
記住我



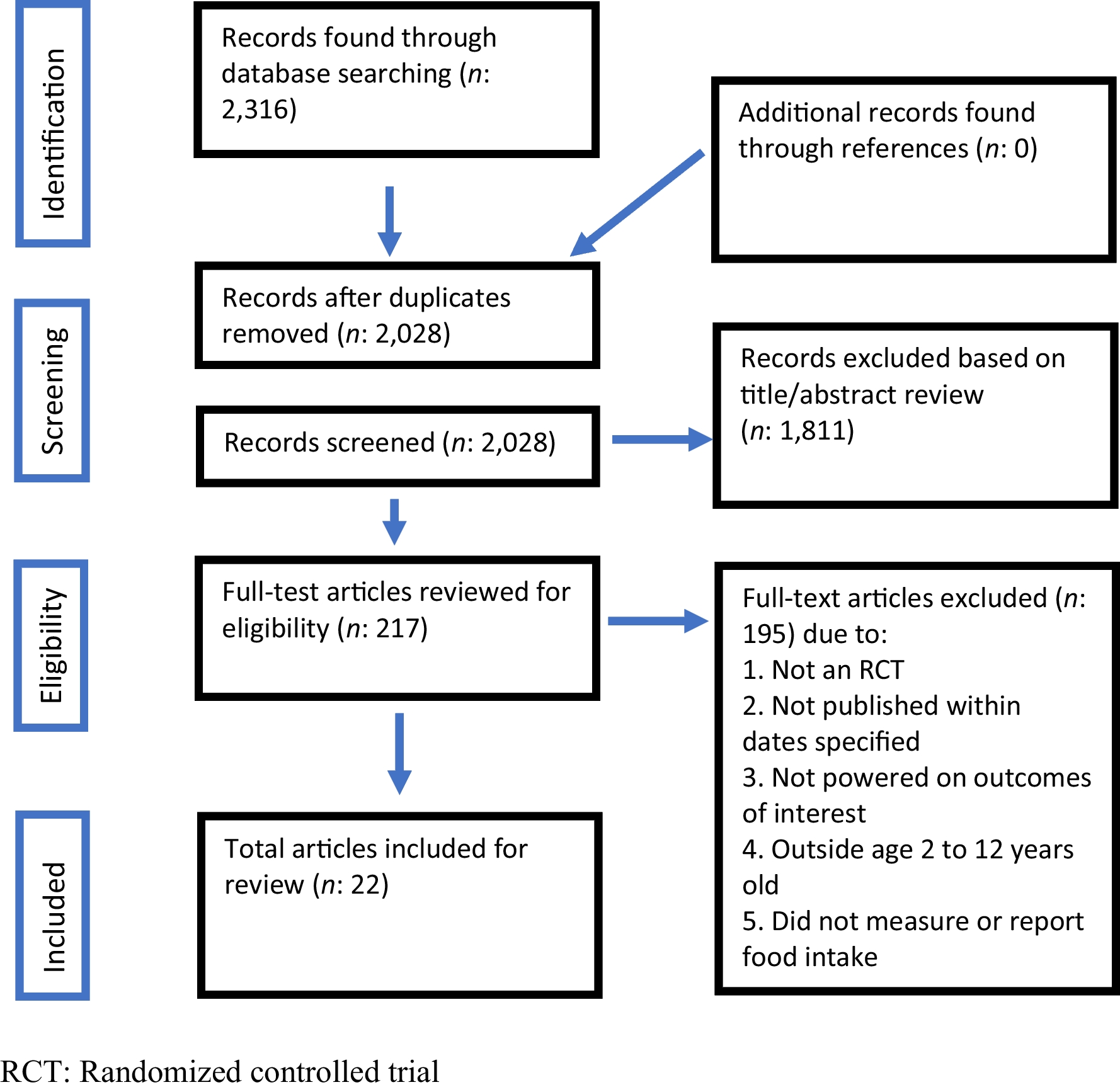





A total of 110 relevant articles were identified during the selection process. Fifteen duplicated records and 17 irrelevant topics were removed. After screening and assessing eligibility, the final 17 studies were included in this systematic review. A flow diagram of the selection process is shown in Fig. 1.
Fig. 1
Flow diagram of the study selection
General overviewArticles related to the rehabilitation of patients with SCI were collected according to the criteria mentioned above, and 17 papers were derived. To precisely analyze exercise protocols, 12 electronic- and robot-based papers and 5 conventional types of rehabilitation articles were classified. This was examined by dividing the number of study participants by average age, duration of injury (years), level of injury (C1–T12), exercise design, research purpose, assessment, and results. The table of research results is presented in Table 1.
Table 1 Characteristics of the studies using robotic- and electronic-based rehabilitationRobotic- and electronic-based rehabilitationTwelve publications discussed electronic and robotic therapies for the survivors of SCI. For the systematic analysis, rehabilitation devices and methods were classified into functional electronic stimulation (FES) and robotic and locomotor training (LT).
Functional electrical stimulation rehabilitationSix articles [1, 2, 3, 4, 5, 6] employed FES rehabilitation using rowing, cycling, and ergometers. FES rowing training (FESRT) was covered in four studies [1, 2, 3, 5]. Afshari et al. (2022) [1] assessed the effects of FESRT on the body composition profiles in the subacute phase of SCI. This clinical trial involved a hybrid exercise involving the upper and lower limbs, which required more muscular activity. Following a substantial increase in total and leg lean mass (p < 0.05), FESRT contributed to a greater exercise ability and a propensity for reduced body fat accumulation. Vivodtzev et al. (2020) [2] instructed patients with high-level SCI (T3–C4) to undergo a whole-body FES rowing protocol with noninvasive ventilation. After 3 months of training, the participants showed an improvement in their capacity to take up oxygen for certain ventilations. Chou et al. (2020) [3] and Kim et al. (2014) [5] employed rowing exercise interventions in the survivors of SCI. This protocol led to improvements in the patients’ motor function and body composition. Gorgey et al. (2019) [4] and Thrasher et al. (2013) [6] focused on the lower extremities using FES cycling and ergometry. Gorgey et al. (2019) [4] confirmed that FES lower limb cycling had positive effects on cardiometabolic results and aerobic fitness. Similarly, Thrasher et al. (2013) [6] designed FES leg cycle ergometry training to compare patients with incomplete and complete SCI. Following 40 exercise sessions, the researchers noted improvements in the power output of the lower extremities and fatigue test.
Robotic and locomotor trainingOf the selected articles, six studies [7, 8, 9, 10, 11, 12] used LT as a rehabilitation program for patients with SCI. Onushko et al. (2019) [7] attempted to determine how sympathetic–somatomotor (SS) coupling in individuals with incomplete SCI (iSCI) can be affected by high- and low-intensity LT. In their study, the participants performed stepping tasks during 20 sessions for 4–6 weeks. The researchers discovered that high-intensity training might outperform low-intensity training, indicating that SS coordination in individuals with iSCI may change depending on the intensity of the intervention. Similarly, Leech et al. (2016) [8] evaluated the effects of exercise intensity on walking function and quality. They also found that high-intensity LT resulted in more favorable outcomes in terms of gait speed and muscle activity than low-intensity LT. Leech and George (2017) [9] employed a high-intensity LT program in patients with iSCI and noted that physical indicators (e.g., serum brain-derived neurotrophic factor, insulin-like growth factor-1) were enhanced following the intervention. Consequently, both studies reported that higher LT intensities were associated with greater improvements in patients with iSCI. Martinez et al. (2018) [10] also revealed that a body weight-supported treadmill using Lokomat® (Hocoma) improved locomotor function, including the motor score of the lower limb and balance. Gorman et al. (2019) [11] also used Lokomat® to assess and compare cardiorespiratory effects. The initial robotic session lasted 20 min and was subsequently extended in 5-min increments in future sessions until the exercise lasted 45 min. Each session began with a 5-min warm-up, followed by personalized, trained gait exercises, and finished with a 5-min cool-down. Peak VO2 level measured using robotic treadmill ergometry statistically improved (14.7%, p = 0.03) during the period of the robotic intervention. In a study by Francisco et al. (2017) [12], 10 individuals with chronic cervical SCI underwent robot-assisted arm training. They performed single-degree-of-freedom upper limb exercises to demonstrate the feasibility, tolerance, and efficacy of MAHI Exo-II for cervical SCI. This device is an electronically operated upper extremity haptic exoskeleton appliance developed for rehabilitation. The treatments were modified based on the movement ability of each joint. After robotic intervention, arm and hand functions (Jebsen-Taylor Hand Function Test, Action Research Arm Test) were improved. In addition, it was found that both trainings using robots improved the targeted physical function.
Conventional rehabilitationBased on the abovementioned criteria, traditional rehabilitation methods for patients with SCI are categorized into resistance training, balance task, aerobic exercise, and mixed training. Five articles [13, 14, 15, 16, 17] were used for the systematic analysis. The table of research results is presented in Table 2.
Table 2 Characteristics of the studies using conventional methods (resistance, balance, aerobic training)Resistance trainingSilva et al. (2020) [13] studied the effects of circuit resistance training (CRT) in individuals with SCI. The participants consisted of patients with chronic SCI, primarily those with injury levels from T4 to T11. CRT protocols involved physical and motor abilities (e.g., frontal lift, agility station, biceps curl). The interventions consisted of activities that were easy for patients to follow in their daily routine and could be performed directly in a wheelchair. After 12 weeks of exercise, although there were no differences in bone-related indicators, the patients’ muscle strength (p = 0.028) and agility (p = 0.028) improved.
Balance trainingSadeghi et al. (2018) [14] used rebound therapy for spinal cord rehabilitation. This intervention involves exercising on a trampoline to improve static stability. The participants performed core stability training and upper extremity exercises on a trampoline and several basic exercises using instruments, such as balls and balloons. After the participants practiced the exercises thrice a week, rebound therapy was found to have a positive effect on several standing stability parameters (p < .01).
Aerobic trainingAerobic training for patients with SCI has been addressed in studies by Wouda et al. (2016) [15] and DiPiro et al. (2016) [16]. Wouda et al. (2016) [15] aimed to determine whether high-intensity interval training (HIIT) increases physical capacity and fitness levels more than moderate-intensity training (MIT) and standard care. The two experimental groups were trained for 12 weeks at intensities of 70% (MIT) and 85–95% (HIIT) of HRmax. The intervention program consisted of jogging or running according to the patient’s fitness level and physical condition. The results showed no differences in effectiveness among the three groups (i.e., HITT, MIT, and standard care). DiPiro et al. (2016) [16] also used an aerobic exercise training (AET) program for iSCI. Ten patients were instructed to perform a non-task-specific, voluntary, progressive AET protocol. The researchers discovered significant improvements in aerobic and locomotor capacities.
Mixed trainingLotter et al. (2020) [17] identified the effects of task-specific therapies compared with impairment-based therapies on gait performance. Impairment-based training includes non-walking training, whereas the task-specific method involves training involving rehabilitation approaches (e.g., strengthening, balance, and aerobic exercise). Weight machines were used for the strengthening activities. During balance training, patients performed standing or sitting activities on unbalanced surfaces (e.g., foam, trampoline) or dual upper limb balance tasks. Aerobic exercise involved cycling or stepping (e.g., NuStep LLC). The protocol consisted of 20 sessions over 6 weeks, with the intensity set at 70–80% HRmax. The researchers found that task-specific training had a positive effect on the determinants of mobility capacity.
留言 (0)