Study design
This was a post hoc analysis of the RESTRIC trial, a cluster-randomized, crossover, non-inferiority multicenter trial that was conducted across 22 institutions in Japan and involved 422 patients [7]. The design of the RESTRIC trial has been previously published [12]. In brief, the participating institutions were randomized to two schedules at a 1:1 ratio, comparing a restrictive RBC transfusion strategy (target hemoglobin level of 7 to 9 g/dL) with a liberal RBC transfusion strategy (target hemoglobin level of 10 to 12 g/dL) among adult patients with severe trauma at risk of major bleeding. The assigned transfusion strategy was implemented for all patients starting from the initial trauma resuscitation phase, upon arrival at the emergency department (ED), and continued until 7 days after hospital admission, intensive care unit (ICU) discharge, decision to withdraw active treatment, or death, whichever occurred first. Resuscitation with fluid or other blood components, such as fresh frozen plasma or platelets, was executed at the physician’s discretion. The protocol was approved by the ethics committees of each participating institution and that of the Japanese Association for the Surgery of Trauma, in line with the declaration of Helsinki. The present study was also approved by the Okayama University Hospital Ethics Committee (K2211-031).
Participants
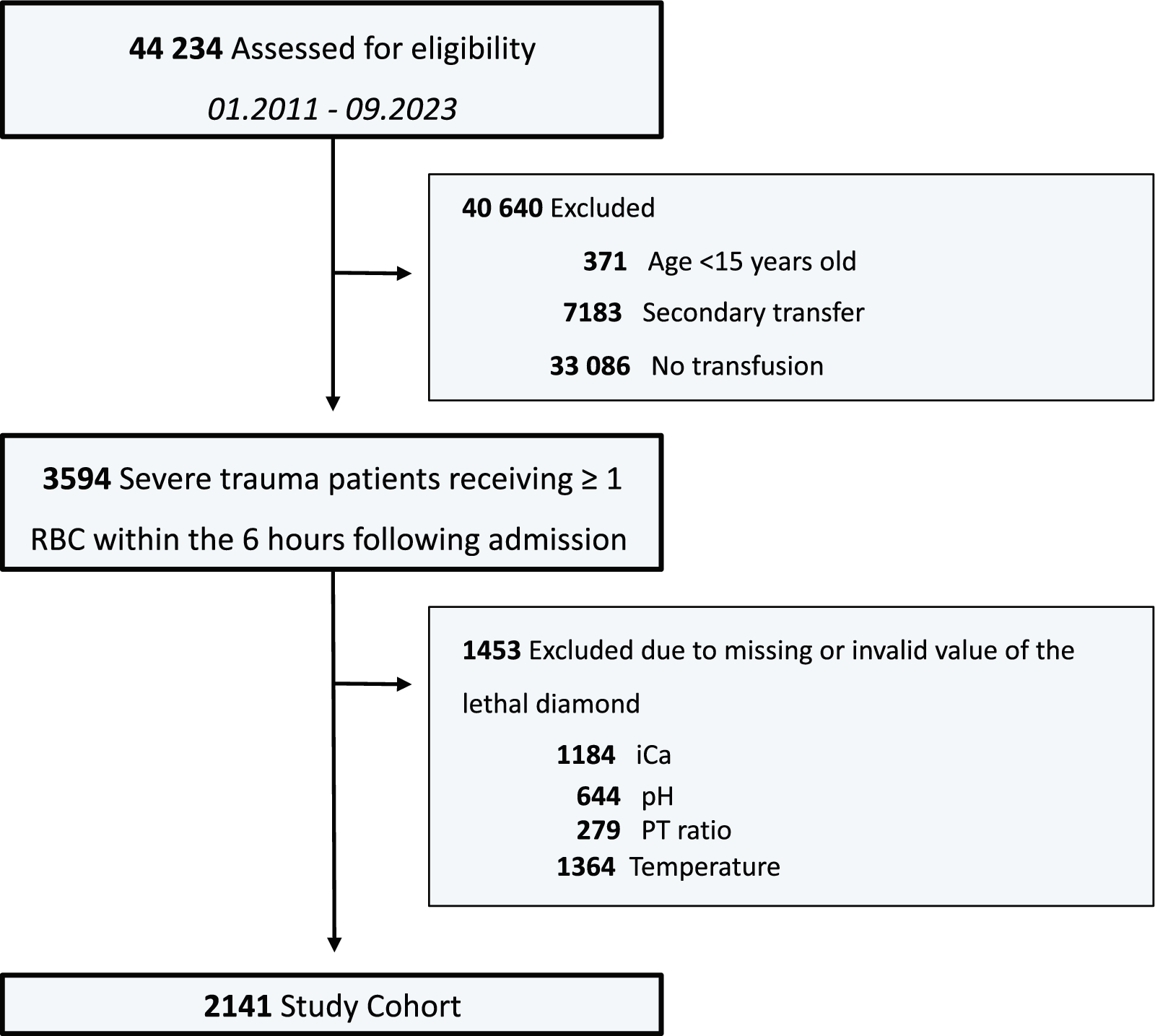
Inclusion criteria encompassed patients aged ≥ 20 years, experiencing one of the following, as judged by a physician: severe bleeding potentially leading to circulatory shock, suspected severe bleeding post-arrival at the ED, or potential for severe bleeding postoperatively during the acute trauma phase. From the participants registered in the RESTRIC trial, this post hoc analysis excluded those who withdrew consent, deviated from the transfusion strategy, were lost to follow-up, or had unavailable lactate level data upon ED arrival.
Outcomes
The primary outcome was all-cause mortality at 28 days. Secondary outcomes included: time to death, cumulative RBC concentrate usage, ICU length of stay, and ventilator-, catecholamine-, and ICU-free days within the first 28 days. Patients who died within the first 28 days of arriving at the ED had zero days without events. Additionally, occurrence of organ (renal, hepatic, and respiratory) failure within the first 7 days and complications (including deep venous thrombosis, pulmonary embolism, cerebral infarction, myocardial infarction, bowel ischemia, transfusion-associated lung injury, and sepsis) within the first 28 days were assessed.
Statistical analyses
We categorized patients into three subgroups based on lactate levels (mmol/L) upon ED arrival: low, middle, and high. This categorization is based on the findings of a previous study that also divided patients into three groups: low (< 2.5 mmol/L), middle (≥ 2.5 mmol/L and < 4.0 mmol/L), and high (≥ 4.0 mmol/L) [9]. Continuous data were expressed as medians with interquartile range (IQR), and categorical data as counts and percentages. Comparisons between the two groups employed the Mann–Whitney U test for continuous variables and the Chi-square test for categorical variables.
Cox regression analysis was utilized to estimate the hazard ratio (HR) and its 95% confidence interval (CI) for predicting 28 days mortality. Survival curves were generated using the Kaplan–Meier method and were compared with the log-rank test. Multiple linear regression analyses were employed to estimate adjusted effects on ICU-free, ventilator-free, and catecholamine-free days. The interaction p value, derived from the logistic linear regression model, was used to test the statistical significance of the interaction between lactate levels and transfusion strategy. Results were presented as β coefficients with 95% CI. Multiple logistic regression models were used to estimate the adjusted odds ratio (OR) and their 95% CI for the occurrence of any organ failure within 7 days and any complications within 28 days. These analyses were conducted for each lactate level category and were adjusted for factors including age, sex, systolic blood pressure on ED arrival, the presence of a severe head injury [defined as an Abbreviated Injury Scale (AIS) of 4 or 5 for the head], injury severity score (ISS), initial hemoglobin levels, and the need for major hemostatic interventions based on the previous studies [11, 13].
Additionally, in an exploratory subgroup analysis excluding patients with severe traumatic brain injury (head AIS of 4 or 5), similar methods were applied to estimate the HR for 28 days mortality and adjusted effects on ICU-free and ventilator-free days.
As a sensitivity analysis, we calculated the HR for 28 days mortality and the OR for the occurrence of organ failure within 7 days and complications within 28 days, using initial lactate levels as a continuous variable. For ICU-free and ventilator-free days, we estimated the β coefficients using linear regression. All these analyses were adjusted for the same variables.
All tests were two-tailed, and a p value of < 0.05 was deemed statistically significant. A threshold of p value for interaction was set at 0.10 [14]. Analyses were conducted using Stata SE version 17 statistical software (Stata-Corp LP, College Station, TX, USA) and Prism 10.0.3 (GraphPad, San Diego, CA).








留言 (0)