
記住我
What is known about the topic?
Critically ill patients are commonly affected by pressure injuries, which is considered a health care-related adverse event. The implementation of multicomponent prevention programs based on scientific evidence is associated with a reduced occurrence of pressure injuries.What does this article add?
Best practice implementation for ICU pressure injury prevention in the context of the COVID-19 pandemic. Use of monitoring cameras in care audits. Education and engagement strategies for raising awareness among multiprofessional teams can improve compliance. IntroductionA pressure injury is localized damage to the skin and/or underlying soft tissue, usually over a bony prominence or related to a medical device; it may present as intact skin or an open ulcer and results from intense and/or prolonged pressure combined with shear.1
Pressure injuries are considered a global public health problem and have been widely discussed as preventable healthcare-related adverse events. Pressure injury prevention should be addressed carefully, especially among those who are at greater risk because of clinical, hemodynamic, or mobility conditions.1,2
Data from a systematic review on the prevalence and incidence of pressure injuries in ICUs showed that the cumulative prevalence of pressure injuries in adult critically ill patients ranged from 16.9 to 23.8% and that the cumulative incidence ranged from 10 to 25.9%.2 During the COVID-19 pandemic, the number of pressure injury cases increased significantly because of the virus pathophysiology, overloaded healthcare systems, limited material and human resources, increased number of hospitalizations in ICUs, and the severity and instability profile of patients with COVID-19.3
Pressure injury prevention in ICUs has been widely discussed,4–6,12 with studies primarily addressing aspects related to instability and severity. The COVID-19 pandemic has further broadened the discussion on the topic, raising more issues about the occurrence of unavoidable pressure injury.7 Although the scientific literature already discusses some unavoidable pressure injuries, no clear and easily applicable criteria in clinical practice are currently available to define the occurrence of unavoidable pressure injuries. Furthermore, there is a lack of robust research on the contraindication of some preventive measures given the patient's severity, such as repositioning a critically unstable patient.
Considering the magnitude of pressure injury-related problems, various preventive interventions have been studied, including the following best practice recommendations for critically ill patients summarized by JBI8:
evaluating patients using a valid and reliable tool such as the Braden scale to determine their pressure injury risk and developing a prevention plan (grade A); performing patient nutritional screening using a tool and setting calorie goals for those at risk of pressure injury (grade A); conducting multiple multiprofessional preventive interventions for patients at risk of developing pressure injuries, such as frequently repositioning/changing decubitus at least every 2 h, using support surfaces (low pressure or memory foam or alternating pressure for those at high risk/very high risk) and prophylactic dressings (silicone foam) and performing nutritional assessment and intervention and skin integrity assessments (grade A); educating patients and their families/caregivers about the risks and strategies for pressure injury prevention and treatment (grade A); inspecting the skin and locations where healthcare devices are attached to the patient within 2 h of admission to the ICU and with each repositioning and shift change for the presence of signs of pressure injury (grade B); slowly and gradually repositioning critically ill and unstable patients to enable hemodynamic and oxygenation stabilization. The body position of highly unstable critically ill patients should be changed frequently but only slightly to maintain a repositioning program and to complement regular repositioning (grade B).Although the hospital examined in this study had a pressure injury prevention protocol, pressure injuries increased during the COVID-19 pandemic. Before the pandemic, the prevalence of pressure injuries in the institution was approximately 5% (March 2020). During the pandemic, however, the prevalence of pressure injuries reached 15.7% (December 2020). This considerable increase led us to develop a best practice implementation project for pressure injury prevention.
Objectives GeneralThis study assessed compliance with best practices for pressure injury prevention in patients admitted to the ICU of a tertiary hospital in São Paulo, Brazil.
Specific Identifying barriers to and strategies for implementing best practices for pressure injury prevention in critically ill patients. Identifying healthcare professionals’ knowledge and beliefs about pressure injury prevention care in ICU patients. MethodsThis evidence implementation project used the JBI method9 whose framework is based on an audit and feedback process, along with a structured approach to identify and manage barriers to compliance with clinical best practices. The model involves the following steps: step 1, establishing a working group and conducting the baseline audit according to evidence-based criteria; step 2, reviewing the results from the baseline audit and defining and implementing strategies for noncompliant items using the Getting Research into Practice (GRiP) tool; step 3, conducting a follow-up audit to assess the results of the interventions to identify any issues in clinical practice and improve them in subsequent audits.
The project was approved by the Research Ethics Committee (Comitê de Ética e Pesquisa; CEP) of the Hospital under opinion number 4.581.515. All measures were taken to preserve the confidentiality and anonymity of the audit participants.
Study areaThe project was implemented in the adult ICUs of a tertiary hospital with 523 beds located in São Paulo, Brazil. The units have 54 adult ICU beds, divided into six wings. However, because of the COVID-19 pandemic, the number of beds increased temporarily during the project. During this period, the ICUs had 85 beds, distributed in 10 wards, with seven wards for patients with COVID-19. Four wards were chosen for the project – two for COVID-19 patients and two for non-COVID-19 patients – totaling 56 audited patients. Approximately 400 professionals – including nurses, nursing technicians, physiotherapists, nutritionists, and physicians – worked in these units.
Step 1: Establishing the working group and conducting a baseline auditThe project was conducted by three nurses: a stomal therapist with extensive knowledge on the central theme of the project; a practice development nurse focused on formulating strategies for raising awareness and training the working group; and a critical care nurse focused on process alignments and improvements throughout the implementation. The core team consisted of three nursing managers, a medical manager, and a coordinator; two nursing coordinators, one from physiotherapy and the other from nutrition; four care leaders; two practice development nurses; two stomal therapists; and 14 healthcare professionals, members of the skin reference group (called “Skin Champions”). The activities of the core team are described below:
1) Managers and coordinators: providing administrative support and approving implementation strategies. 2) Care leaders: helping in the engagement of the local team, scheduling training, and supporting the development and approval of implementation strategies. 3) Practice development nurses and stomal therapists: helping in the audits, compiling data, and training staff. 4) Skin Champions: Multidisciplinary team, active since mid-2018, working to support prevention activities in their units. In this project, the group worked on designing and implementing improvements as well as training staff and disseminating practices. 5) The baseline audit took place between May and June 2021, and the follow-up audit was carried out in October 2021. In both audits, care was observed in two steps: an indirect observation of care using monitoring cameras placed in the beds; and a direct observation at the bedside, followed by a retrospective analysis of the medical records to assess compliance with the JBI criteria.During the baseline audit, the unit managers helped us to inform all ICU professionals about the start of the project and disseminate research on difficulties in preventing pressure injuries faced in clinical practice and on the multidisciplinary team's knowledge on the subject. We administered two questionnaires using the Google Forms application to assess the pressure injury prevention knowledge, beliefs, and values of the entire multidisciplinary team in the ICUs. The knowledge questionnaire was administered after we adapted some vocabulary from the questionnaire used by Pieper and Mott; it was validated in Brazil by Fernandes, Caliri, and Hass.10 Healthcare professionals who refused to sign the informed consent form or who were on vacation or sick leave during the data collection period were excluded from this research on knowledge, beliefs, and values.
During the baseline audit, the core team was made aware of the relevance of this work using strategies such as brainstorming for generating and sharing ideas for change organized in a diagram.
During this period, Brazil had a high number of people infected with COVID-19, and 100% of ICU beds were occupied, 42% by patients with COVID-19.
To the nine criteria recommended by JBI,8 we added a tenth criterion addressing whether the patients remained with floating heels, in line with international guidelines for preventing calcaneus pressure injury,1 an ongoing problem in the institution.
The audit criteria, sample, and method for measuring compliance with best practices are summarized in Table 1.
Table 1 - Audit criteria, sample, and method for measuring compliance with pressure injury prevention in critically ill patients Audit criteria Sample Method for measuring compliance (%) with best practices 1. Patients are assessed using a valid and reliable tool to determine their risk of PI and inform the development of a prevention plan. Patients:The results from the baseline audit and assessment of the pressure injury prevention knowledge, beliefs, and values of the ICU multidisciplinary team were compiled. The GRiP tool made it possible to identify barriers and develop strategies to overcome them. The results were presented to specialization managers, coordinators, and leaders during four meetings held on Microsoft Teams and lasting 1 h each. After the managers were briefed on the implementation strategies, four more meetings were held, this time in person with the Skin Champion team, to present the results of the first phase and to define strategies for increasing compliance with best practices, gaining support for the change in practices, and fostering engagement. In all meetings, we sought to motivate the team in their search for the knowledge, know-how, and willingness. For this purpose, personalized invitations were sent, and reflections on the problem, patient testimonials, and cost surveys related to injuries developed in the institution in question were presented to the team to promote reflection on incorporating the practices into the care routine. The GRiP strategies are described in the Results section.
Step 3: Follow-up audit after change strategy implementationThe follow-up audit used the same criteria as those used in the baseline audit. The sample had the same number of patients (28), totaling 56 patients before and after best practice implementation. The profile of the patients treated at the participating ICUs changed because, given the decreasing number of new COVID-19 cases, the ICU that was initially intended to treat COVID-19 patients only was transformed into a general ICU, treating patients with other diseases.
AnalysisThe data were analyzed via automatic reporting using JBI PACES software. A descriptive analysis of the data on the professionals’ knowledge, beliefs, and values was performed using a Microsoft Excel spreadsheet, calculating the percentages of hits in each answer.
ResultsThe results are presented according to the different steps of the project.
Step 1: Baseline auditThe results of the baseline audit are presented in the graph shown in Fig. 1, using PACES version 0.0.11/2021 (JBI, Adelaide, South Australia, Australia).
 Figure 1:
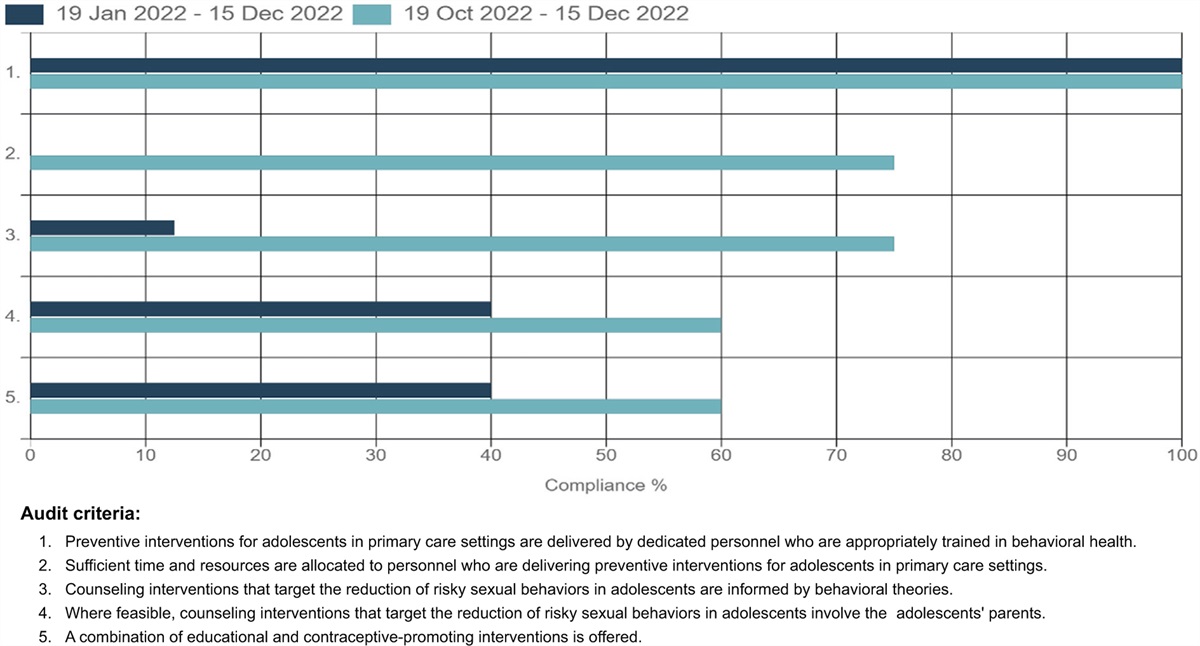
Figure 1: Rate of compliance with best practice criteria for pressure injury prevention at the baseline audit (%). São Paulo, 2021.
None of the audited criteria reached 100% compliance. Criterion 1 had the highest percentage of compliance (93%). The criterion with the lowest compliance in the baseline audit was criterion 9, related to patient and family/caregiver education on risks, prevention strategies, and pressure injury management, with 20% compliance.
Criteria 6 and 8 reached 72 and 78% compliance, respectively. Criteria 4 and 5 related to nutritional assessment (criterion 4) and caloric goals showed 68 and 57% compliance, respectively.
Criterion 10, which assesses the proper positioning of the calcaneus, had 50% compliance, and repositioning stable patients at risk of developing pressure injuries at least every 2 h (criterion 7) had 37% compliance.
Data related to skin assessment include two criteria: whether patients undergo skin assessment, including inspection of areas with devices within 2 h of admission to check for signs of pressure injury (criterion 2) and whether this assessment is repeated at every repositioning and every shift change to check for signs of pressure injury (criterion 3). The compliance rates were 57% for criterion 2 and only 29% for criterion 3.
The results derived from the 223 responses about knowledge, beliefs, and values show that 71% of the participants claimed to have some type of knowledge about pressure injury prevention. Most (62%) participants believed that adherence to the pressure injury prevention protocol in ICUs was adequate, and 74% of the participants stated that pressure injury prevention measures were clear and well disseminated. In the individual analysis, 66% of the sample reported having adequate adherence to prevention protocols.
On pressure injury prevention in ICU patients, 78% of the healthcare professionals understood that these lesions were avoidable, and 92% believed that the use of protective dressings was an effective tool for reducing the risk of developing a pressure injury. Regarding the mobility of critically unstable patients, 64% of the healthcare professionals stated that repositioning in bed was possible, 30% denied this possibility, and 6% did not express an opinion.
The main limitation identified by the participants was other staff members’ difficulty in adhering to pressure injury preventive measures (28.7%), followed by the lack of time caused by the excessive number of activities (26.4%), and insufficient knowledge about prevention strategies specifically aimed at critically ill patients (14.8%). Other difficulties listed by the healthcare professionals included the hemodynamic instability of patients (11.2%), the unavailability of human resources (9.4%), the low achievement rate of nutritional goals (0.9%), patient nonadherence with proposed actions (0.9%), lack of participation by nurses (0.4%), and lack of interest among leaders (0.4%). When healthcare professionals were asked about the education strategies that should be followed for pressure injury prevention in critically ill patients, 66.4% listed quick educational actions within the ICU, 39% indicated face-to-face training, 31.8% proposed keeping brochures at the bedside or in ICU discussion groups, and 23.8% suggested distance training.
Step 2: Best practice implementation and strategies for overcoming barriersThe barriers, GRiP strategies, and results of the changes are described in Table 2.
Table 2 - Expected barriers and strategies for implementing best practices in pressure injury prevention, related to work process Barrier Strategy Resources Outcomes Delay in starting the project and implementing improvements because of the COVID-19 pandemic Raising the awareness of ICU managers and coordinators of multidisciplinary teams by presenting the project and contextualizing the problem Virtual meetings were held with leaders of the multidisciplinary team using Microsoft Teams. The leaders were authorized to start the project after reasonably balancing changes resulting from the pandemic and a commitment to help meet managerial and educational demands. Multiprofessional team resistant to best practice implementation Four awareness-raising meetings with the Skin Champions team to present the project and ideas for improving practiceRaising the teams’ awareness of the importance of patient and family education in PI prevention during training sessions
A prototype for patient/family education was built and sent to the marketing department to develop adequate material according to institutional standards The marketing department is continuing the project. Absence of care guidelines for repositioning unstable patients Meeting with the leaders of the ICUs and with multiprofessional team to design guidelines for bedside decision-making. The Lucidchart digital platform was used to develop the guideline An unstable patient mobilization algorithm was designed.The training was incorporated into the training program for new staff.
High number of recently hired ICU professionals (pandemic) “No-pressure workshop.” “No-pressure workshop,” a 1 h, hands-on meeting for disseminating PI prevention best practices through realistic simulation and storytelling Approximately 70 meetings were held to train 81% of the healthcare professionals (nurses and physical therapists). Unavailability of pillows for repositioning Presentation to leaders on evaluation of materials available on the market and benchmarking with other services.The postimplementation follow-up audit was conducted from 4 October to 12 October 2021, with 28 patients, as in the baseline audit. Unlike the baseline audit, however, the follow-up audit required the inclusion of patients from another wing of the ICU, given the low occupancy of the project wards. In addition, the patient profile changed from patients with COVID-19 to patients with other conditions.
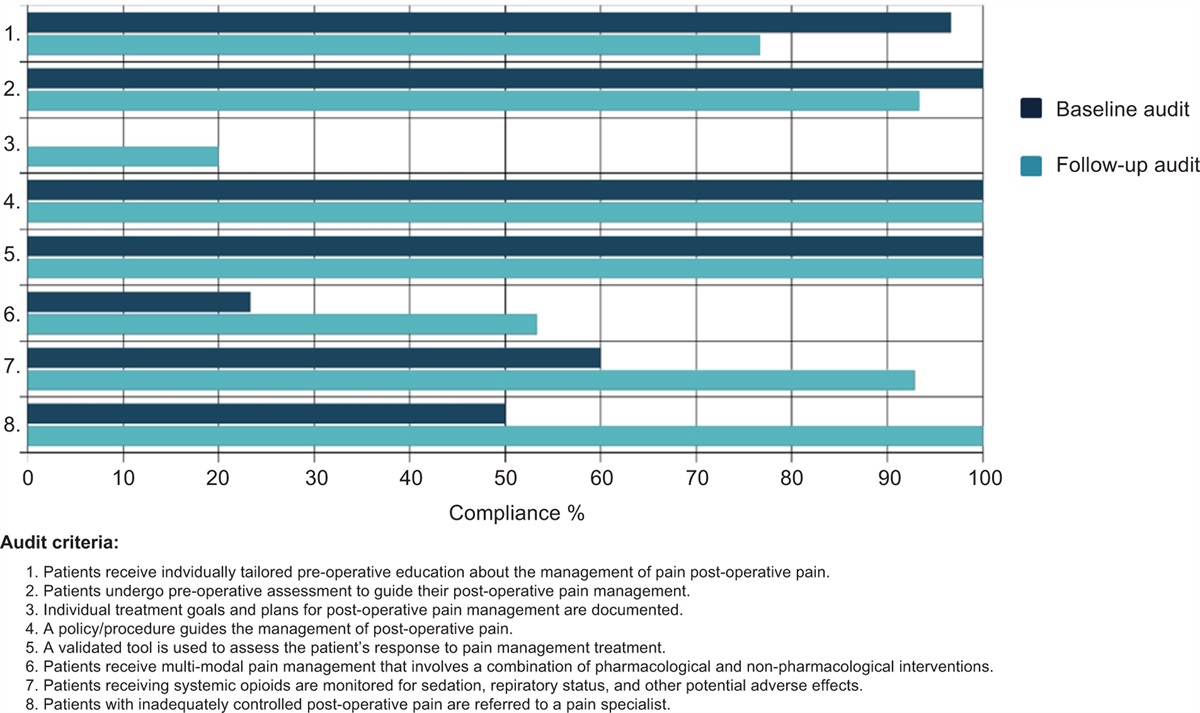
The results regarding compliance with pressure injury prevention best practice criteria from the follow-up audit, with a comparison with the data from the baseline audit, are presented in Fig. 2.
 Figure 2:
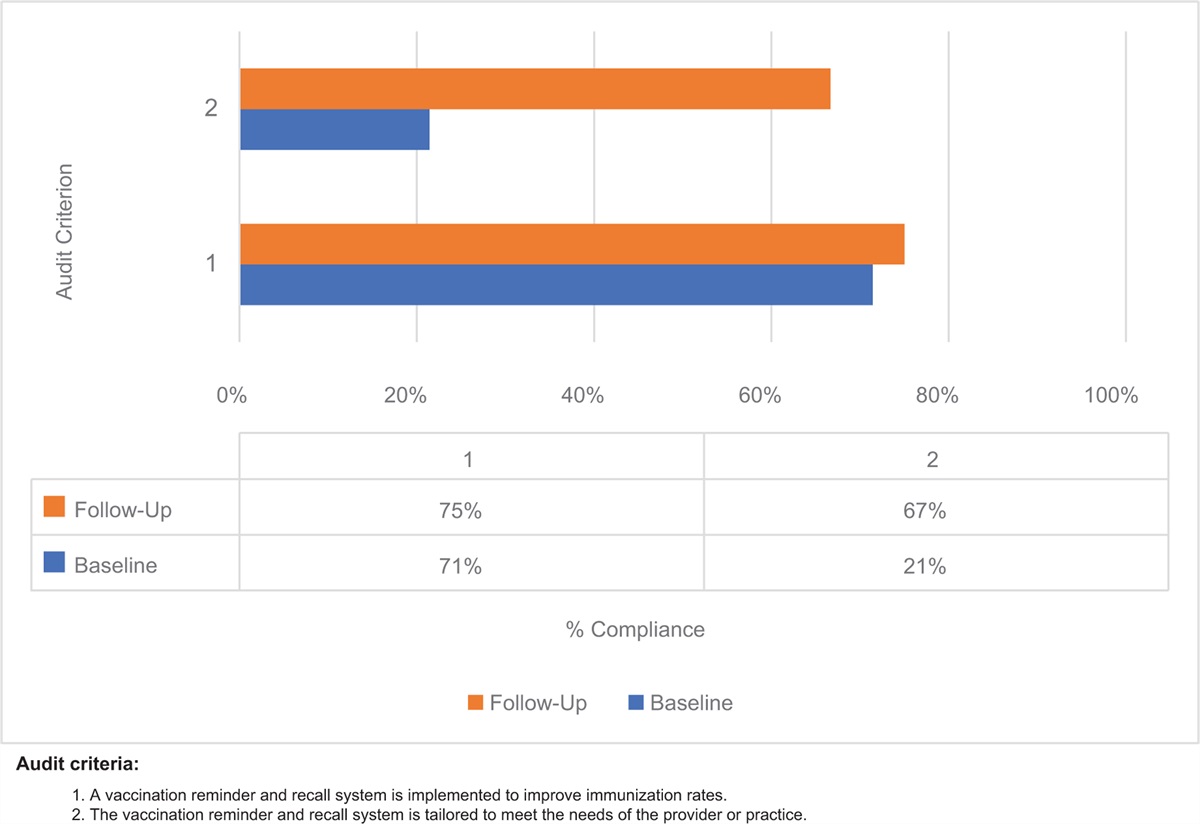
Figure 2: Rate of compliance with best practice criteria for pressure injury prevention in baseline and follow-up audits (%).
Compliance increased across all best practice criteria for pressure injury prevention. Two criteria (1 and 8) reached full compliance (i.e. 100% compliance) in the follow-up audit. Compliance with criterion 6 increased from 10 to 82%. Criteria 4 and 5 attained 76 and 85% compliance, respectively. Criteria 7 and 10 reached 58 and 73% compliance. The data on criterion 2 showed 80% compliance, while criterion 3, which includes the inspection of areas with devices, showed 50% compliance. Criterion 9, which addresses patient and family education, had the lowest compliance rate in the follow-up audit (21%). Corresponding to the improvement in adherence to best practices, the general indicator of pressure injury prevalence in the institution decreased by approximately 50% between the month preceding the implementation (June 2021; 13.2%) and the last data collection after implementation (November 2021; 6.7%). In addition, the most serious pressure injury indicator decreased significantly, more than or equal to the decrease in step 2, from June to November. This corresponds to the period before and after project implementation, from June 2021 (12%) to November 2021 (4.1%), as shown in Fig. 3.
 Figure 3:
Figure 3: ICU-acquired pressure injury prevalence indicator (%).
DiscussionAlthough the study hospital had a pressure injury prevention culture and 96% of the healthcare professionals reported having knowledge on the subject, the findings of the baseline audit showed a low rate of compliance with several criteria, demonstrating weak adherence to preventive strategies.
Among the 10 audited criteria, only criterion 1, related to the use of a validated pressure injury risk assessment tool, showed high compliance. The risk assessment tool is applied daily using the Braden scale in addition to several other interventions in the nursing therapeutic plan, which contributed to the level of compliance.
However, the criteria regarding the required completion of electronic medical records, such as criteria 2 and 4 – which involve recording the skin assessment within 2 h of admission to the ICU and the nutritional assessment using a validated tool, respectively – showed low compliance. The analysis of this low compliance showed that the skin assessment was not included in the new electronic medical patient record in the nursing physical examination and that the nutritional assessment was performed by nutritionists but was not visible to the multidisciplinary team. With the assistance of the IT staff, the electronic record templates and nutritional assessment reports were adjusted, and the team was retrained. In a recent implementation project11 on pressure injury prevention in patients with lung disease conducted in Taiwan, these criteria showed better compliance than in our study because problems related to electronic medical and information records limited our ability to achieve better results.
A key activity in ICUs is the mobilization of unstable patients. Although 64% of the healthcare professionals stated that they believed that unstable patients could be mobilized, many professionals reported discomfort and difficulty in performing the mobilization of critically ill patients because of the absence of clear criteria on indications, contraindications, and how to perform this care. Such data corroborate the low compliance with the criteria related to repositioning (criteria 3, 7 and 10) (Appendix I, https://links.lww.com/IJEBH/A106).
The barriers identified by the team about this issue are in line with the scientific literature, which still lacks practical recommendations for unstable patient mobilization. However, several recommendations are already available, mainly addressing slow and gradual mobilization.1,12
On the basis of this result, a repositioning decision-making algorithm for cases of serious or potentially fatal risks in patient handling was developed by the team, with evidence-based care recommendations.12 As the algorithm was still under development, in the audit, criterion 7 was deemed not applicable to unstable patients at fatal risk for repositioning, who were hence removed from the total sample of patients for this criterion.
After the preliminary version of the algorithm was prepared, the algorithm was PDSA-tested by ICU specialists and applied in a simulated environment. Currently in its final validation step, the algorithm will be made available in the ICU beds, and the teams will be trained in its use. The idea of designing the algorithm with the multidisciplinary team aimed at engaging them because the decision to reposition an unstable patient encompasses the entire care team, and at least five professionals are required at the bedside to reposition a patient, an operation that relies heavily on the expertise of nurses, physicians, and physical therapists.
Another strategy for improving compliance with criterion 7 was the repositioning schedule, which was implemented at the bedside and updated by employees with each change in position. The material was prepared using low technology; however, the adherence of the teams was low. For this reason, in agreement with the local managers, this pilot was discontinued.
To optimize the use of mattresses appropriate to the patient's risk, all mattresses in the institution were identified in order to relocate those indicated for patients at high risk of pressure injury, which was not possible for logistical reasons. After meetings were held on the subject, the manager purchased new mattresses, to be made available in early 2022.
The criterion with the lowest compliance in both audits was patient and family education on the risk of pressure injuries. The practice was considered compliant when the electronic medical records showed that patients, family members, and caregivers had been educated on the risks, prevention strategies, and management of pressure injuries. Despite the institutional form for planning education and hospital discharge preparation, we identified nonadherence to this process in intensive care.
Including the patient and family in care is known to improve safety and adherence to hospital risk mitigation measures.13 Thus, in addition to focusing on this issue in training and retraining on the importance of recording education in the discharge plan, a patient and family education folder was prepared at the request of the care team (Appendix II, https://links.lww.com/IJEBH/A107). The layout by the marketing team and content validation by the patient experience team are currently being finalized. After this process, the folder will be made available in electronic format on the patient portal. A key point of the audit in the COVID-19 ward was that criterion 9 was not applicable because no companion was allowed and the patients were sedated.
Educational interventions are known to be crucial for promoting improvements in hospitals. Our findings are in line with the scientific literature, which indicates divergent pressure injury prevention knowledge and attitudes.14 In light of this evidence and in view of the findings of the baseline audits, the working group focused most of its actions on raising awareness of all stakeholders and on the collective development of risk-mitigation measures and adherence to prevention measures.
Considering these interventions, the results of the follow-up audit showed improvements in all audited criteria, but there is still a long way to go before reaching at least 80% compliance with all recommended items.
A strength of this implementation project was the use of video cameras to observe most practices, especially the critical patient repositioning routine. The images were retrospectively audited, and 8 h of care were monitored for all 56 patients, totaling 448 h of observation. This is an innovative process, given the possibility of capturing and analyzing large volumes of observations and minimizing bias arising from direct inspection, such as having another professional observing the care, which can change practice; this tendency of some people to work harder and perform better when they participate in an experiment and know they are being audited/observed is known as the “Hawthorne effect.”15 The health literature does not often cite the use of continuous remote video auditing to improve quality, but a clear and long-term observation of the clinical setting ensures the reliability of the findings, in both the baseline and follow-up audits.
As a lesson learned during the pandemic, we underscore the use of technological resources to connect patients with their families, because of the imposed isolation, and of teleservices to reduce the number of professionals in direct contact with the patient. In a study conducted in a large United States hospital,16 the nursing team evaluated wounds using teletechnology in iPad form, thereby identifying pressure injury trends and patterns and introducing real-time care adjustments. Thus, in this implementation project, we highlight the key role of technological resources in supporting patient evaluation and care audits, with as little bias as possible.
LimitationsThe COVID-19 pandemic was the main limiting factor of this project because we were experiencing one of the largest pandemics in history while conducting this study. During this period, healthcare professionals were inevitably overworked, patient and care profiles changed, and no family members or companions were allowed in the ICU, among many other new contributing factors. Coupled with all these issues, frontline employees experienced several emotional impacts, burnout, physical exhaustion, worsened sleep quality, and higher stress levels, aspects that can adversely impact their performance, as described in the scientific literature.17
ConclusionThis project was implemented during one of the largest pandemics in modern history, which was the main challenge faced by the implementation team. The results demonstrate that the JBI implementation model improved adherence to best practices in pressure injury prevention among critically ill patients. This increased adherence to recommended practices and implemented innovations decreased pressure injury prevalence indicators and their severity at the institution. These findings confirm that providing evidence-based care improves care quality and minimizes healthcare risks. Future audits will be required to review and improve compliance with best practices and to promote evidence-based practice sustainability.
AcknowledgmentsThe authors thank the multiprofessional care and management teams at the general and cardiology ICUs and the Nursing Development and Stomal Therapy staff at the Hospital Sírio-Libanês for their support for and engagement with this project, as well as the entire Skin Champions team and the core working team that helped us with their ideas and availability for this project.
The authors also acknowledge the New Knowledge Unit for their guidance and guidelines, with special thanks to the education development manager for entrusting us with this challenge and believing in our potential.
The authors are also grateful to the instructors of the Evidence Implementation Training Program (EITP), taught by the Brazilian Centre for Evidence-based Healthcare: A JBI Centre of Excellence (JBI Brazil).
FundingThis EITP was funded by the HSL, which supported the nurses who authored this project.
Conflict of interestThe authors have no conflict of interest to declare in this project.
留言 (0)