Study setting
This study was conducted between July 2019 and October 2021 in three districts in southeastern Tanzania: Kilwa district in Lindi region and Rufiji and Kibiti districts in Pwani region. The selection of these districts was purposive, taking into account logistical considerations and the variation in malaria prevalence as indicated by health facility data. In each district, two wards were selected representing four catchment populations. The catchment population in this context refers to the group of individuals who live within the service area of a particular health center. The boundaries of catchment areas are determined at the ward level—a local administrative division within a district—and determined based on health records. There was a total of 62 health facilities in the study area. These facilities included both public and private institutions, ranging from larger health centres which typically serve as the principal healthcare provider at the ward level to smaller dispensaries which are the primary healthcare units at the village level.
These catchment areas, including all villages located within these areas, were then assigned to either an intervention group or a control group based on malaria incidence rates (MIRs) and positivity rates. MIR is defined as the total number of malaria positive cases divided by population size from census conducted by the project team in 2019. Positivity rate is defined as the number of malaria positive cases divided by total number of malaria tests, recorded in the previous three years at the health facility level. In this study, the primary operational level was a village with an average of 2500–5500 inhabitants. We also imposed a minimum distance of 30 km between the centers of intervention and control wards to minimize spillover. Based on the 2012 census, the total population for these selected wards was approximately 243,449 people.
1,7-mRCTR approach
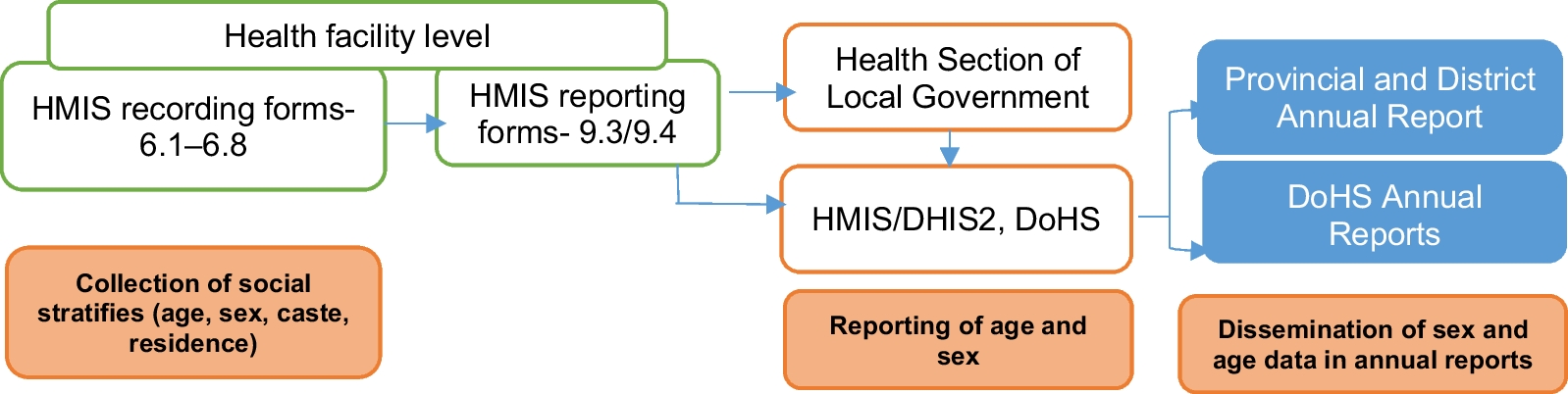
The 1,7-mRCTR approach involved reporting any confirmed malaria cases at health facilities within one day and conducting follow-up community-wide testing in selected villages within seven days to slow malaria transmission in the same phase of the Plasmodium life cycle. The main intervention was community-based malaria testing and treatment based on surveillance data from health facilities. We developed a case-based reporting system using the Open Data Kit (https://opendatakit.org/) tool to capture information on malaria cases at health facilities. The reporting system was compatible with the District Health Information Software 2 (DHIS2) platform (https://www.dhis2symposium.org/) and allowed data aggregation and sharing. We provided tablets to health facilities to collect case-based data, including patients’ demographic information and their residence village. Data from all confirmed malaria cases were aggregated weekly to calculate a village-level MIR.
Villages with the highest MIR within each catchment area were targeted for community-based malaria testing and treatment in each week. Field supervisors first notified local leaders that their villages were identified as malaria hotspots for malaria testing and treatment. Local leaders then met with CHCWs, who were recruited from the study areas, to select the location for community mobile testing stations. The testing stations were placed in areas with clustered households to provide easy access for community members. From Monday to Friday, CHCWs set up testing stations in different hamlets of the targeted villages, starting with those presumed to have the highest burden of malaria cases and moving around to increase testing coverage. If there was a school in the targeted village, the testing and treatment campaign was conducted on the premises of the school at least one day a week. The field team requested head teachers to provide a list of students who lived in the targeted village, and while other students were invited to participate in testing and treatment campaigns, only data from students residing in targeted villages were recorded.
All individuals who were at least six months of age were eligible to participate in malaria testing and treatment. Malaria testing was done with rapid diagnostic tests [RDTs; CareStartTM Malaria Pf/PAN (HRP2/pLDH) Ag Combo, Access Bio, Inc 65 Clyde Rd., Suite A, Somerset, NJ 08873, USA] at community testing stations. Participants who tested positive were given a short survey, including questions about their travel and medical history, and offered a full regiment of artemisinin-based combination therapies (dihydroartemisinin piperaquine phosphate) according to the National Malaria Treatment Guidelines [7]. The first dose of malaria treatment was given via directly observed treatment at the testing station. Pregnant women who tested positive for malaria were referred to nearby health facilities for follow-up care.
A social team comprised of sociologists, CHCWs, and local leaders conducted a series of activities before and during the campaigns to encourage community participation and offer health education. In the week preceding the campaigns, the social team sent out messages via megaphones to encourage voluntary malaria testing and emphasized that testing and treatment were provided at no cost. The social team also distributed user-friendly booklets and posters that were written in the local language and highlighted the importance of early testing, treatment adherence, use of long-lasting insecticidal nets, and environmental control. Detailed activities for the 1,7-mRCTR intervention have been published previously [18, 19].
In addition to malaria testing and treatment, larviciding was provided in the intervention wards in Rufiji district to reduce the vector population and to further drive malaria transmission towards a pre-elimination phase. Larviciding was implemented between November 2020 and October 2021 through a community-based approach using either Bacillus thuringiensis var. israelensis or Bacillus sphaericus, called BACTIVEC and GRISELESF, respectively, and produced in Tanzania. All the larval habitats identified in the area were targeted with larvicide application weekly, except when interrupted by either heavy rains or floods. Villages in both the intervention and control areas continued to benefit from the routine malaria control program implemented by the National Malaria Control Programme, such as vector control, distribution of long-lasting insecticide-treated nets, and routine malaria case management at health facilities.
Data collection via household surveys
We used two waves of cross-sectional household surveys to assess the effects of the 1,7-mRCTR approach in the study wards located in three districts of Tanzania. The baseline survey was conducted between July 24, 2019 and September 4, 2019, and the endline survey was conducted between September 20, 2021 and October 27, 2021. We used a stratified sampling approach to select households within a village and then individuals within a household. All households located in the study ward were enumerated and a random sample of households was recruited to participate in the study. If a household was not available for the interview, we recruited the household next door.
Within each household, we first interviewed the head of household and then randomly selected one available household member from each of three age groups (under 5 years, between 5 and 15 years, and above 15 years) to participate in the survey. For individuals aged 15 or under, we obtained informed assents and parental consents before conducting interviews and malaria tests. For children who were unable to respond to the survey themselves, we interviewed the head of household or a child’s caregiver on questions related to the use of preventive measures and care seeking behaviors.
The household surveys were developed based on the Malaria Indicator Survey Tool and collected data on socio-economic characteristics, knowledge, and use of malaria preventative measures, health expenditures, use of health services, and travel history [20]. We also collected blood samples from selected household members for malaria testing, including RDTs, blood smears to determine parasite density at a central laboratory, and dried blood spots collected on filter paper and preserved for later PCR-based parasite detection. All blood samples were drawn from a single finger prick to collect a total of ≤ 30 μl of blood. Participants who tested positive based on RDT results were offered free treatment according to the National Malaria Treatment Guidelines, and the first dose was given via directly observed therapy. If a participant refused this treatment option, they were referred to a nearby health facility with logistical assistance.
Outcomes
The main outcome was malaria status assessed via RDTs. The secondary outcomes included self-reported fever in the previous 14 days and underarm temperature measured using a digital thermometer during household surveys. To determine sample size, we used a stratified sampling approach to select the number of villages and then the number of households within each village [21], using malaria prevalence data from health facilities and population data from the National Bureau of Statistics which is public available (www.nbs.go.tz). The precision of the estimated sample size for areas with low parasitemia was set to 0.03 to adjust for the difference in prevalence between community and health facility estimates. We assumed a non-response rate of 10% and an average of five residents per household. Weights calculated as the relative proportion of a village population size to the total stratum population were applied to obtain the final sample size.
Ethical considerations
Informed consent was obtained from heads of household and household members who were 18 years of age or above. For those under 18 years of age, informed consent was obtained from parents or guardians. The consent forms were prepared in English and translated into Kiswahili. For individuals who were not able to read, the informed consent form was read out by the local CHCWs in the presence of a community witness, and the participant was asked to mark a thumb impression on the form. Institution ethical approval was obtained from the Ifakara Health Institute Institutional Review Board (IHI/IRB/EXT/No: 18–2020) and the National Institute of Medical Research (NIMR/HQ/R.8a/Vol. IX/3634).
Statistical analysis
We used a difference-in-differences (DID) quasi-experimental design to assess the impact of the 1,7-mRCTR approach on malaria prevalence. The DID design compares changes in malaria prevalence before and after the intervention in “treatment” areas, with changes in malaria prevalence during the same period in “control” areas. A key assumption of the DID methodology is that changes in outcomes in the treatment areas would have been similar to the changes in outcomes in the control areas in the absence of the intervention [22].
We analyzed outcomes using a multi-level regression model, in which individuals are nested within households which are nested within villages. The primary outcome in the linear probability model was a binary variable equal to one if an individual tested positive for malaria. The dependent variables included a binary “post” variable equal to one for the endline survey measures and zero for the baseline survey measures, an interaction between the “post” variable and an indicator variable equal to one if the individual lived in a treatment village, and a full set of village fixed effects. The model controlled for household characteristics (ownership of any treated mosquito net, flush toilet, improved source of drinking water, house ownership, and health insurance) and household member characteristics (age and sex). Standard errors were adjusted for clustering at the household level to account for the correlation of members from the same households.
We conducted several sensitivity analyses to assess the robustness of our results. First, we compared the results from alternative model specifications, including probit models instead of linear probability models, clustering standard errors at the village and ward levels instead of the household level, and including different sets of control variables. Second, since treatment assignment was not random, we performed coarsened exact matching on average age and access to improved water sources, two variables that were significantly different at baseline, at the village level to improve the comparability between the intervention and comparison groups [23]. Specifically, we used baseline data aggregated at the village level to match villages and then compared endline malaria prevalence among matched villages, applying weights generated from the baseline data. This matching procedure retained 55 out of the 85 villages that were surveyed in both waves and achieved a better balance in village characteristics in the baseline (Additional file 1: Table S1). We only included two variables because adding a third matching variable retained fewer than one third of the villages in the original sample.
Since intervention areas in Rufiji district received larviciding treatment in addition to the other components of the intervention, we assessed the intervention effects in Rufiji separately in addition to the overall effects in the three districts combined. We conducted subgroup analyses to assess intervention effects by age, sex, education, and household wealth. We also assessed whether the effects of the intervention varied by treatment intensity, defined by the number of testing and treatment campaigns a village received during the intervention period. These regression models included an additional triple-interaction term of survey round, intervention arm, and number of treatment rounds. In alternative models, we defined treatment intensity as a binary variable and considered a village to be “highly treated” if it had more than the median number of treatment rounds.
To explore alternative explanations for declines in malaria prevalence besides the intervention, we assessed changes in malaria-related knowledge and travel history. To test whether differences in household characteristics between intervention and control areas could cause confounding, we also examined whether there was any association between the intervention arm, survey round, and key household-level characteristics. Since the baseline and endline surveys were conducted in different months of the year, we used daily agro-climatology data produced through the Prediction of Worldwide Energy Resources project to examine changes in climate patterns in the study areas, including temperature, precipitation, humidity, and surface soil wetness [24]. All analyses were performed using Stata version 15 (StataCorp, College Station, USA).


留言 (0)