM P/S = range of motion pronation-supination arc, SEV = subjective elbow value, SOD = Summary Outcomes Determination score, and VAS = Visual Analog Scale.
†Posttherapy values are presented.
TABLE III -
Outcomes of Children with SED
*
Study
No. of Elbows
Mean Age (yr)
Mean Functional Outcome by Study
†
Complications, n (%)
Mean Follow-up (mo)
1-3 wk immobilization
Borris et al., 1987
44
43
10
16 (37) minor
11 (26) major
84
Subasi et al., 2015
48
22
11.6





留言 (0)