
記住我

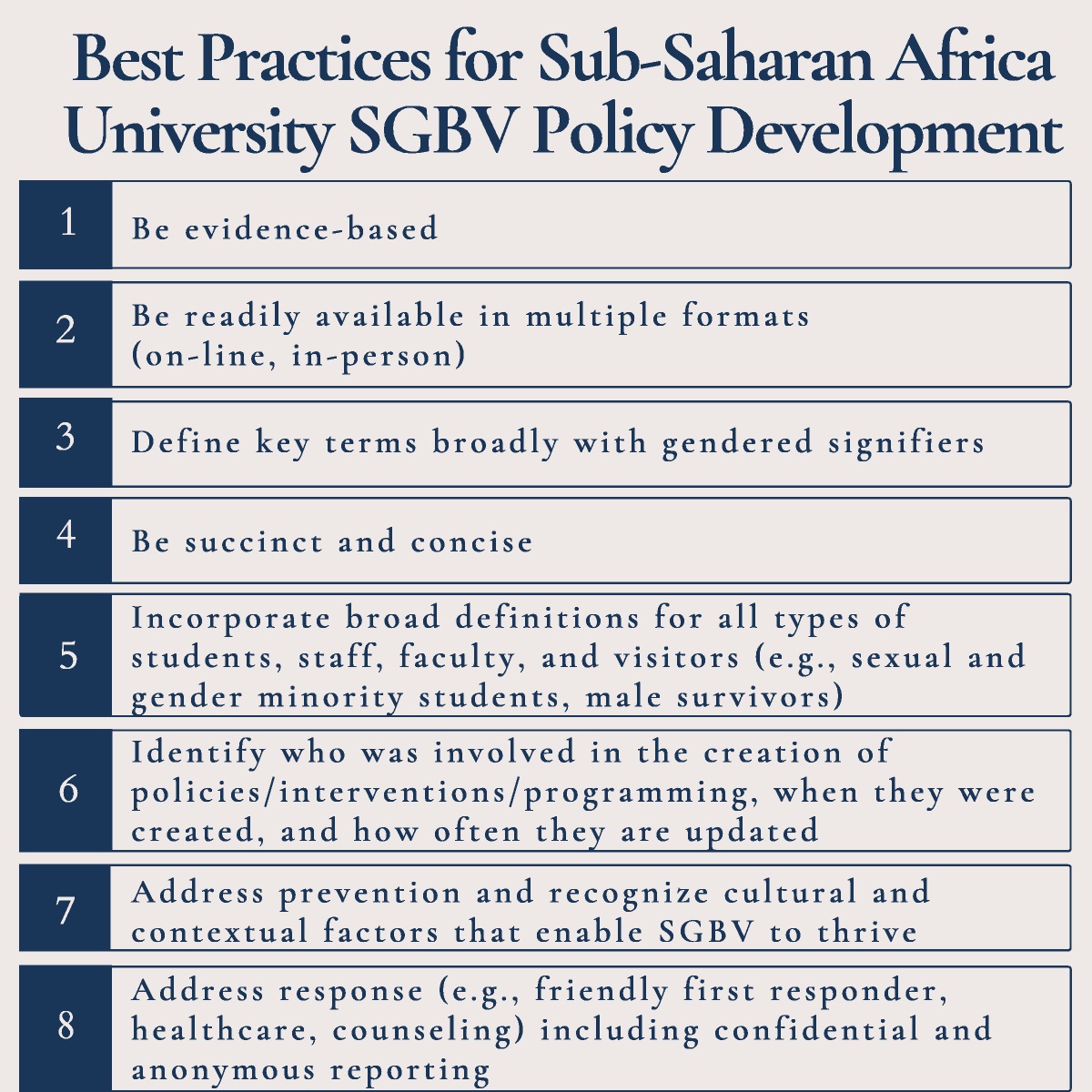

The Nelson Mandela Rules require that individuals experiencing incarceration should enjoy the same standards of health care that are available in the community (Rule 24.1; McCall-Smith, 2016). This international standard underlines the importance of respecting prisoners' autonomy with regard to their own health (Rule 32.1.b) and ensuring the confidentiality of medical information (Rule 32.1.c). Incarcerated people carry a high burden of physical and mental health conditions (Fazel & Baillargeon, 2002), including trauma, anxiety (Dudeck et al., 2011), substance use disorder (Fazel et al., 2006), and serious mental disorders (Fazel & Seewald, 2012). Ensuring access to medication while conforming to prison or jail security requirements, and taking into account concerns about trafficking, theft, and misuse, particularly of prescribed psychoactive substances, need a pragmatic and well-adjusted operational approach (Elger & Shaw, 2017). Ensuring the continuum of care between the community, the prison, and back to the community is also a challenge, especially for continued medication treatment (Norman & Parrish, 1999). For example, the coordination between community and prison of the prevention, treatment, and care continuum for individuals with severe infectious diseases, such as tuberculosis, offers a telling example (Herce et al., 2018). Therefore, clinical services operating in prisons and jails, which should be independent of custodial and justice authorities (Pont et al., 2018), play a critical role in offering nonpharmacological and pharmacological treatment to treat, care for, and support individuals. Preparing them to reintegrate into the community and continue their prescription medication upon their release is equally important (Vaughn, 1997).
Focusing on prescribed medications, their preparation forms a significant part of the daily activities of medical staff as to allow individuals to timely access to their treatment. By relying on prison officers or even fellow incarcerated individuals, many models of medication preparation and distribution in prison do not adhere to standards of quality of care, autonomy, confidentiality, and respect and dignity (Tran et al., 2020). In some of the worst instances of poor quality of care and disempowerment, tablets are crushed, mixed with water, and given to patients who must take it under direct staff supervision. There is a paucity of research on the best practices regarding this essential operational aspect of health service management in prisons (Tran & Wolff, 2020).
Professionals from the Geneva University Hospitals provide health services for people incarcerated in the detention facilities in the Geneva Canton, Switzerland. These professionals (nurses, psychologists, physiotherapists, dentists, and physicians from different specialties, including internal medicine and mental health) work independently from the custodial and criminal justice authorities. Their work is underpinned by the equivalence of care principle, among other rights-based principles (Pont et al., 2018; Pont & Harding, 2019), such as the use of respectful and person-centered language (Tran et al., 2018). When La Brenaz, a male-only carceral facility for sentenced individuals, opened in 2008, it initially had 68 individual cells and a specific system of medication preparation and distribution. First, there were no healthcare staff during weekends and certain holidays, and therefore, the facility could not receive individuals who required supervised medication intake. During workdays, nurses prepared prescribed medications in paper sleeves on which they wrote the patient name and dosing and placed them in individual name-tagged but not lockable boxes (resembling shoe boxes) before giving them to prison officers. On the day before weekends or holidays, when there was no healthcare staff on duty, additional medication sleeves were prepared accordingly. Prison officers stored them in a cabinet in each of the units and unlocked it once daily at a set time for patients to take their medications before locking it again after use. They did not supervise the medication intake. Although the system allowed users to be autonomous, it lacked confidentiality and was prone to medication thefts and exchanges and, at times, disrespectful user interactions. In 2012, because of these disadvantages described, the healthcare team, under nurses' impulse, conceived a new approach consisting of personal lockable medication boxes, which this study aimed to describe and evaluate.
MethodsA cross-sectional study was carried out at La Brenaz detention facility from March 1 to August 9, 2019, using convenience sampling.
ProceduresIn 2012, in coordination with the carceral authorities, one of the prison units implemented the lockable medication box system. The boxes, akin to the mailbox system (see Figure 1), were set up inside the carceral unit. Each person living in that unit received from prison staff a key for his medication box, whether he was under pharmacological treatment or not. Both prison staff and nurses held a master key that opened all boxes. Nurses prepared the medications in individual name-tagged paper sleeves. As medical staff worked (and have continued working) independently from the carceral and criminal justice authorities, they did not have the keys to enter the locked units. Therefore, a prison officer accompanied the nurse to open the pilot unit. The nurse opened the boxes of individuals who had prescribed treatment and placed the corresponding medication sleeves with a medication card into the boxes before locking them. The card was a reminder of when, why, and how to take each treatment. The distribution rounds occurred when the unit was empty (i.e., during vocational training or working hours). Therefore, there was no interaction with users: They picked up their treatment from the boxes and took it on their own. However, doctors first saw patients individually to discuss treatment options and, if a medication was required, explained its indication, main side effects, and the way to take it. Once medications were prescribed, prepared, and distributed, patients' adherence was monitored by doctors and nurses in individual follow-up visits. Access to other healthcare services continued to be guaranteed. Importantly, excluded from the box distribution were the medications that required an intake directly observed by nurses. These were controlled substances, such as opioid agonist therapy; medication prone to trafficking, such as methylphenidate for attention-deficit/hyperactivity disorder; and those requiring careful intake monitoring based on the initial patient assessment made by nurses and doctors.
 FIGURE 1:
FIGURE 1: Individual lockable medication boxes.
After a year of piloting, prison authorities scaled up the system to the whole facility, including when it expanded in 2015 to a total capacity of 168 individual cells. Over the years, the frequency of in-box distribution became more flexible. It offered patients several options depending on individual preferences and situations: once weekly (Mondays), twice weekly (Mondays and Thursdays), or more frequently as needed. The clinical team took the time to evaluate each new patient and get familiar with his medical needs and resources before deciding which distribution modality to adopt. In 2017, increased resources allowed nurses to also work on weekends and holidays, which allowed the facility to accommodate individuals who required supervised intake. Such individuals received their medication in hand from nurses.
FrameworkUsers, officers, and prison authorities provided iterative feedback over the years that has helped improve the running of the medication distribution boxes. However, nurses and doctors engaged in the continuum of patient care and medication prescription, preparation, distribution, and follow-up felt that it was necessary to formally assess their system and adequately document the experience of users and prison officers. Such a process would help improve the intervention and promote the dissemination of the approach to other carceral facilities. Therefore, this study was done with an operations research lens to assess perceived advantages, disadvantages, and satisfaction levels to improve the running of the medication box system (Peters et al., 2013). In addition, participatory action research principles of ownership, democracy, and safe space underpinned this inclusive and multiperspective research process (Pope & Mays, 1995). Healthcare staff and, principally, nurses wanted to actively participate in designing and conducting this research on an approach that they spearheaded in the first place (ownership). They also wanted to engage and give a meaningful voice to users and prison staff to inform potential actions to improve their system (democracy) within a safe space for mutual learning and program improvement.
Study PopulationOf 166 persons incarcerated at La Brenaz on March 1, 2019, 78 (47%) were on medication. Of these, four were under direct observation treatment (2% of the total population at La Brenaz), one had a pill organizer delivered in hand, and 73 (44%) received their medication in the medication boxes (37 weekly, 29 twice weekly, and eight daily). Of the 73 eligible individuals, 47 (64%) agreed to participate, six declined, and 20 were released before their interview.
Between May 20 and August 9, 2019, of 96 prison officers employed at La Brenaz, we invited all the 19 officers (20%) who were doing shifts at our clinic to participate in the study. All had previously accompanied nurses during their medication distribution rounds, and all agreed to enroll.
Data CollectionParticipants answered a standardized questionnaire administered by a team of nurses and physicians, who together were fluent in interviewing participants in French, English, Italian, Spanish, and German. The questions were crafted using an operations research lens to help answer programmatic issues (Peters et al., 2013). They were also framed by the long-standing experience of the healthcare team on medication dispensing as well as literature on the rationale to limit the prescription of certain substances in prisons (Burns, 2009). Such reasons included the potential for misuse; barter, sell, and trade; intimidation and victimization; security; and nursing challenges. Therefore, beyond sociodemographic characteristics (age, gender, country of birth, and educational level), questions explored the current experience with medication boxes (who provided the instructions on how to use the boxes, experience of thefts, disadvantages, advantages, and satisfaction) and the prospect of dispensing medication once a month. The questions were first drafted and tested in 2018 during a formative phase involving patients and prison officers before their use in the 2019 survey.
Statistical AnalysisData entry preceded quantitative data analysis (simple descriptive statistics) using IBM SPSS Version 25. Continuous variables were summarized as mean and standard deviation, and categorical variables were summarized as absolute and relative frequencies. There were no missing data.
Ethics StatementThe Cantonal Ethical Review Board of Geneva granted ethical approval for the study (2017-01379). All participants gave written informed consent.
FindingsTable 1 summarizes the general characteristics of the all-male end users and mixed-gendered prison officers.
TABLE 1 - General Characteristics of Participants End users Gender (male) 47 (100%) Age in years 39 (21–73) Number of years of education 11 (0–23) Region of origin 47 Western Europe 13 (28%) Eastern Europe 12 (26%) Sub-Saharan Africa 10 (21%) Northern Africa 8 (17%) Latin America 3 (6%) Asia 1 (2%) Prison officers Gender Male 15 (79%) Female 4 (21%) Age in years 33 (27–41) Number of service years at La Brenaz 4 (0–13)Data are n (%) or mean (range).
Medication users had treatment for somatic illnesses, mental health conditions, or both (see Table 2). Half (51%) received their treatment in the medication boxes once a week; 38%, twice a week; and five (11%), daily. The individuals in the daily category took medication for mental health conditions, such as attention-deficit/hyperactivity disorder and substance use, depression, or sleep disorders. Most had received instructions on how to use their boxes from prison officers who gave them the keys as well as from nurses and doctors. Only two participants reported a theft of medication, although this occurred in their room and not in relation to the boxes.
TABLE 2 - Evaluation of the Medication Boxes Among End Users (N = 47) Current experience Pharmacological treatment For physical disorders 35 (74%) For mental health 21 (45%) For both physical disorders and mental health 9 (19%) Frequency of medication distribution Once a week 24 (51%) Twice a week 18 (38%) Once a day 5 (11%) Instructions on how to use the box given by Prison officers 38 (81%) Nurses 33 (70%) Doctors 29 (62%) Theft of medication during the past 12 months In their cell 2 (4%) In the area close to the medication boxes 0 (0%) Disadvantages Risk of forgetting to pick up medication 5 (11%) Lack of instructions on how to use medication 3 (6%) Cannot pick up medication if sanctioned to cell lockdown 2 (4%) No health provider to talk to 1 (2%) Theft risk 1 (2%) Confidentiality issues 1 (2%) Risk of medication misuse 1 (2%) Do you agree with the following about the medication boxes? a Simple use 4.8 (0.38) More autonomy to manage my treatment while in prison 4.70 (0.51) Trains me on how to manage my treatment after release 4.3 (0.81) It shows that the medical staff trust me 4.66 (0.64) Respects my dignity (one missing value) 4.5 (0.72) Lower theft risk 4.40 (0.92) More confidential than in-hand distribution 4.4 (0.94) Allows to forget my treatment less frequently 3.8 (1.26) I am satisfied with this system 4.7 (0.58) I would recommend this system in other prisons 4.6 (0.82) Overall score of previous 10 variables 4.51 (0.50) Distribution once per month Agree that a monthly distribution of current treatment is possible 32 (68%) Potential disadvantages Risk of medication misuse 20 (43%) Too many medications to manage 17 (36%) Fear of mistake 11 (23%) Fear of theft 9 (19%) Delay in the delivery of newly prescribed medication 8 (17%) Others 3 (6%) Potential advantages More autonomy 24 (51%) Need to go less often to pick up medication 16 (34%) Less theft of medication 3 (6%) Others 2 (4%)Data are n (%) or mean (standard deviation).
a1 = do not agree at all, 2 = do not agree, 3 = neutral, 4 = agree, and 5 = strongly agree.
End users experienced a few downsides to the box system. These included the risk of forgetting to pick up their medication followed by the lack of instructions on how to use their medication (although counseling by medical staff for each new or renewed treatment was standard practice), no health provider to talk to, theft risk, confidentiality issues, and risk of medication misuse. Two mentioned the lack of access to the boxes when people were sanctioned to cell lockdowns (in this case, agents would pick up the medication on their behalf, which raised the issue of confidentiality). End users agreed or strongly agreed about the perceived advantages of the box system. These encompassed the ease of use, respect of human rights principles (increased autonomy to manage medication while in prison, which could also help after their release, respect of dignity, and more confidentiality than in-hand distribution), lower theft risk, the demonstration that medical staff trusted them, and increased compliance. End users were overall satisfied with this system and would recommend its implementation in other prisons.
A minority of officers reported disadvantages (see Table 3). These included the following: no availability of health provider for end users to talk to and subsequent communication triangulation (involving officers, end users, and medical staff); risk of medication or box key theft; and confidentiality issues, trafficking, and risk of medication misuse. One officer reported the burden of doing extra work to bring medication to patients if nurses forgot to deliver it in their boxes, which was perceived as less likely to occur with the in-hand distribution. As for advantages, officers agreed that the system allowed better role differentiation between prison and health staff. In general, their perception of advantages concurred with that of end users, albeit with a slightly lower magnitude (overall score of 4.05 [SD = 0.37] among officers and 4.51 [SD = 0.50] among end users). Officers strongly agreed that medication boxes were more time-efficient than in-hand distribution. To help substantiate this finding, nurses carried out an exploratory timing exercise during 70 distribution rounds in different sectors. Their results indicated that the dispensing of one medication package took, on average, 14 seconds with the inbox system compared with 80 seconds with the in-hand distribution (5.7 times shorter).
TABLE 3 - Evaluation of the Medication Boxes Among Prison Officers (N = 19) Current experience Disadvantages No health provider to talk to 6 (32%) Risk of medication theft 4 (21%) Risk of theft of medication box key 3 (16%) Confidentiality issues 2 (11%) Triangulation/indirect communication 1 (5%) Risk of medication misuse 1 (5%) Extra work for prison officers if health staff forgets to distribute medication during rounds 1 (5%) Medication trafficking 1 (5%) Do you agree with the following about the medication boxes? a More time-efficient than in-hand distribution 4.8 (0.42) Simple use 4.6 (0.61) Allows patients' autonomy to manage own treatment in prison 4.37 (0.68) Respects patients' dignity 4.4 (0.83) More confidential than in-hand distribution 4.1 (0.91) Trains patients on how to manage treatment after release 4 (0.91) Improves role differentiation between prison officers and health staff 3.9 (1.10) It shows that the medical staff trust users 3.84 (0.76) Lower theft risk 3.63 (1.07) Allows people to forget less to take their medication 2.7 (1.00) I am satisfied with this system 4.4 (0.76) I would recommend this system in other prisons 4.1 (0.94) Overall score of previous 12 variables 4.05 (0.37) Distribution once per month Agree that a monthly medication distribution is possible 5 (26%) Potential disadvantages Risk of medication misuse 19 (100%) Increased medication trafficking 17 (89%) Stocking medication 16 (84%) Risk of theft 11 (58%) Risk of mistake 6 (32%) “Difficulty in checking how so many medications truly belong to the patient.” 1 (5%) Potential advantages Fewer medication distribution rounds 15 (79%) More autonomy of patients 10 (53%) Patients need to go less often to pick up medication 2 (11%) Less theft of medication 0 (0%)Data are n (%) or mean (standard deviation).
a1 = do not agree at all, 2 = do not agree, 3 = neutral, 4 = agree, and 5 = strongly agree.
The prospect of a monthly distribution appealed to 68% of end users, but to only 26% of prison officers. For end users, potential disadvantages included the risk of medication misuse (a concern reported by all the officers), too many medications to manage with the fear of making mistakes, and the risk of theft. A few reported the risk of delay in delivering new prescriptions. In addition to medication misuse, most officers were worried about stockpiling and trafficking. As for potential advantages, end users cited more autonomy and less back and forth between boxes and cells, whereas officers largely saw fewer medication distribution rounds as the main benefit.
DiscussionThis study aimed to assess the novel approach of personal lockable medication boxes among incarcerated people and prison staff at La Brenaz. Overall, this distribution system was found to be simple to operate and yielded a high level of satisfaction while ensuring respect for key human rights principles, including autonomy, confidentiality, and dignity.
Current Distribution SystemTo our knowledge, this is the first study assessing a pioneering system of medication distribution via personal lockable boxes. In general, there was a similarity in the direction of answers from both end users and prison officers, with advantages outweighing disadvantages. The results from these two groups of stakeholders, including the simplicity of use, better time efficiency than in-hand distribution, and empowerment of people taking medication, confirmed the experience that medical staff, including nurses and physicians, had over the years. Nurses had more time for one-on-one follow-up consultations, and access to healthcare services remained guaranteed for all.
The most common concerns about the box system since its implementation were thefts, trafficking, and misuse. There were two cases of thefts reported by end users over the previous 12 months, which occurred in the cells and did not relate to the medication boxes. Both end users and officers agreed that the system lowered the risk of theft. Users have had the option to leave their medication in their lockable boxes for increased safety instead of bringing all of it back to their rooms. Since the inception of the medication boxes, our medical team has not experienced cases of medication thefts linked to the boxes. Regarding the risk of misuse, our experience also matched that of end users and officers. There had been no case of medication overdose or misuse linked to the box system itself. This risk was mitigated by the careful eligibility assessment by health professionals. As described under the Methods section, substances prone to trafficking and misuse were given in hand and taken under direct nurse observation. However, other medications that could have been misused, such as those for sleep, depression, anxiety, and pain relief, were regularly dispensed via the boxes. In essence, any medication could be used differently than initially purported, but no such incident was reported. This finding is consistent with previous research done in the general population, showing that people on prescription medications using higher-than-prescribed dosages are doing so for the very reason the medications were typically prescribed, such as tension release and sleep (Lipari et al., 2017). Another explanation could be found in the close follow-up offered by healthcare staff to individuals identified to need counseling on and support for medication compliance. Indeed, healthcare staff could support patients struggling with medication adherence through regular counseling and by directly observing the intake. A major constraint for individuals requiring direct observation was the limitation of nurse presence to mornings during weekends and public holidays. Therefore, individuals under direct observation needed to be on a once-a-day medication, failing which the carceral system could not assign them to La Brenaz facility.
Results indicate that the medication box approach could contribute to enforcing key human rights principles. La Brenaz is an institution for sentenced individuals and aims to help them reintegrate into society. The box system was designed to empower individuals under pharmacological treatment to become autonomous in managing their medication—just as they would back in the community. The in-hand medication distribution exposes recipients to the eyes and ears of others, including prison officers. It could be stigmatizing because of the type of medication taken (e.g., antiretrovirals for HIV treatment), the frequency of distribution (e.g., perception of physical, mental “fragility,” or both if repeated distribution), or the nature of the verbal exchange with the nursing staff delivering the medication.
Officers agreed that the box system for those who were eligible saved time, a finding that was substantiated by the exploratory timing exercise done by nurses. However, to document with rigor and accuracy the resources that could be spared by the box system, a rigorous cost-effectiveness study would be needed. Meanwhile, on the basis of the exploratory timing exercise, one could easily imagine the amount of time and human resources that could be saved with the scenario of a typical patient. Such a patient would take his medication 3 times daily. After eligibility assessment by the medical team, he would switch from receiving his treatment from three daily nurse–officer encounters to a biweekly or weekly pickup of his medication from a personal box. Prison officers could dedicate freed-up time to meaningful activities, such as facilitating vocational and social skills training and support—a way to reconcile custodial and security tasks with human service works, a dilemma explored in past research (King, 2009). For nurses, the amount of time lost to repeated medication preparation, distribution rounds, and its documentation could be reallocated to one-on-one patient encounters for information, education, and counseling about the medical condition and its treatment or health promotion and prevention activities. Such nursing activities and roles have been neglected over the past decades in prison-based healthcare services and could contribute to advancing the Health Promoting Prison movement (Whitehead, 2006). At La Brenaz, the box system has, for instance, freed up time for nurses to have more patient visits and conduct health promotion activities, such as stress management sessions in a group setting, which was described in another study (Pralong et al., 2020), or individual smoking cessation counseling. They also had more time for continuing nursing education or to conduct operational research, such as this current study.
Officers agreed that the box system helped to improve the differentiation between each actor's role as the in-hand distribution approach with a nurse–officer dyad could be confusing for people receiving medication and further compound the issue of dual loyalty of health professionals working in prison, as highlighted in the literature (Pont et al., 2012). However, to optimize the system efficiency, nurses should have access to the living quarters without the escort of prison officers.
Expanding to a Monthly DistributionTwo thirds of end users would welcome a monthly distribution, which contrasted with only a quarter of prison officers. Monthly dispensing matches the dispensing practices in the community. With the view of reinforcing patient autonomy, the medical service could pilot the monthly scheme with a selected number of individuals receiving chronic nonpsychotropic treatment. Showing the feasibility of this approach with lower-risk medication and with end users who have provided informed consent and have no record of stockpiling and abuse could be the first step in reassuring the carceral authorities. Regular monitoring and sharing of experience would build the confidence of all stakeholders in such an expanded monthly dispensing scheme.
Strengths and LimitationsThe strengths of our study included the piloting of the research questions during a formative phase and the participation of both end users and prison officers, with a high participation rate of officers. However, there were limitations. First, a quarter of eligible participants left the facility before being interviewed. Still, the results from participating end users indicated common trends in satisfaction that matched those found among officers, except for the issue of monthly dispensing. Second, the use of descriptive statistics limited the breadth of our study conclusions. Adopting a mixed method with qualitative interviews of both individuals using the boxes and prison officers would have enriched and nuanced the results. Third, assessment bias could not be ruled out, nor bias toward socially desirable answers, especially as some of the authors prepared and dispensed medication and contributed to data collection.
Implications for Clinical Forensic Nursing PracticeAs an alternative or complement to in-hand medication distribution, nurses could facilitate the implementation of personal lockable medication boxes in prisons. The system could allow nurses to dedicate more time to individual visits and health promotion and prevention activities.
Several operational considerations could limit the implementation and scale-up of the medication box strategy. First, it requires a start-up investment (boxes and keys), which could be mitigated by having the prison workshops design and make robust and secure boxes. Second, this dispensing system might encounter operational challenges in larger pretrial detention facilities or jails with a high turnover of individuals. In such facilities, individuals often share a common living space and may be locked up in their cells for long periods each day. The prolonged confinement would limit their access to the living quarters, where the medication boxes would be located. Third, La Brenaz is a male-only facility, which limits the application of our in-box intervention to female detention centers. However, as there is no specific gender consideration with the in-box intervention, its implementation in female facilities should not encounter major operational barriers.
ConclusionsOverall, our study illustrated how a nurse-led initiative on the dispensing of prescribed medication, which switched from high-frequency in-hand dispensing to a lower-frequency in-box distribution in a 168-cell prison for sentenced individuals, could be feasible, acceptable, easy to use, and secure. Such an approach could contribute to the autonomy of people who experience incarceration, reduce the risk of confidentiality breaches, and allow nurses to dedicate time to more meaningful services, such as individual follow-ups and health prevention and promotion.
References Burns K. A. (2009). Commentary: The top ten reasons to limit prescription of controlled substances in prisons. Journal of the American Academy of Psychiatry and the Law Online, 37(1), 50–52. Dudeck M., Drenkhahn K., Spitzer C., Barnow S., Kopp D., Kuwert P., Dünkel F. (2011). Traumatization and mental distress in long-term prisoners in Europe. Punishment & Society, 13(4), 403–423. Elger B. S., Shaw D. M. (2017). Confidentiality in prison health care—A practical guide. In S. B. Elger, C. Rittre, & H. Stöver (Eds.) Emerging issues in prison health (pp. 183–200). Dordrecht: Springer. Fazel S., Baillargeon J. (2002). The health of prisoners. The Lancet, 377(9769), 956–965. 10.1016/S0140-6736(10)61053-7 Fazel S., Bains P., Doll H. (2006). Substance abuse and dependence in prisoners: A systematic review. Addiction, 101(2), 181–191. Fazel S., Seewald K. (2012). Severe mental illness in 33 588 prisoners worldwide: Systematic review and meta-regression analysis. The British Journal of Psychiatry, 200(5), 364–373. Herce M. E., Muyoyeta M., Topp S. M., Henostroza G., Reid S. E. (2018). Coordinating the prevention, treatment, and care continuum for HIV-associated tuberculosis in prisons: A health systems strengthening approach. Current Opinion in HIV and AIDS, 13(6), 492–500. King S. (2009). Reconciling custodial and human service work: The complex role of the prison officer. Current Issues in Criminal Justice, 21(2), 257–272. Lipari R. N., Williams M., Van Horn S. L. (2017). Why do adults misuse prescription drugs? In The CBHSQ Report. Substance Abuse and Mental Health Services Administration (US). https://www.ncbi.nlm.nih.gov/books/NBK343537/. McCall-Smith K.. (2016). United Nations standard minimum rules for the treatment of prisoners (Nelson Mandela Rules). International Legal Materials, 55(6), 1180–1205. Norman A., Parrish A. (1999). Prison nursing: Improving the quality and range of service. British Journal of Community Nursing, 4(7), 328–331. Peters D., Adam T., Alonge O., Agyepong I., Tran N. (2013). Implementation research: What it is and how to do it. BMJ, 347, f6753. Pont J., Enggist S., Stöver H., Williams B., Greifinger R., Wolff H. (2018). Prison health care governance: Guaranteeing clinical independence. American Journal of Public Health, 108(4), 472–476. 10.2105/ajph.2017.304248 Pont J., Harding T. W. (2019). Organization and management of health care in
留言 (0)