
記住我
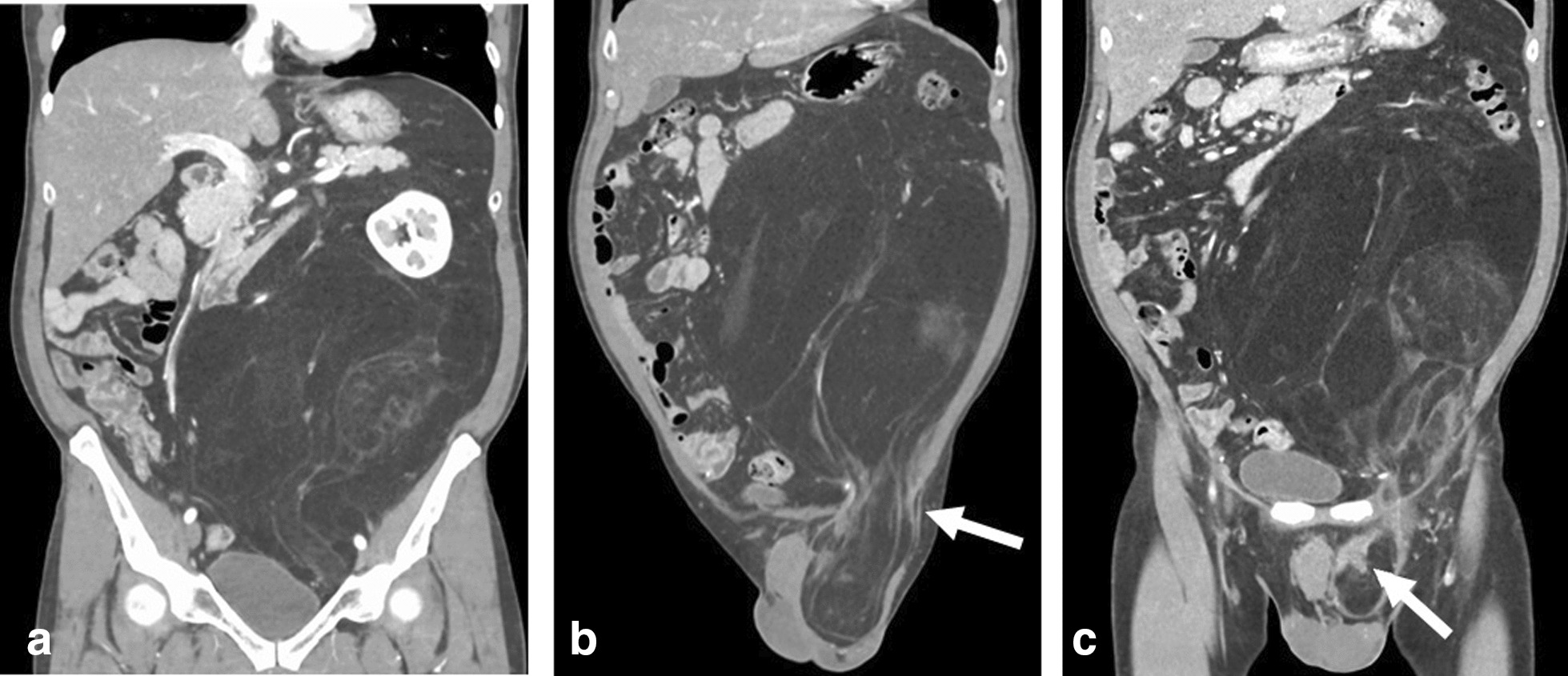
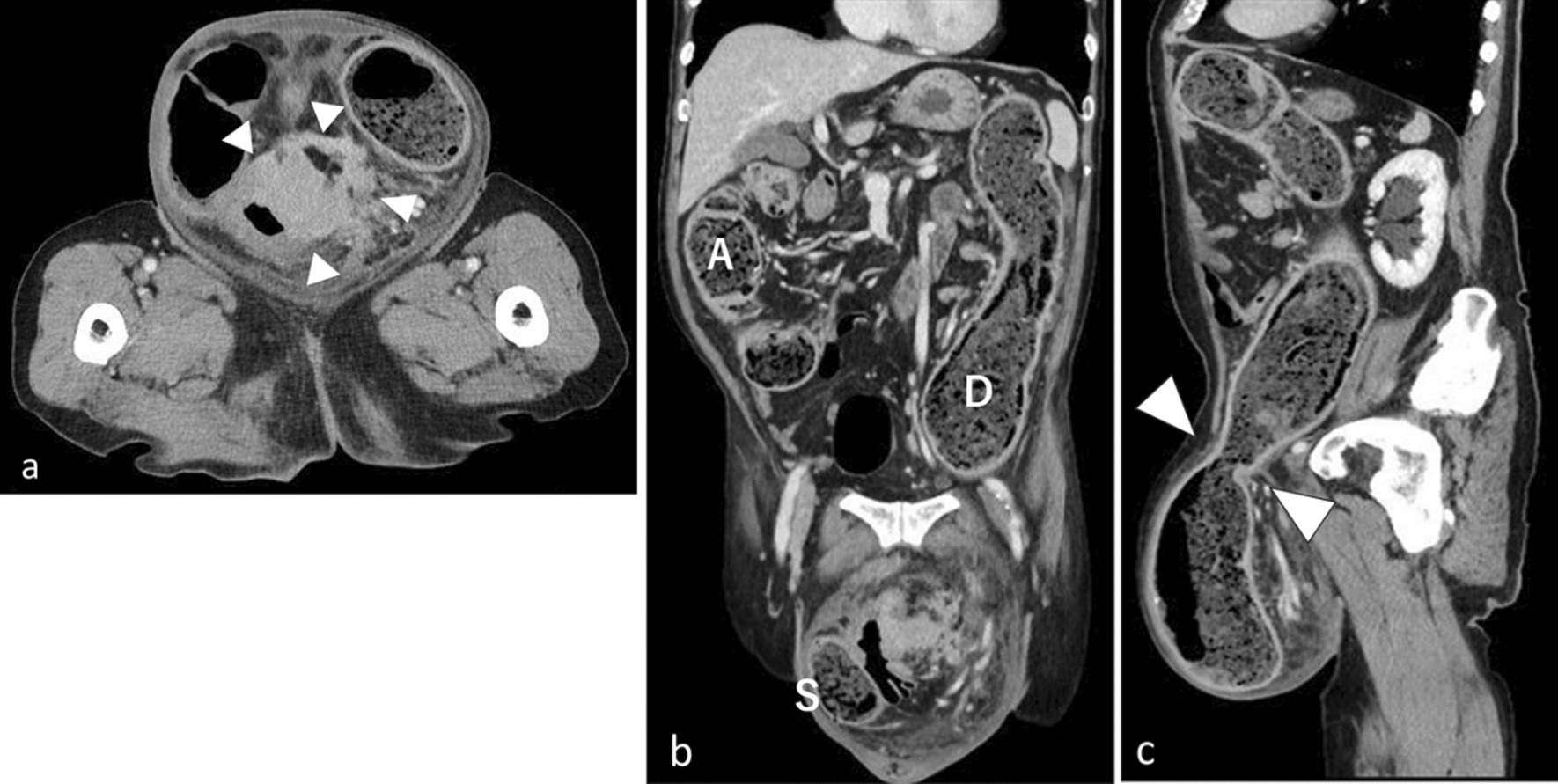






A 1-month-old male infant with a huge abdominal tumor was transferred to our hospital. The patient exhibited severe abdominal distension, an umbilical hernia, and severe edema of the lower extremities and scrotum. He required an oxygen mask because of respiratory distress. Computed tomography showed massive hepatomegaly with left adrenal gland swelling (Fig. 1A, andB). Iodine-123 metaiodobenzylguanidine (MIBG) scintigraphy demonstrated significant uptake in the liver but minimal uptake in the left adrenal gland (Fig. 1C). Laboratory data on admission showed severe liver dysfunction, as evidenced by hyperbilirubinemia (total bilirubin 10.1 mg/dL, direct bilirubin 2.5 mg/dL) and coagulopathy (PT-INR 1.67, APTT 46.70%, fibrinogen 99 mg/dL, AT-III 23.4%). Significant elevation of neuron-specific enolase (93.7 ng/mL), urine vanillylmandelic acid (499 μg/mg Cr), and urine homovanillic acid (378 μg/mg Cr) was also confirmed. Although bone marrow examination revealed negative cytology, further tests confirmed minimal residual disease, suggesting the existence of neuroblastoma cells in the bone marrow. An MYCN amplification test was negative, and chromosomal abnormalities including 11q deletion were not observed. We finally diagnosed the patient with stage 4S neuroblastoma.
Fig. 1
Enhanced computed tomography scan and iodine-123 metaiodobenzylguanidine scintigraphy on admission (A–C) and after chemotherapy (D–F). The single arrow indicates left adrenal gland swelling, and the double arrows indicate the compressed inferior vena cava by the enlarged tumorous liver. Note that the enlarged liver (B) changed to a normal size (E) after chemotherapy. D Left adrenal gland swelling disappeared and the inferior vena cava was relieved by improvement of the hepatomegaly. Iodine-123 metaiodobenzylguanidine scintigraphy on admission (C), significant uptake was seen in the liver, but minimal uptake was seen in the left adrenal gland. F After chemotherapy, the significant uptake in the liver disappeared
Although the stage 4S neuroblastoma was expected to have a high likelihood of spontaneous tumor regression, the patient’s abdominal compartment syndrome, hyperammonemia, and coagulopathy deteriorated. Seven days after the patient was transferred to our hospital, chemotherapy using carboplatin and etoposide was administered with expected acceleration of tumor regression compared with its natural course without chemotherapy, based on the Children’s Oncology Group A3961 low-/intermediate-risk course I regimen. However, because the patient developed respiratory failure secondary to abdominal compartment syndrome, which required intensive care unit admission with respiratory ventilation, a silo operation using an Alex wound retractor for the eviscerated intestine was performed to manage the severe abdominal compartment syndrome. The hepatomegaly was gradually relieved, and the silo was successfully closed 12 days postoperatively (Fig. 2). Partial disease resolution was also confirmed by computed tomography (Fig. 1D, E) and MIBG scintigraphy (Fig. 1F).
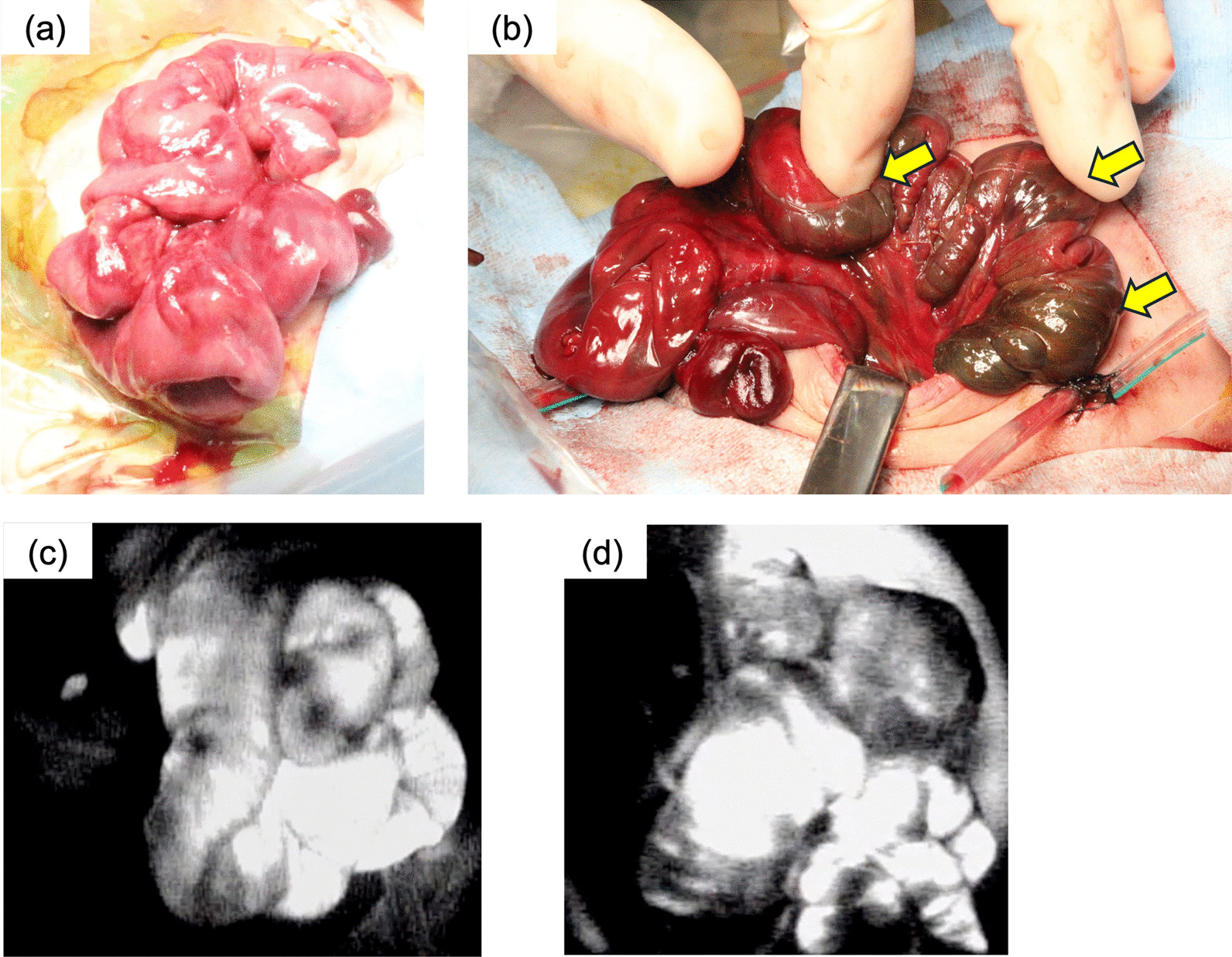
Fig. 2
Postoperative photograph of silo operation (day #12). Because of gradual relief of abdominal compartment syndrome along with liver tumor resolution, the abdominal contents in the wound retractor were successfully returned into the abdominal cavity 12 days later
Despite the decrease in tumor size, liver dysfunction continued. Fresh-frozen plasma, thrombocyte concentrates, and antithrombin III were administrated repeatedly, and continuous hemodiafiltration and plasma exchange were continued for liver support (Fig. 3).
Fig. 3
Clinical course from patient transfer to liver transplantation. Mechanical ventilation and liver support were required during this period. Blood transfusion and fractionated plasma products were administered repeatedly. Hyperbilirubinemia persisted until liver transplantation. PE plasma exchange, LDLT living-donor liver transplantation, CHDF continuous hemodiafiltration, CBDCA carboplatin, ETP etoposide, PC platelet concentrate, FFP fresh-frozen plasma, AT3 anti-thrombin III, RBC red blood cells, T-Bil total bilirubin
One month after patient transfer, the pediatric team referred the patient to the transplant team for consideration of liver transplantation. Although the levels of neuron-specific enolase, urine vanillylmandelic acid, and urine homovanillic acid as well as the imaging findings were improving, the liver failure persisted. While the patient’s father was evaluated to determine whether he could serve as a living donor, a wait-and-see approach was undertaken for the next 2 weeks to monitor for possible recovery of the patient’s liver function. Because of no sign of recovery of the patient’s liver function was observed, LDLT was performed at 93 days after birth. Because the recipient’s body weight at the time of transplantation was 4.7 kg, the lateral segment graft was reduced at the back table as well as in situ for graft accommodation (Fig. 4). Because left adrenal gland swelling as a primary lesion was already disappeared on the preoperative image study (Fig. 1D), left adrenal gland was not resected during transplant procedure. Macroscopically, the explanted liver was cholestatic and fibrotic. Hematoxylin–eosin staining and immunohistochemical microscopy showed massive dropout of hepatocytes, fibroblast replacement, and slight existence of residual neuroblastoma cells (Fig. 5A–F). The massive loss of hepatocytes was similar to that seen in fulminant hepatic failure, which explains this patient’s preoperative sustained liver failure status. Any sign of vascular complications including veno-occlusive disease were not identified clinically and microscopically.
Fig. 4
Intraoperative photograph during living-donor liver transplantation. A Native liver and B reduced lateral segment liver graft
Fig. 5
Histological findings of explanted liver. A–C Hematoxylin–eosin staining. Note the areas of small residual neuroblastoma cells (inside red line). After tumor regression, few scattered hepatocytes were present (black arrows), and the remaining areas were replaced by fibroblasts after hepatocyte dropout. Immunohistochemical staining with D synaptophysin and E neuron-specific enolase showed small residual neuroblastoma cells in vascular structures, and immunohistochemical staining with F hepatocyto paraffin 1 (HepPar-1) showed scattered hepatocytes (significant dropout of hepatocytes)
After transplantation, the patient’s liver function and coagulation status recovered quickly. Due to the unique character of spontaneous regression ability of stage 4S neuroblastoma, no chemotherapy was considered postoperatively. Because of his long pre-transplant respiratory ventilation, he required a tracheostomy for long-term respiratory rehabilitation. He was discharged from the hospital 5 months after transplantation with home intermittent respiratory support. At the time of this writing (23 months after LDLT), he was in good condition with no signs of recurrence of neuroblastoma.
留言 (0)