This study reviewed ICU clinical pharmacist contributions in the management of sepsis across the globe. Sources of variability associated with barriers and aspirations were captured. These were correlated with participant and clinical pharmacy service characteristics. Findings may be used to increase stakeholder awareness of ICU clinical pharmacist contributions and their delivery. This may improve understanding and consideration of how pharmacists can integrate into an ICU service. A unique insight into contribution barriers further provides an opportunity for stakeholders to reflect on the challenges faced by pharmacists in different settings. Whereas reported aspirations provide an opinion on developmental goals stakeholders can work with clinical pharmacists to achieve.
Defining ContributionsContribution Context
Clinical pharmacists from Western countries report reducing sepsis-related mortality and improving care quality through advisory and logistical activities [1, 2, 7,8,9, 11,12,13,14,15,16,17,18,19,20,21,22]. Typically contributions involve: guiding drug choice and administration, identifying and managing drug interactions or prescribing errors, therapy modification based on patient/concomitant medication factors, reducing antimicrobial prescribing and administration delays, patient and clinician education, generating guidance, medication reconciliations including history taking and medication reviews. Delivery is typically reported through bedside activities such as ward round interventions, supported by back-office operations [1,2,3,4, 6•, 7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24, 26, 27•, 28•, 29•, 30, 31•, 38, 39]. Variance in pharmacist contribution outcomes exists, and is likely due to differing local practices and metrics capture. Due to a lack of comparative studies, contribution impact from bedside and non-bedside clinical roles is unclear. Although, increased scope of clinical pharmacist practice can be attributed to patient bedside locations [1,2,3,4, 6•, 7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24, 26, 27•, 28•, 29•, 30, 31•, 38, 40,41,42]. Study findings offer additional insights into contributions prior to and after antimicrobial prescription generation. Particularly for AMS, prescribing and digital activities. Furthermore, identification of contributions delivered by ICU clinical pharmacists within sepsis outreach teams and ICU triage pathways is novel. Associated impact of additionally identified contributions and delivery mechanisms on patient clinical outcomes should be investigated. Empirical evidence suggests suboptimal patient outcomes when seven-day pharmacy services closer to patients’ bedside are not employed [34•]. Therefore, stakeholders should consider the benefits of assisting clinical pharmacists accordingly. This could be achieved by working with pharmacists to identify and address associated barriers, whilst capturing local metrics to support service changes.
Contributions Prior to/at Time of Prescription
Reported independent and supplementary prescribing, plus digitally facilitated activities are examples of evolving clinical pharmacist roles in sepsis. Furthermore, an AMS sub-speciality of contributions not previously associated with pharmacists is emerging. Associated reported activities include de-labelling of patient allergies, generating antibiograms and leading TDM activities [32, 40, 41]. Although, such activities were only reported in select institutions where clinical pharmacists were well-integrated into MDTs at the bedside. Sharing stakeholder experiences of pharmacists and implementation strategies at such institutions, could offer constructive learning opportunities. In other settings, evolving contributions may contend with traditional MDT roles, preventing adoption. However, stakeholder assessment of how pharmacists’ skillset could be integrated, enhanced and balanced within the MDT has demonstrated benefits. Including reductions to MDT workloads, reduced ICU workforce shortages and enrichment of patient outcomes (particularly for TDM) [2, 8, 12, 15, 17, 19, 30, 32, 34•, 36, 40, 41, 43,44,45,46,47]. Further research on which professional partnerships offer the best quality metrics and return on investment would be useful for commissioners. Whereas implementation research and regulatory consideration of evolving clinical pharmacist roles outlined by professional bodies, could further support adoption [8, 11, 16, 17, 19, 27•, 36, 48].
Post-Prescription Contributions
Clinical re-assessment, data review and antimicrobial modification, are common activities associated with clinical pharmacist advice. Increasingly, pharmacists reported using ePMA technology as a tool to facilitate medicines optimisation and AMS activities [8, 9, 11, 16, 17, 20, 21, 26, 32, 47]. By harnessing technological advancements, some pharmacists have demonstrated that they are well-positioned to embrace evolving ICU landscapes [6•, 10, 35]. ICUs could therefore utilise pharmacists to undertake greater clinical governance activities and metric reporting, including AMR surveillance [8, 11, 16, 17, 32, 40, 41]. Clinical pharmacist integration into sepsis response teams and emergency department triage pathways, has demonstrated reduced ICU admission rates and improved clinical outcomes [1, 2, 8, 15, 16, 18, 20,21,22, 24, 45, 47, 49]. Therefore, pharmacists should be considered in sepsis-related performance strategies [5•, 30, 50, 51]. Providing pharmacists with opportunities to upskill in PK/PD expertise, may also improve likelihood of antibiotic effectiveness in complex patients. Supporting pharmacists with the time and resources they need to develop this skillset and fulfill their research ambitions, may also empower ICUs to offer unique cutting-edge services [7, 8, 11, 16, 17, 27•, 36, 43,44,45,46, 52, 53,54,55,56].
Exploring VariabilityParticipant Characteristics
The study’s recruitment strategy is subject to response and selection bias. This restricted insight into pharmacists’ contributions from smaller, remote institutions and less-developed countries [28•, 29•, 33•, 34•, 57]. Despite this, participants from six continents were represented. However, findings reinforce that ICU clinical pharmacy is a sub-speciality of clinical pharmacy established predominantly in developed nations or well-resourced institutions [28•, 29•, 33•]. Clinical pharmacist contributions and associated impact has been correlated with seniority and experience [27•, 36]. Therefore, although the study sample underrepresented junior pharmacists, it offers a unique perspective to answer the research question.
Clinical Pharmacy Service Characteristics
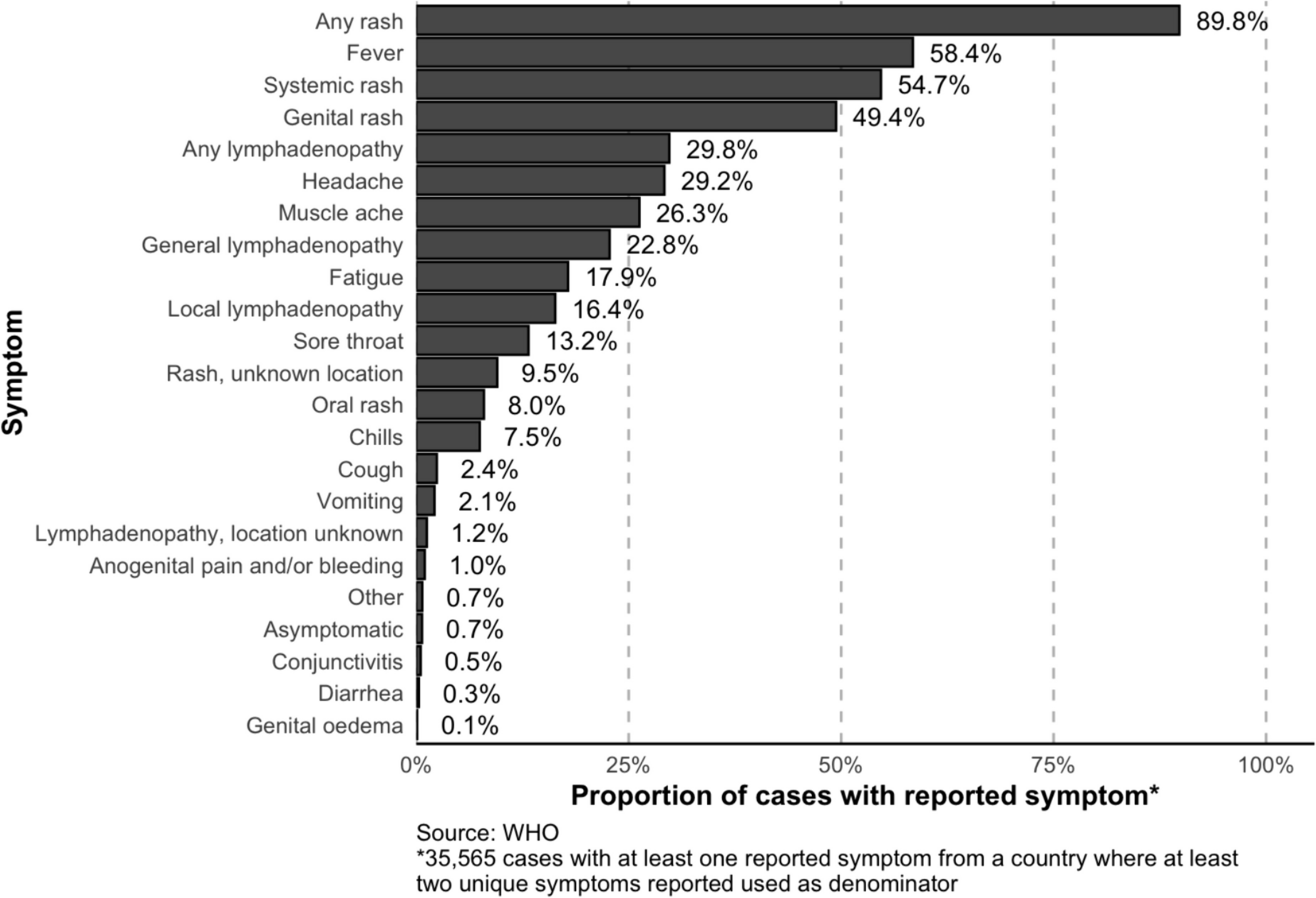
Sepsis contributions generally consisted of World Health Organization (WHO)/Centers for Disease Control and Prevention (CDC) AMS components [32, 40, 41]. Advisory contributions based on antimicrobial dose adjustment, administration and TDM were reported by all participants. However, inconsistencies in contribution type and detail emerged between bedside and non-bedside clinical contributions. Particularly for activities relating to medicine reconciliation, sepsis recognition, [5•, 50, 51] utilisation of ePMA software and prescribing. These disparities were associated with physical, social, financial and education/training themed barriers tabulated in Online Resources 2a and 2b plus Fig. 1 [28•, 29•, 33•]. Interestingly, institutions with limited or no ICU clinical pharmacy services were reported in both Western and non-Western countries [28•, 29•, 33•]. This suggests that a greater emphasis may be placed on social barriers in preventing clinical pharmacy adoption and expansion of practice. Advocacy of ICU clinical pharmacy services to stakeholders at such institutions by professional leaders, with endorsement from politicians could be an effective approach. This could emphasize sub-optimal clinical outcomes and increased expenditure associated with the abscence of clinical pharmacy services [1, 2, 4, 7, 8, 11, 15,16,17, 34•, 57]. This could be associated with local authority enforcement of a national/international consensus on ICU service standards, specifying minimal safe clinical pharmacist to patient staffing ratios [6•, 10, 17, 29•, 34•, 57,58,59].
Physical Barriers
Inconsistent pharmacy workforce provisions and prohibitive barriers were identified in many non-dedicated ICU clinical pharmacist services. These issues were associated with preventing timely contributions at sepsis onset, plus the breath of contributions [28•]. Reduced supply given the demand for competent ICU clinical pharmacists and provision of safe staffing levels, [29•] is associated with multiple factors [6•, 10, 38, 58, 60•, 61]. Whereas prohibitive pharmacist access to the ICU and patient records, alongside poor utilisation of ePMA resources may be associated with social barriers and health inequalities [9, 20,21,22, 26, 29•, 34•, 47, 60•, 61]. Legislation limiting the scope of clinical pharmacists’ practice was often reported to be interlinked and compound such barriers.
Solutions to workforce issues guided by reported ambitions could include robust local staffing mechanisms. Including greater utilisation of pharmacy technicians, well-evidenced ICU clinical pharmacist business cases, on-call or twenty-four hour bedside clinical pharmacy services, increased pharmacy undergraduate engagement and incentivising ICU development pathways [6•, 10, 29•, 34•, 57, 58]. Whereas interlinked social and physical barriers could be tackled through advocacy solutions, interprofessional education and ICU pharmacist accreditation. Similar strategies have been reported to advocate national changes in legislation and stakeholder perceptions of clinical pharmacists in the UK [27•, 29•, 33•, 34•,






留言 (0)