
記住我


Acute myeloid leukemia (AML) is a heterogeneous disease both in terms of genetics and clinical outcome.1 Patients can be subdivided into 3 risk groups using the European LeukemiaNet (ELN) prognostic risk classification with significantly different cumulative incidence of relapse (CIR) and overall survival (OS) rates.2 Induction therapy for patients considered fit for intensive therapy commonly starts with 2 cycles of high-dose chemotherapy. The choice of postremission therapy is based on the risk classification and measurable residual disease (MRD) status.3,4 It consists of consolidation with nonmyeloablative chemotherapy, myeloablative chemotherapy followed by an autologous hematopoietic cell transplantation (auto-SCT), or allogeneic hematopoietic cell transplantation (allo-SCT).5 Due to good tolerability, myeloablative chemotherapy (busulfan and cyclophosphamide) followed by an auto-SCT can be considered as a consolidation therapy for ELN favorable- and intermediate-risk patients who are in first complete remission and MRD negative in bone marrow (BM).6–9 While MRD assessment in BM is the standard practice, alternative sources such as autologous hematopoietic cell apheresis products (ASCAPs) are of interest, particularly when BM samples are unavailable. Studies have explored the use of MRD in ASCAP enriched with hematopoietic stem and progenitor cells (HSPCs), and possibly malignant cells, in hematological diseases like acute lymphocytic leukemia and multiple myeloma (MM),10,11 but large studies on AML are lacking.12–14 Here, we retrospectively investigated the prognostic impact of MRD detection in ASCAP on outcome in a cohort of 229 patients with newly diagnosed AML enrolled in various multicenter prospective phase III Dutch–Belgian Cooperative Trial Group for Hematology–Oncology (HOVON) and the Swiss Group for Clinical Cancer Research (SAKK) clinical trials.7,15–18 For details of MRD detection and methods, we refer to our previous publications and supplemental materials.19 To quantify MRD in ASCAP, we first verified the background events in ASCAP from 10 healthy donors and 4 pathological controls (MM patients), resulting in a total of 14 measurements for 25 leukemia-associated immunophenotypes (LAIPs). An overview of the results can be found in Suppl. Table S1. In 7 healthy donor control samples and 2 MM control samples, a phenotype mimicking an LAIP was detected above the 0.1% cutoff. In 1 sample, this was the expression of CD13+CD33− on primitive cells (both CD34+ and CD117+), with otherwise normal myeloid CD33 expression. The other 8 samples showed a phenotype mimicking the mature LAIP CD14+HLA-DR−. These 2 LAIPs were considered related to granulocyte colony-stimulating factor (G-CSF) exposure as it can promote proliferation and differentiation of hematopoietic progenitor cells, potentially affecting the reliability of mature LAIPs.20 Therefore, ASCAP samples from patients with AML who showed these LAIPs were considered MRD negative unless an alternative LAIP was also present. The G-CSF–related LAIPs were found in 8 AML specimen, for which in 3 specimen, an alternative LAIP was measured. This influence of G-CSF stimulation was not detected in BM control samples, suggesting that these LAIPs may be specific to ASCAP specimens.21
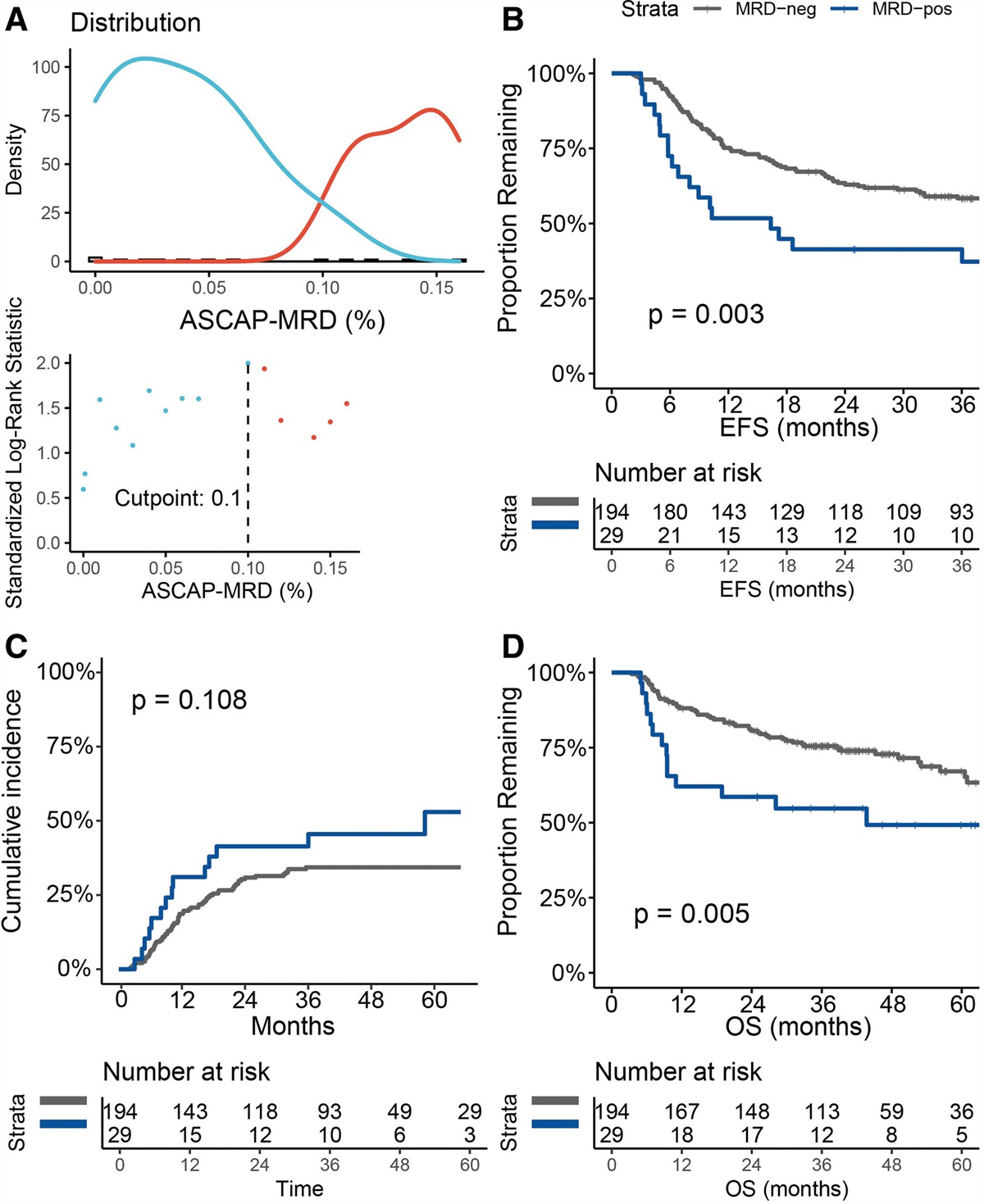
ASCAP-MRD was measured in 229 de novo AML patients of whom the sample quality was adequate to measure ASCAP-MRD in 223 specimen. According to MaxStat, the optimal cutoff was found at 0.1% LAIP of total white blood cells (Figure 1A). Using this cutoff, 29 of 223 (13%) patients were considered ASCAP-MRD positive. There were no statistically significant differences in baseline characteristics between the ASCAP-MRD–positive and ASCAP-MRD–negative patients, as can be seen in Suppl. Table S2. As expected, a substantial percentage of the patients had a favorable risk profile (55%) according to the ELN-2017 definition, as these patients are primarily selected for consolidation with auto-SCT. Moreover, patients with a positive MRD resulting in ASCAP showed a significantly higher frequency of MRD-positive BM sample (P<0.001). ASCAP-MRD–positive patients had a statistically significant worse outcome in terms of 3-year event-free survival (EFS; ASCAP-MRD positive, 41% versus ASCAP-MRD negative, 58%; P=0.003; Figure 1B). The 3-year CIR was 45% for ASCAP-MRD–positive patients compared to 32% for ASCAP-MRD–negative patients (P=0.108; Figure 1C). In addition to EFS difference, ASCAP-MRD–positive patients had a significant worse 5-year OS (ASCAP-MRD positive, 49% versus ASCAP-MRD negative, 67%; P=0.005; Figure 1D). Univariate and multivariate Cox regression analyses confirmed ASCAP-MRD as an independent prognostic factor for EFS, along with the ELN-2017 risk score and type of consolidation therapy (Suppl. Tables S3 and S4). When the MRD groups were stratified for ELN risk classification, the subgroups became small, and in general, no statistically significant differences were found (Suppl. Figure S1).
 Figure 1.:
Figure 1.: Optimal cutoff and subsequent survival differences for MRD acquired from ASCAP. (A) Cutoff determination by using maximally selected rank statistics with the highest log-rank for MRD in ASCAP measured at 0.1% LAIP cells of total white blood cells. The graph shows the density and distribution of MRD-negative patients (in blue) and MRD-positive patients (in red) according to the cutoff. (B) Using the 0.1% cutoff, 29 of 223 patients were MRD positive. These patients had a statistically significant worse 3-y event-free survival (EFS) compared to MRD-negative patients (41% vs ASCAP-MRD negative, 58%; P=0.003). (C) Three-year difference in CIR for MRD-positive patients was 45% compared to 32% for MRD-negative patients (P=0.108). (D) Difference in 5-y OS between ASCAP-MRD–positive and MRD-negative patients (49% vs 67%, respectively; P=0.005). ASCAP = autologous stem cell apheresis products; CIR = cumulative incidence of relapse; EFS = event-free survival; LAIP = leukemia-associated immunophenotype; MRD = measurable residual disease; OS = overall survival.
To exclude the type of consolidation therapy as a potential confounding factor, we performed a subgroup analysis of only patients undergoing auto-SCT. Of all patients, 84% (188/223) received an auto-SCT as first consolidation therapy, with a list of reasons for abstaining from auto-SCT provided in Suppl. Table S5. In the auto-SCT subgroup, 13% (24/188) of patients were identified as ASCAP-MRD positive, and there were no statistically significant differences at baseline characteristics between the MRD-positive and MRD-negative patients (Suppl. Table S6). The survival outcomes showed consistent results, with ASCAP-MRD positivity associated with worse EFS (46% versus 61%; P=0.012), CIR (51% versus 33%; P=0.028), and OS (58% versus 68%; P=0.029), as visualized in Suppl. Figure S2. The ASCAP-MRD status remained an independent prognostic factor in multivariate analysis, together with ELN-2017 risk classification (Suppl. Table S7).
In addition, we evaluated the concordance between MRD detection in ASCAP and BM to determine whether MRD in ASCAP offers additional prognostic value independent from MRD in BM. A paired BM specimen was acquired for MRD analysis in 185 of 223 (83%) patients, with a median time interval of 6 days (range, 0–57 days) after the ASCAP-MRD sample. As depicted in Suppl. Figure S3, BM-MRD–positive patients had statistically significant worse EFS and CIR and a trend toward worse OS compared to MRD-negative patients. This was confirmed in a multivariate model, including ELN-2017 risk classification and FLT3-ITD/NPM1 status (Suppl. Table S8). ASCAP-MRD and BM-MRD results were concordant for 172 of 185 (93%) patients, of whom 154 (83%) patients were double MRD negative, with a moderate correlation (r=0.488; P<0.001). The nonconcordant group of 13 (7%) patients consisted of 8 patients who were BM-MRD positive/ASCAP-MRD negative, with no clear cause for the discrepancy. When the double-positive, double-negative, and discrepant groups were compared based on survival, there was a statistically significant difference in EFS, CIR, and OS (Suppl. Figure S4). In a pairwise comparison, a significant difference was only found between the double-positive group and patients who were MRD negative in both specimen, for both 3-year EFS (33% versus 60%; P=0.021), CIR (50% versus 30%; P=0.041), and 5-year OS (43% versus 64%; P=0.016).
In this relatively homogeneous group of predominantly favorable-risk AML patients, MRD above 0.1% in ASCAP was associated with a worse EFS and OS. In the subgroup of patients who actually received an auto-SCT as consolidation therapy, CIR was also statistically significantly worse for ASCAP-MRD–positive patients in addition to EFS and OS. The presence of leukemic contamination in the auto-SCT graft of the 24 patients, who underwent an auto-SCT despite the presence of MRD, may have a contributory effect on the statistically higher CIR observed in comparison to ASCAP-MRD–negative patients. However, previous studies evaluating the ex vivo purging of autologous products have not shown any beneficial impact on the risk of relapse or OS, which explains the limited adoption of this approach in routine clinical practice.22 In addition, from 20 of 24 patients, also a paired BM sample was present, and 15 of 20 of these were also MRD positive. Consequently, it is more likely that a significant portion of residual disease persisted in these patients, although this remains speculative. During data collection, it was not common practice to base clinical decisions on the MRD result. However, with current knowledge, we would escalate consolidation therapy to an allo-SCT in fit MRD-positive patients, similar to the approach currently applied to ELN intermediate-risk patients.6,7,23
It is noteworthy that there was a 93% concordance between the ASCAP-MRD and BM-MRD results. This suggests that MRD assessed in ASCAP could be regarded as an alternative specimen when BM is not available. However, this has not prospectively been assessed, much like the exploration of MRD measured in peripheral blood as a possible alternative to BM. The high degree of concordance makes it difficult to interpret the discrepant MRD results (n=13), which may be attributed to various factors, including the time between the collection of ASCAP-MRD and BM-MRD.
Contrary to expectations, our data indicate that the sensitivity of MRD in ASCAP based on the relapse rate is comparable to that observed in BM, rather than being enhanced, despite the increased mobilization of leukemic cells and enrichment of HSPC through G-CSF stimulation.24,25 The impact of G-CSF on MRD reliability seems to be minimal, although healthy and nonleukemic control ASCAP samples showed higher background events compared to NBM samples.21
Limitations of our study include its retrospective nature and the lack of a universally accepted ASCAP-MRD cutoff.14 The study population predominantly consisted of patients with favorable- and intermediate-risk AML who were consolidated with an auto-SCT, limiting the generalizability of the findings to patients with unfavorable risk profiles. This study demonstrates that MRD detected above 0.1% in ASCAP is significantly associated with poorer outcomes. While ASCAP shows promise as an alternative source for MRD detection, it does not appear to enhance sensitivity compared to BM, as it yields similar results in 93% of cases. Nonetheless, when the preferred BM samples are unavailable, ASCAP may be considered for MRD assessment. Further validation studies are needed to confirm these findings and establish standardized cutoff for ASCAP-MRD positivity.
AUTHOR CONTRIBUTIONSJMT, YB, LLN, CB, AAvdL, JC, and DCdL contributed to the conception and design of the study. BTG, AAvdL, MGM, TP, GJO, and DCdL collected the data. JMT, YB, LLN, AK, and WS organized the database. JMT and YB performed the statistical analysis. JMT wrote the first draft of the manuscript. All authors contributed to manuscript revision, read, and approved the submitted version.
DISCLOSURESBTG serves as a consultant for BerGenBio, Phizer, Inc, and Novartis and holds stock options in Alden Cancer Therapy and KinN Therapeutics. MGM serves as a consultant for CDR-Life, Inc; holds stock options in CDR-Life, Inc; and has a patent licensed to the University of Zurich. GJO serves as a consultant for Novartis, Pfizer, Inc, Celgene, Janssen, Agios, Amgen, Gilead, Astellas, Roche, Jazz Pharmaceuticals, and Merus; has received honoraria from Novartis, Celgene, Agios, Gilead, and Astellas; received research funding from Novartis; and holds a membership on an entity’s Board of Directors for Roche. JC has received research funding from Takeda, DC-One, Genentech, Janssen, Novartis, and Merus. All the other authors have no conflicts of interest to disclose.
SOURCES OF FUNDINGThe authors declare no sources of funding.
REFERENCES 1. Dohner H, Weisdorf DJ, Bloomfield CD. Acute myeloid leukemia. N Engl J Med. 2015;373:1136–1152. 2. Dohner H, Estey E, Grimwade D, et al. Diagnosis and management of AML in adults: 2017 ELN recommendations from an international expert panel. Blood. 2017;129:424–447. 3. Heuser M, Freeman SD, Ossenkoppele GJ, et al. 2021 update measurable residual disease in acute myeloid leukemia: European LeukemiaNet Working Party consensus document. Blood. 2021;138:2753–2767. 4. Short NJ, Zhou S, Fu C, et al. Association of measurable residual disease with survival outcomes in patients with acute myeloid leukemia: a systematic review and meta-analysis. JAMA Oncol. 2020;6:1890–1899. 5. Cornelissen JJ, Blaise D. Hematopoietic stem cell transplantation for patients with AML in first complete remission. Blood. 2016;127:62–70. 6. Venditti A, Piciocchi A, Candoni A, et al. GIMEMA AML1310 trial of risk-adapted, MRD-directed therapy for young adults with newly diagnosed acute myeloid leukemia. Blood. 2019;134:935–945. 7. Löwenberg B, Pabst T, Maertens J, et al. Addition of lenalidomide to intensive treatment in younger and middle-aged adults with newly diagnosed AML: the HOVON-SAKK-132 trial. Blood Adv. 2021;5:1110–1121. 8. Saraceni F, Bruno B, Lemoli RM, et al. Autologous stem cell transplantation is still a valid option in good- and intermediate-risk AML: a GITMO survey on 809 patients autografted in first complete remission. Bone Marrow Transplant. 2017;52:163–166. 9. Ferrara F, Picardi A. Is there still a role for autologous stem cell transplantation for the treatment of acute myeloid leukemia? Cancers. 2020;12:59. 10. Riebl V, Dold SM, Wider D, et al. Ten color multiparameter flow cytometry in bone marrow and apheresis products for assessment and outcome prediction in multiple myeloma patients. Brief research report. Front Oncol. 2021;11:708231. 11. Merryman RW, Redd RA, Taranto E, et al. Minimal residual disease in patients with diffuse large B-cell lymphoma undergoing autologous stem cell transplantation. Blood Adv. 2022;7:4748–4759. 12. Mulé MP, Mannis GN, Wood BL, et al. Multigene measurable residual disease assessment improves acute myeloid leukemia relapse risk stratification in autologous hematopoietic cell transplantation. Biol Blood Marrow Transplant. 2016;22:1974–1982. 13. Siehl JM, Thiel E, Leben R, et al. Quantitative real-time RT-PCR detects elevated Wilms tumor gene (WT1) expression in autologous blood stem cell preparations (PBSCs) from acute myeloid leukemia (AML) patients indicating contamination with leukemic blasts. Bone Marrow Transplant. 2002;29:379–381. 14. Feller N, Jansen-van der Weide MC, van der Pol MA, et al. Purging of peripheral blood stem cell transplants in AML: a predictive model based on minimal residual disease burden. Exp Hematol. 2005;33:120–130. 15. Randomized study to assess the added value of laromustine in combination with standard remission-induction chemotherapy in patients aged 18-65 years with previously untreated acute myeloid leukemia (AML) or myelodysplasia (MDS) (RAEB with IPSS ≥ 1.5). EU Clinical Trials Register. Available at: https://www.clinicaltrialsregister.eu/ctr-search/trial/2008-000404-92/NL. Published 2008. Accessed January 14, 2022. 16. Löwenberg B, Pabst T, Maertens J, et al. Therapeutic value of clofarabine in younger and middle-aged (18-65 years) adults with newly diagnosed AML. Blood. 2017;129:1636–1645. 17. Terwijn M, van Putten WL, Kelder A, et al. High prognostic impact of flow cytometric minimal residual disease detection in acute myeloid leukemia: data from the HOVON/SAKK AML 42A study. J Clin Oncol. 2013;31:3889–3897. 18. Janssen J, Löwenberg B, Manz M, et al. Inferior outcome of addition of the aminopeptidase inhibitor tosedostat to standard intensive treatment for elderly patients with AML and high risk MDS. Cancers. 2021;13:672. 19. Zeijlemaker W, Kelder A, Cloos J, et al. Immunophenotypic detection of measurable residual (stem cell) disease using LAIP approach in acute myeloid leukemia. Curr Protoc Cytom. 2019;91:e66–e66. 20. Kovtonyuk LV, Manz MG, Takizawa H. Enhanced thrombopoietin but not G-CSF receptor stimulation induces self-renewing hematopoietic stem cell divisions in vivo. Blood. 2016;127:3175–3179. 21. Hanekamp D, Bachas C, van de Loosdrecht A, et al. Re: myeloblasts in normal bone marrows expressing leukaemia-associated immunophenotypes. Pathology (Phila). 2020;52:289–291. 22. Feller N, Kelder A, Westra G, et al. Positive selection for CD90 as a purging option in acute myeloid leukemia stem cell transplants. Cytometry Part B. 2008;74B:9–16. 23. Gorin NC, Giebel S, Labopin M, et al. Autologous stem cell transplantation for adult acute leukemia in 2015: time to rethink? Present status and future prospects. Bone Marrow Transplant. 2015;50:1495–1502. 24. Konopleva M, Benton CB, Thall PF, et al. Leukemia cell mobilization with G-CSF plus plerixafor during busulfan–fludarabine conditioning for allogeneic stem cell transplantation. Bone Marrow Transplant. 2015;50:939–946. 25. Uy GL, Rettig MP, Stone RM, et al. A phase 1/2 study of chemosensitization with plerixafor plus G-CSF in relapsed or refractory acute myeloid leukemia. Blood Cancer J. 2017;7:e542–e542.
留言 (0)