
記住我
What is already known
Elevated blood pressure during pregnancy has been associated with adverse maternal and fetal outcomes. Several conditions are classified as hypertensive disorders in pregnancy, such as preeclampsia/eclampsia, gestational hypertension, and chronic hypertension. Preeclampsia is a disorder that affects multiple organ systems and is usually characterized by high blood pressure and proteinuria after 20 weeks of gestation.What this article adds
Continued nursing education is vital and should continue to be supported, utilized, and encouraged through the unit's nurse educator and/or nursing administration. Simulation is a strategy to encourage evidence-based practice at the point of care, which allows the acquisition of clinical skills through deliberate practice. Assessment, identification, and documentation are key to improving outcomes of pregnant women with hypertensive disorders. IntroductionThe United States is the only industrialized nation with a consistently rising maternal mortality rate, despite spending more per capita on health care than any other country.1 One woman dies every 2 min due to pregnancy-related complications.2 Elevated blood pressure (BP) during pregnancy has been associated with adverse maternal and fetal outcomes.3 Although Mississippi's mortality rate ranked 32nd in 2018, the increasing prevalence of obesity, hypertension, and lack of access to care in rural Mississippi could contribute to future ranking changes.4 In 2019, 13.9% of women giving birth in Mississippi received inadequate prenatal care, and 5% acquired late or no prenatal care at all.5 Although access to care, obtaining care, and current comorbidities do contribute to maternal and fetal mortality, assessment and early risk recognition play a vital role in complication prevention.6
Hypertension in pregnancy affects as many as 8% of births in the United States with more than 10 000 fetal deaths resulting.3 The American College of Obstetricians and Gynecologists (ACOG) Task Force on Hypertension in Pregnancy defines hypertensive disorders as chronic hypertension, gestational hypertension, preeclampsia with or without features, and eclampsia.7 Chronic hypertensive disorders include hypertension present before conception or hypertension occurring prior to 20 weeks’ gestation8; whereas gestational hypertension occurs after 20 weeks’ gestation.8 Chronic and gestational hypertension place pregnant women at risk of complications, including preeclampsia, eclampsia, pulmonary edema, and HELLP (hemolysis, elevated liver enzymes, low platelets) syndrome.8Preeclampsia is a hypertensive disorder of pregnancy that affects multiple organ systems, including the heart and kidneys, as evidenced by high BP and proteinuria after 20 weeks’ gestation.9 The International Society for the Study of Hypertension in Pregnancy (ISSHP) defines preeclampsia as hypertension of at least 140/90 mmHg on two separate occasions at least 4 h apart accompanied by significant proteinuria of at least 0.3 g in a 24-h collection of urine (or >30 mg/mmol protein/creatinine ratio), arising de novo after the 20th week of gestation in a previously normotensive woman, and resolving completely by the 6th postpartum week.8Preeclampsia, once described as mild or severe, is now defined based on the presence or absence of features, according to the ISSHP.8Preeclampsia with features includes any of the following symptoms: right upper quadrant pain, nausea, visual changes, breathing difficulty, and edema in the extremities.7Preeclampsia convolutes as much as 3.8% of pregnancies in the United States and almost 5% globally.7 Despite these seemingly low numbers, preeclampsia remains a leading cause of mother and infant morbidity and mortality.3 The definitions and treatment guidelines issued by ISSHP, ACOG, and the National Institute for Health and Care Excellence (NICE) serve the United States and the United Kingdom as evidence-based guidelines for the diagnosis and management of preeclampsia.7–9 Healthcare teams are learning to appreciate preeclampsia as a multidimensional, compound, and escalating disease process.7 Current treatment protocols for preeclampsia are directed at the presence or absence of features of preeclampsia.6Preeclampsia, left untreated, increases the risk of eclampsia, pulmonary edema, and HELLP8; therefore, assessment and recognition of the signs and symptoms of disease progression and complications remains a key to prevention.6
According to a 2020 Gallup poll, nursing in the United States remains the most trusted profession for the 19th consecutive year.10 Although Americans appreciate and value nursing integrity and ethical standards, it is believed that nurses rank high consistently because, of all healthcare professionals a client may encounter, nursing is the profession that is most present.10 This presence represents ongoing care, assistance, empathy, and comfort while promoting effective communication with the client.11 Therefore, bedside nurses, specifically those represented in intrapartum settings, are often the first to identify the subtle, subjective signs and symptoms of hypertension and the complications associated with hypertensive disorders in pregnancy.7 Management of hypertensive disorders and the clinical decision to treat them continue to be based on clinical manifestations.7 Hypertensive bundles, which are pre-set, outlined interventions or algorithms used to manage pregnant mothers with hypertensive complications, are being implemented in hospital settings across the United States.7 However, ongoing evaluation and nursing care are key in the prevention of complications resulting from hypertensive disorders in pregnancy.7
The current quality improvement project is a result of opportunities for improvement identified by clinical leadership in the nursing assessment of women with hypertensive disorders of pregnancy admitted to the intrapartum unit at the Winfred L. Wiser Hospital for Women and Infants at the University of Mississippi Medical Center (UMMC) in Jackson, Mississippi. The UMMC is the only academic health science institution in Mississippi. It is a publicly owned medical facility with the largest group of maternal–fetal subspecialists in the state. The Wiser Hospital for Women and Infants uses cutting-edge technology to diagnose and manage unique and complicated pregnancies, including mothers with hypertensive disorders. There are currently 38 registered nurses employed in the intrapartum unit, and as many as 208 medical students and 24 obstetric residents were rotated through the area during this project.
From January 2021 to April 2021, the intrapartum unit at UMMC served more than 650 pregnant clients, many with hypertensive disorders. An estimated 30–35% of these clients were treated for preeclampsia. Staff cared for a large percentage of the 18.9% of pregnant women in Mississippi who received little to no prenatal care in 2019.5 Predicting which pregnant women will succumb to pregnancy complications secondary to hypertensive disorders of pregnancy is impossible; however, the majority of complications are preventable or treatable when care is early and adequate.2 Mothers and infants are susceptible to long-term complications resulting from untreated hypertension, although some treatment is better than none due to the risk of death or disability.2 Pre-conception care and early prenatal care are directly related to pregnancy outcomes, but for those with limited access to healthcare, the first healthcare visit may not occur until the woman has been admitted for labor.2 Therefore, it is imperative for bedside nursing staff to be equipped to perform thorough and complete assessments to allow for early identification of progressing hypertensive disorders.2Hypertension, cardiomyopathy, and pulmonary edema are among the recurrent factors leading to maternal death.1 At this time, the only cure for hypertensive disorders of pregnancy is the delivery of the neonate.3 However, delivery for cure commonly results in the birth of a preterm infant, compounding the risk of negative outcomes.3 Ultimately, this project sought to optimize compliance with best practices for early identification of progressing hypertensive disorders and prevention of related complications to decrease maternal and infant morbidity and mortality. An evidence summary developed by JBI,12 the NICE guidelines,9 and CEUFast Inc., an accredited provider of nursing continuing professional development by the American Nurses Credentialing Center's Commission on Accreditation,13 supported the audit criteria used in this implementation project. The Preeclampsia Foundation, ACOG, ISSHP, California Maternal Quality Care Collaboration (CMQCC), and NCC-WHC support the practice guidelines used for this project.
Because eclampsia, pulmonary edema, and HELLP syndrome can be prevented through early detection of preeclampsia, the project team members chose it as the main focus for this project. The NICE guidelines recommend BP assessments based on the client's classification of hypertension, including chronic, gestational, or preeclampsia with or without features.9 The NICE guidelines also support the administration of antihypertensive treatments throughout the intrapartum period and consideration for operative delivery based on labor progress and the presence of preeclampsia with features.9 Clients experiencing preeclampsia without features require lung assessments every 4 h, while those experiencing preeclampsia with features should be assessed every 2 h.13 Advanced practice nurses, practical nurses, registered nurses, and midwives promote early detection and intervention by adhering to the recommended assessment guidelines.13 The CMQCC supports these assessments and adds the assessment of deep tendon reflexes (DTRs) every 12 h for clients with preeclampsia without features and every 4 h for clients with preeclampsia with features.14
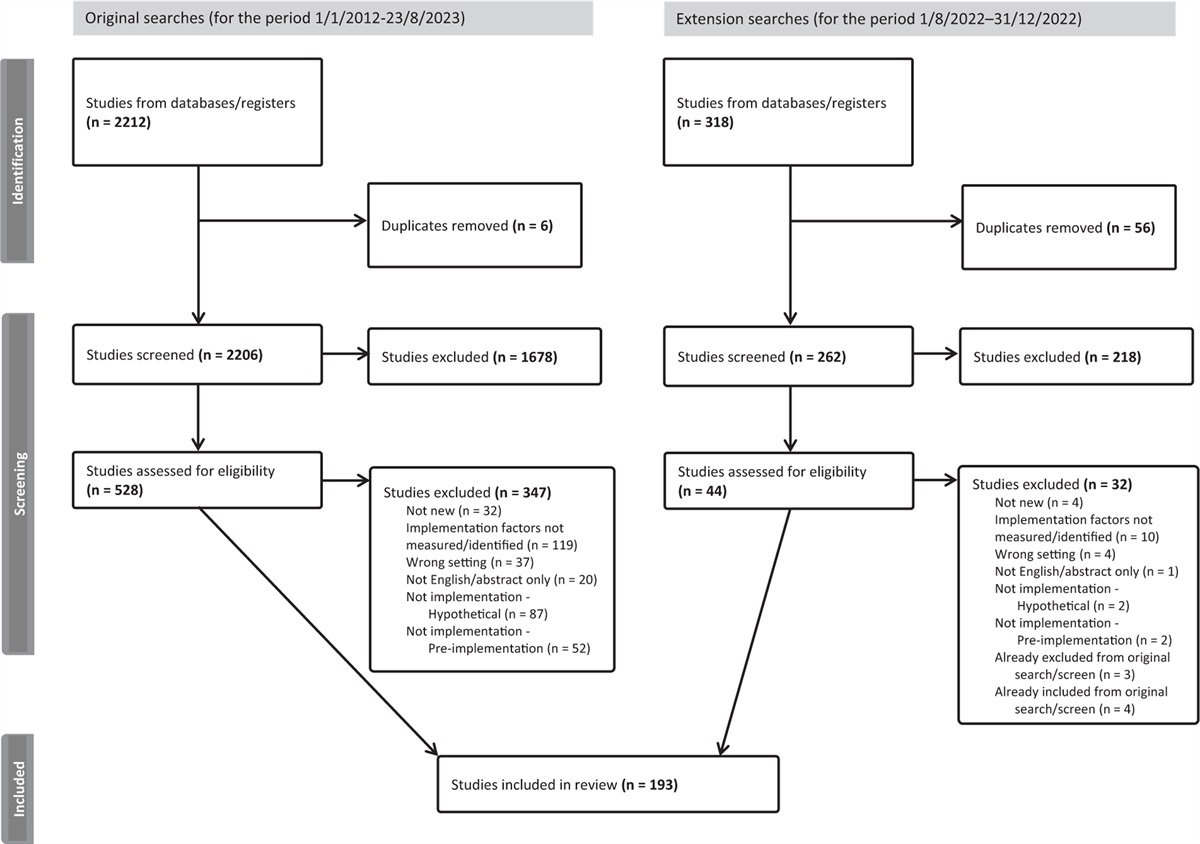
The implementation of this best practice project was guided by the JBI Model of Evidence-based Healthcare15 and used the JBI Practical Application of Clinical Evidence System (PACES) and Getting Research into Practice (GRiP) audit and feedback strategy (JBI, Adelaide, Australia)16 to promote evidence-based practices regarding the nursing assessment of pregnant women with hypertensive disorders admitted to an intrapartum unit. Practices regarding the nursing assessment of pregnant women with hypertensive disorders were audited to ensure awareness of and adherence to current best practice recommendations, which are central to optimizing client outcomes. This evidence implementation project used baseline audits to determine the level of awareness of and compliance with best practice recommendations through the JBI PACES audit and feedback tool. Next, interventions to encourage the adoption of evidence-based practices regarding the nursing assessment of pregnant women with hypertensive disorders were implemented. Follow-up audits were conducted to determine the effectiveness of the interventions.
ObjectivesThe aim of this project was to promote evidence-based practices regarding the nursing assessment of pregnant women with hypertensive disorders admitted to an intrapartum unit.
Specific objectives:
1. To determine baseline compliance with evidence-based practices regarding nursing assessment of pregnant women with hypertensive disorders. 2. To design and implement strategies to address areas of noncompliance regarding the nursing assessment of pregnant women with hypertensive disorders. 3. To complete a follow-up audit to assess compliance with evidence-based practices after the implementation of strategies. MethodsThe current evidence implementation project used the JBI evidence implementation framework.16 The JBI implementation approach is grounded in an audit and feedback process along with a structured approach to the identification and management of barriers to compliance with recommended clinical practices. It consists of seven stages, including identification of practice area for change, engaging change agents, assessment of context and readiness to change (i.e., situational analysis), review of practice (i.e., baseline audit) against evidence-based audit criteria, implementation of changes to practice, reassessment of practice using a follow-up audit, and consideration of the sustainability of practice changes.
The JBI PACES and GRiP tools were also utilized, which involve three phases of activity:
Establishing a team for the project and undertaking a baseline audit based on criteria informed by the evidence. Reflecting on the results of the baseline audit and designing and implementing strategies informed by the GRiP framework to address noncompliance found via the baseline audits. Conducting follow-up audits to assess the outcomes of the interventions implemented to improve practice and identify future practice issues to be addressed in subsequent audits. EthicsThe current project did not require approval by the Institutional Review Board (IRB) as it was not considered research, but a quality improvement project, according to the flowchart and self-certification form referenced through the University of Mississippi Medical Center IRB website.17
Phase 1: Stakeholder engagement (or team establishment) and baseline auditA project team consisting of the unit's nurse educator, nurse manager, and a Doctor of Nursing Practice student with a special interest in this area was formed. An initial meeting and a course of e-mail correspondence were held at differing times during the planning period of the project. Although the roles of the team members varied, all were actively involved in the structure, format, and development of the project and related interventions.
Four audit criteria were developed based on best-practice recommendations for the assessment of pregnant women with hypertensive disorders from a JBI evidence summary.12 These four audit criteria can be accessed from the JBI PACES online tool. Another four audit criteria were included based on the recommended nursing assessment guidelines for the frequency of lung and DTR assessments and the client's degree of hypertension.9,13,14,18
The evidence-informed audit criteria used in the project (baseline and follow-up audits), together with a description of the sample and approach for measuring best practices for each audit criterion, are listed in Table 1. A baseline audit was conducted of 20 electronic health records (EHRs) of pregnant women with hypertensive disorders admitted to the intrapartum unit. The EHR audits were conducted on 1 August 2021 and were based on hypertension-related International Classification of Diseases, 10th Revisions (ICD-10) codes of clients admitted between 1 January 2021 and 30 June 2021. The UMMC Center for Informatics and Analytics was pivotal in the collection and reporting of this specific information. The US Department of Health and Human Services requires institutions covered by the Health Insurance Portability and Accountability Act to use ICD-10 for medical coding.19 Codes O10–O16 represent the various types of hypertension occurring in pregnancy. Some of these included pre-existing hypertensive disorders (O10–O11), gestational hypertensive disorders (O12–O13), preeclampsia-related disorders (O14–O15.9), and unspecified maternal hypertension (O16).20 See Table 2 for a complete list of ICD-10 codes used in the EHR audits.
Table 1 - Audit criteria, sample, method to measure compliance, and audit guide Audit criteria Sample Method used to measure % compliance with best practice Audit guide Antenatal antihypertension treatments are continued throughout intrapartum in women with hypertensive disorders during pregnancy 20 pregnant women with hypertensive disorders, as defined by ICD codes O10, O10.1, O10.2, O10.3, O10.4, O10.5, O10.6, O10.7, O10.8, O10.9, O11, O12.0, O12.1, O12.2, O13, O14, O14.1, O14.2, O14.3, O14.4, O14.5, O14.6, O14.7, O14.8, O14.9, O15, O15.1, O15.2, O15.3, O15.4, O15.5, O15.6, O15.7, O15.8, O15.9–O16 Chart audit was performed in collaboration with the CIA “Yes” if there was documentation of pregnant women with hypertensive disorders receiving antihypertensive medications throughout the intrapartum periodCIA, The Center for Informatics and Analytics; DTR, deep tendon reflexes; ICD, International Classification of Diseases.
Phase 2 was conducted from 1 October 2021 to 20 October 2021. The GRiP tool was used to identify the barriers and develop strategies to overcome the barriers. The project team reviewed and compared the results of the baseline audit against the best-practice standards for the nursing assessment of pregnant women with hypertensive disorders. Gaps between evidence and practice were identified for criteria 3, 5, 6, 7, and 8. The project team held three discussion sessions to reach final consensus on change strategies. The aims of the consultation sessions were to garner professional and technical support for the project, identify any potential barriers to implementing best practices that may emerge, develop strategies based on the available resources to overcome the barriers, and draft relevant EHR changes based on research evidence and contextual factors for pregnant women with hypertensive disorders.
Phase 3: Follow-up audit postimplementation of change strategyThe follow-up audit was conducted following the GRiP phase. The data were collected using the same audit criteria as in the baseline audit and with the same sample size and auditing process. The follow-up data collection was conducted from 21 October 2021 to 27 November 2021.
AnalysisResults data on changes in compliance were measured using descriptive statistics embedded in JBI PACES in the form of percentage changes from baseline.
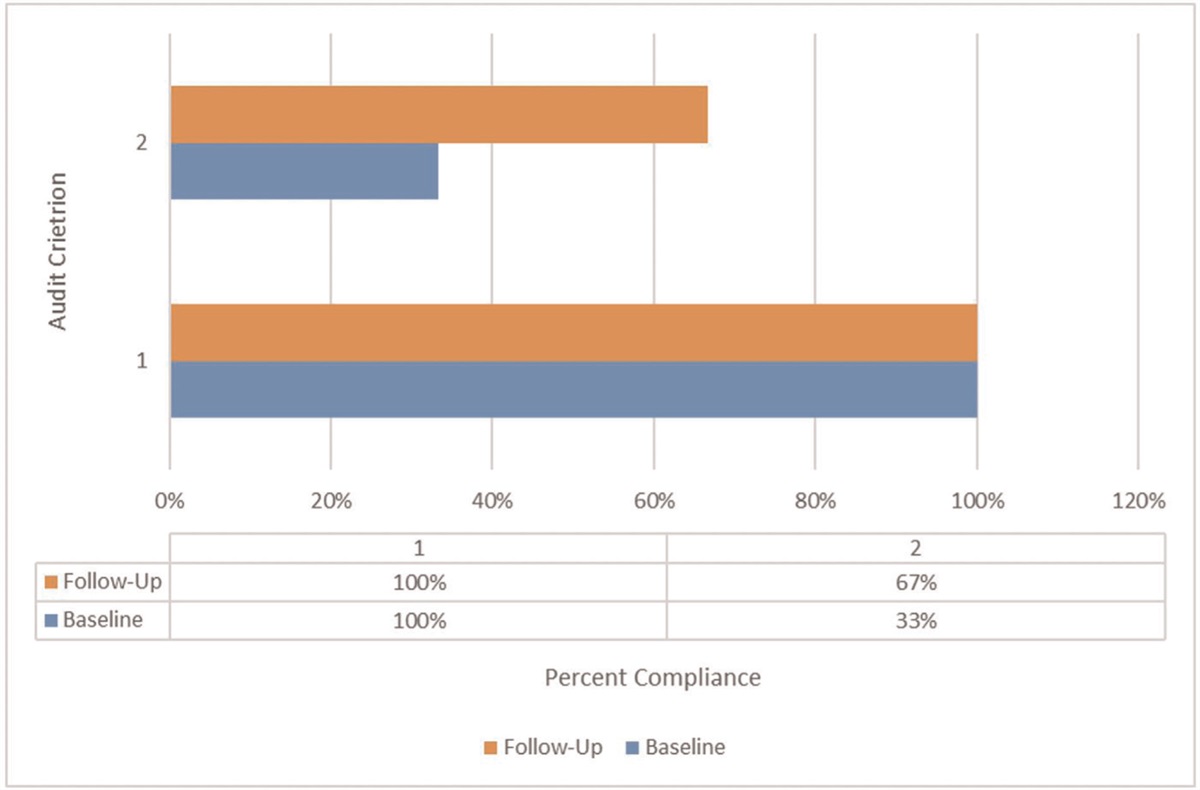
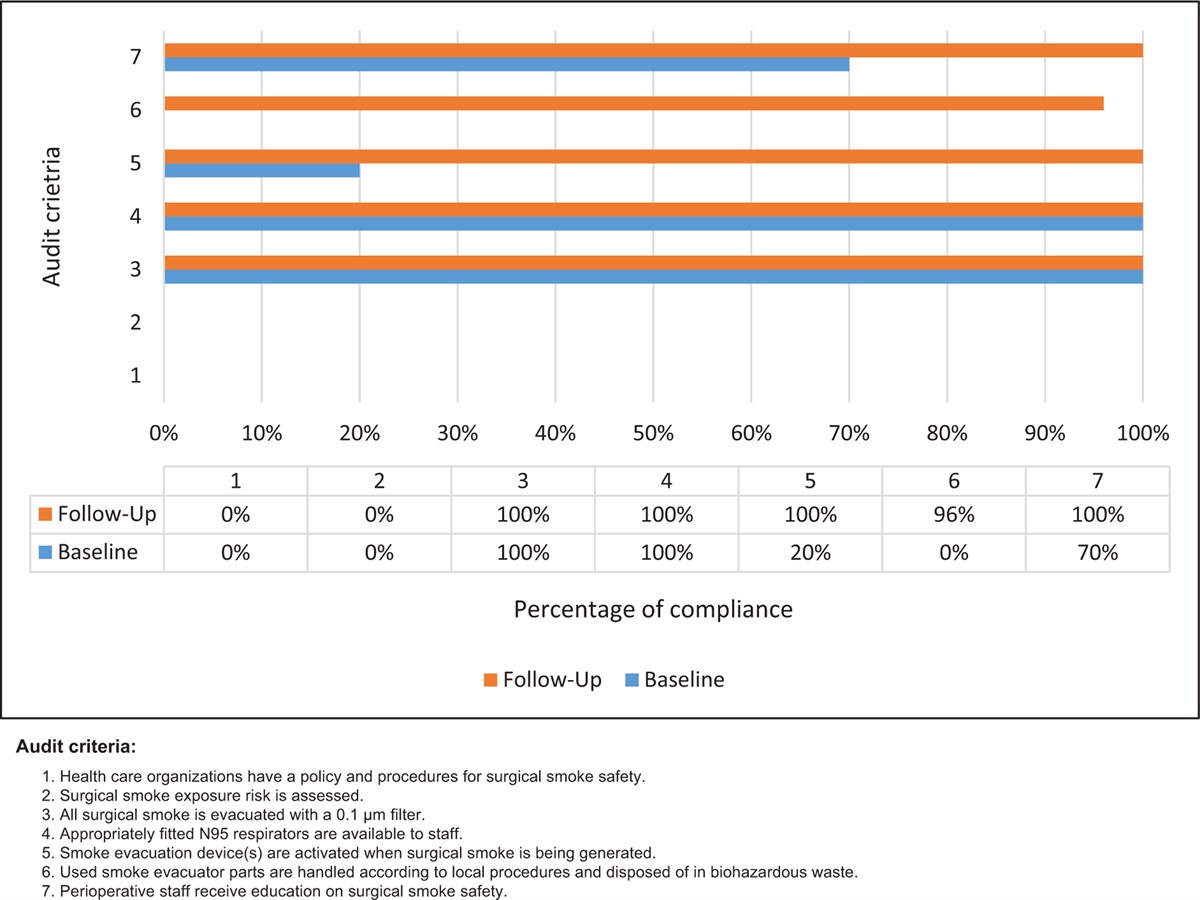
Results Phase 1: Baseline auditAll women with hypertensive disorders received antihypertension treatments throughout the intrapartum period (criterion 1; 100%) and had their BPs monitored and documented according to the assessment guidelines (criterion 2; 100%). However, pregnant women with severe hypertension did not have their BP monitored and documented as recommended (criterion 3; 37.5%). All pregnant women with sustained severe hypertension were evaluated to determine the need for an operative or assisted delivery, resulting in 100% compliance with criterion 4. Criteria 5 and 6 (frequency of lung assessments) were met with only a 10% compliance rate. The compliance rate was 0% for criteria 7 and 8 (frequency of DTR assessments).
Phase 2: Strategies for Getting Research into PracticeThree barriers to compliance with best practices were identified, and strategies to overcome these barriers (as summarized in Table 3) were then implemented over an 11-week period.
Table 3 - Getting Research into Practice matrix Barrier Strategy Resources Outcomes Lack of knowledge Provide an on-site simulation educational opportunity for nursing staff to improve assessment skills and documentation guidelinesDTR, deep tendon reflexes; EBPs, evidence-based practices; EHR, electronic health record.
The first barrier was a lack of knowledge regarding current nursing assessment guidelines for the frequency of lung and DTR assessments of pregnant women with hypertensive disorders. The nurses also expressed concern regarding their own proficiency to identify various adventitious lung sounds. This factor contributed to less frequent lung assessments and inadequate documentation. The current unit practice was to assess and document lung sounds and DTRs every 6 h. The nursing staff was provided simulation training to review normal and abnormal lung sounds, DTR testing, and documentation of these findings. All 35 nurses and one nursing student verbalized understanding of updated assessment guidelines. Laminated reminder cards containing lung and DTR assessment guidelines were made to remind nursing staff of the current practice. These cards were placed at both nurses’ stations and on each documentation station within the intrapartum unit.
The second barrier was inadequate documentation by nursing staff. Education during the simulation training emphasized the recommended assessment and documentation frequency based on the NICE guidelines.9 During this training, the participants agreed that the lack of documentation could be due to EHR limitations or that the nurse did not personally perform the assessments but witnessed them. Nursing staff expressed often being present during lung and DTR assessments performed by residents and attending physicians and felt there was no need to perform the same assessments again. The staff was reminded that documentation is evidence of care provided and was encouraged to document the witnessed assessments in their nursing documentation to support best practices. All participants (35 full-time nurses and one senior nursing student) confirmed an understanding of the current recommendations for the frequency of documentation.
The third barrier was documentation limitations within the EHR. Although the current EHR offers a specific hypertensive disorders assessment template, this template lacks the inclusion of lung assessment findings. Lung assessments were being documented in a separate tab within the EHR, which increases the chances of inadequate documentation. A request was submitted to the EHR development team to add lung assessment to the existing hypertensive disorders assessment template to improve documentation compliance. The intrapartum nurse manager and hospital director approved this change.
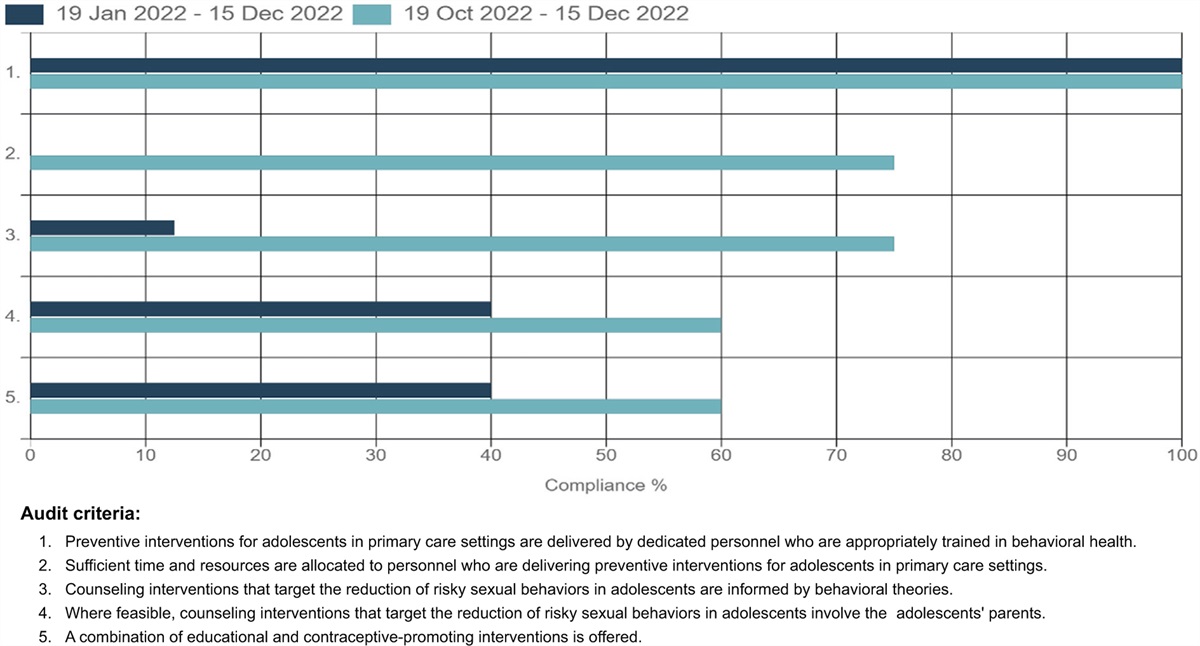
Phase 3: Follow-up auditAs shown in Fig. 1, all pregnant women with hypertensive disorders continued to receive antihypertension treatments throughout the intrapartum period (criterion 1; 100%). Compliance with BP monitoring for pregnant women with hypertensive disorders remained at 100% compliance from the baseline audit. Pregnant women with severe hypertension had their BP monitored and documented 100% of the time, a significant improvement from a baseline compliance rate of 37.5%. Criterion 4, consideration of operative or assistive births, remained at 100% compliance. Criteria 5 and 6 (frequency of lung assessments) more than doubled in compliance percentage. Lung assessments of pregnant women with hypertensive disorders increased from 10% compliance to 38.89%, while lung assessments of pregnant women with preeclampsia with features increased from 10% to 22.22%. Criteria 7 and 8 (frequency of DTR assessments) showed the greatest improvement in compliance. Postimplementation audits revealed DTR assessments for pregnant women with hypertensive disorders was 72.22%, while DTR assessments for pregnant women with preeclampsia with features was 50%. These numbers are a significant improvement when compared with a baseline compliance rate of 0%.
 Figure 1:
Figure 1: Compliance (%) with best practice for audit criteria at baseline and follow-up.
DiscussionThere are many risks associated with pregnancy and labor from the moment of conception. However, pregnant women experiencing hypertensive disorders are considered at higher risk of pregnancy and labor complications, including preeclampsia, eclampsia, pulmonary edema, and HELLP. Early identification of preeclampsia promotes early intervention, resulting in improved outcomes and decreased mother and infant morbidity and mortality. The aim of this implementation project was to promote evidence-based practices regarding the nursing assessment of women with hypertensive disorders during pregnancy. Following the baseline audit of 20 EHRs, analysis of the barriers led to the development and implementation of three strategies, including on-site simulation for nursing staff, an EHR change, and reminder cards for quick reference use by nursing staff during client care. A follow-up audit was performed, showing significant improvements in compliance with BP monitoring frequency and documentation, specifically of pregnant women with severe hypertension. The frequency of lung and DTR assessments also increased for pregnant women with hypertensive disorders and those with preeclampsia with features.
In the baseline audit, the project team identified several opportunities for improvement with regard to nursing assessment frequency and documentation. The most important opportunity to improve knowledge or awareness of the most recent nursing assessment guidelines. Although the intrapartum unit employs a full-time nurse educator and nurse manager, adhering to ongoing and changing practice recommendations can be challenging. After meeting with the nurse educator and nurse manager, a plan was developed to address not only improving assessment compliance but also fulfilling the unit's quarterly competency needs. An on-site simulation activity was planned, and two dates were scheduled to allow participation from all current nursing staff. The staff were provided YouTube videos demonstrating lung and DTR assessment techniques and illustrated graphs differentiating normal and abnormal lung sounds to review prior to the scheduled simulation activity. The simulation activities were implemented with 100% staff participation. During this time, current assessment guidelines were reviewed, normal and abnormal lung sounds were auscultated on a simulator, and each participant performed a DTR assessment on their coworker. Assessment guidelines were printed and laminated on cards for nursing reference and use in each intrapartum client room.
Second, an opportunity to improve documentation of BP, lung, and DTR assessments was identified. Although this opportunity was directly linked to the nursing staff's lack of knowledge, documentation limitations were identified during the baseline audit and after discussion with the nursing staff during the simulation activity. Most nursing staff expressed not documenting a lung or DTR assessment performed by physicians, although they were present when the assessment was performed. The nursing staff was encouraged to document the witnessed assessment and who performed it. This prevented excessive and unnecessary patient stimulation while promoting compliance with assessment frequency. A second barrier to documentation was identified in the EHR, and a request for change was submitted to add a place for lung assessment to the existing hypertensive disorders assessment template. Though this change has not yet been implemented, it is expected that documentation compliance will increase by having all areas of the recommended nursing assessment in one location.
The current implementation project resulted in positive changes in compliance with nursing assessment frequency and documentation for pregnant women with hypertensive disorders. There was an improvement in compliance for all best-practice recommendations and maintenance in the areas noted to have 100% compliance during the baseline audit. To maintain and sustain this improvement, the current nursing assessment guidelines must continue to be followed by nursing staff. Education and training must continue to be strengthened, not only for existing nursing staff but as new nursing staff are employed and oriented. Quarterly competencies should reflect the most up-to-date best-practice recommendations. Access to the lung sound simulator for nursing staff would be beneficial to promote proficiency in auscultation skills. Therefore, funding to support the purchase of a simulator will be explored.
A review of similar projects implemented supports the need for improving protocol compliance in the assessment and management of pregnant women with hypertensive disorders. ElazimElmenshewy et al.21 identified the need for more training to address methods of BP measurement and identifying symptoms of eclampsia. O’Brien et al.22 audited the adherence to unit protocols and algorithms used to treat severe hypertension, resulting in the identification of conflicting protocols and issues with communication.
There are limitations to this project that should be considered. Early maternity leave of the nurse educator placed the team member's responsibility on the nurse manager, leading to simulation scheduling delays and communication challenges. A second limitation occurred during Phase 3 while conducting the follow-up audit. The challenge was the inability to search client types by diagnosis codes due to incomplete coding and chart completion. A backup search was implemented with assistance from the nurse educator on the intrapartum unit. Although the end results were not affected, the original follow-up audit was unable to be completed through the Center for Informatics and Analytics at UMMC, thereby delaying follow-up audit data. In addition, the duration of Phase 3 was less than 2 months; compliance rates may have been affected with more time between implementation and the follow-up audit.
ConclusionThe current evidence implementation project utilized a clinical audit process leading to improvements in practice behavior related to nursing assessments of pregnant women with hypertensive disorders. Baseline audits revealed an average 45% compliance rate with the eight best practice audit criteria. Follow-up audits revealed an average compliance rate of 73% for all eight audit criteria, a 28% improvement.
The project team members were successful in identifying the need for change in the EHR template to improve documentation frequency, educating the nursing staff on current practice guidelines, and promoting confidence in skills proficiency, including lung and DTR assessment. The nurse educator and nurse manager will continue to promote current practice guidelines with new staff and during quarterly competency events.
AcknowledgmentsThe authors would like to acknowledge Alyssa Mamdani, RN, BSN, nurse educator for the intrapartum unit at Wiser Hospital for Women and Infants for her assistance and support throughout the change implementation process in phase 2 and the EHR audits during phase 3.
Conflicts of interestThere are no conflicts of interest to declare for this project. This report will contribute toward a Doctor of Nursing Practice (DNP) degree for TP.
留言 (0)