
記住我
The overall objective of the study is the evaluation of the clinical rationality of the one-finger meditation massage of the abdomen for treating patients with irritable bowel syndrome (IBS-C), providing a basis for clinical promotion, to have better long-term efficacy compared with drug treatment alone, to take advantage of its painlessness and higher patient compliance, and to provide an exact and effective treatment for IBS-C in Chinese medicine.
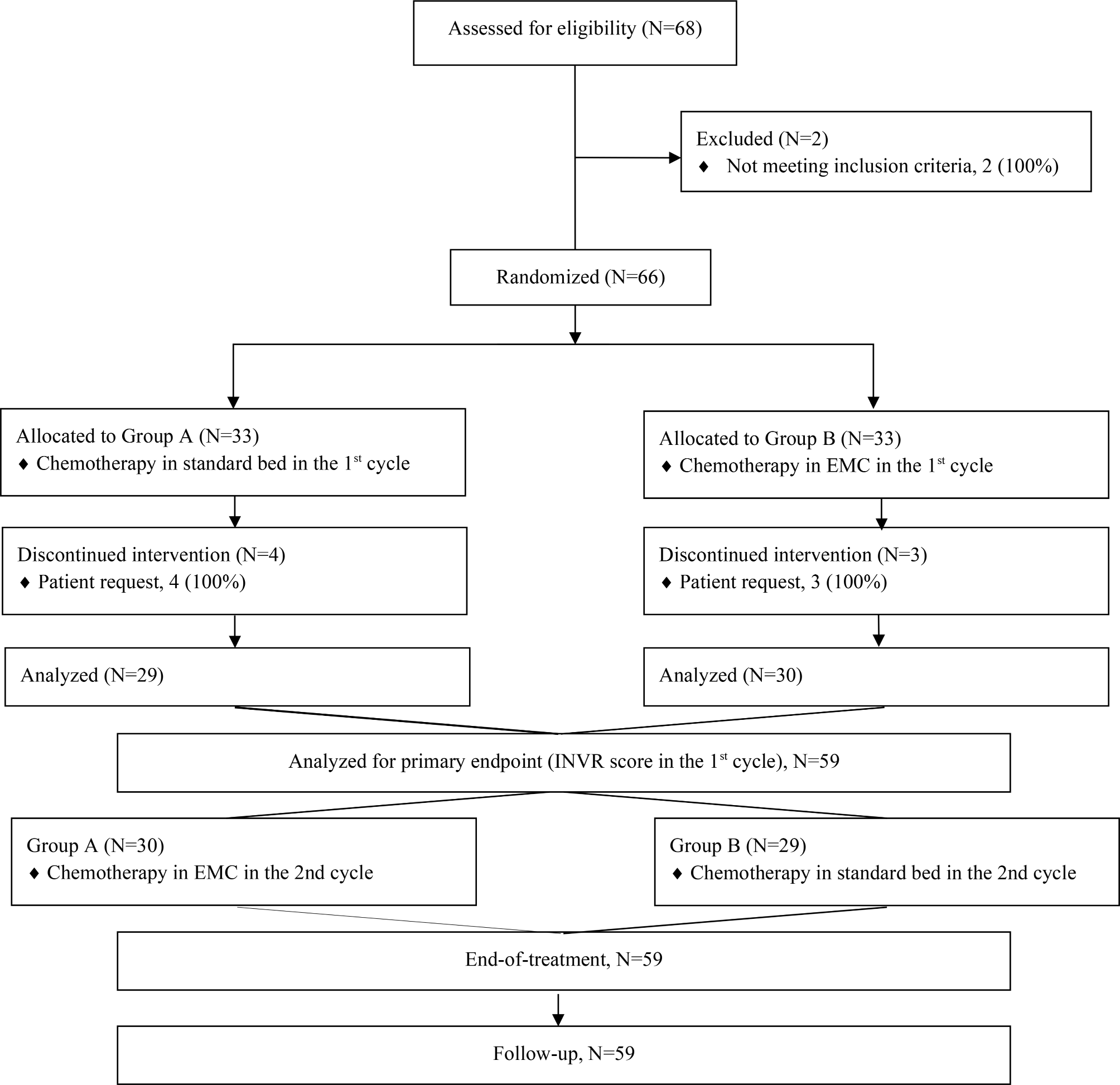
Trial designThis trial is a single-center randomized, blinded trial in which outcome assessors were blinded to compare the efficacy of one-finger meditation massage combined with probiotic therapy versus pharmacotherapy in patients with IBS-C, which were conducted at Zhejiang Hospital. In total, 66 participants with IBS-C were randomly assigned to the trial and control groups. The protocol was registered on the following website: www.chictr.org.cn (No. ChiCTR2200066417). Protocol reporting is fully compliant with the SPIRIT guidelines [55]. Figure 1 shows the flowchart of the study process. In addition, the schedule for enrolling, treating and evaluating the trial is shown in Fig. 2.
Fig. 1
Flow chart of the study process. 5-HT, 5-hydroxytryptamine, SP, substance P, IBS-SSS, IBS Severity Scale, BRSA,Bristol Rating Scale Assessment, IBS-QOL, IBS Quality of Life Questionnaire
Fig. 2
Schedule of enrolment, treatments, and assessments. O, required; 5-HT, 5-hydroxytryptamine; SP, Substance P; IBS-SSS, IBS Severity Scale (IBS-SSS) assessment; BRSA, Bristol Rating Scale Assessment; IBS-QOL, IBS Quality of Life Questionnaire
Participants, recruitment, and ethicsRecruitment of participants were from Zhejiang Hospital in two ways: recruitment posters and online recruitment. Participants were informed of the inclusion and exclusion criteria, interventions, intervention times, and other positive trial considerations during recruitment. Participants who meet the recruitment criteria will again be provided with the above information. After obtaining patient consent, patients will sign an informed consent form and be randomly assigned to a group. The Zhejiang Hospital Ethics Committee approved the study protocol (No. 2021 Pro-Audit No. 15 K).
Diagnostic criteriaRefer to the < Rome IV Diagnostic Criteria for Functional Gastrointestinal Disorders>.
IBS typically presents with recurrent episodes of abdominal pain, at least 1 day per week for the last 3 months, associated with 2 or more of the following: (1) bowel movements; (2) changes in bowel frequency; and (3) changes in stool characteristics (appearance). IBS Constipation (IBS-C): At least 25% of bowel movements are Bristol 1–2, and less than 25% of bowel movements are Bristol 6–7.
Inclusion criteriaSubjects with all of the following conditions were included: (1) meet the Western medicine diagnostic criteria of IBS-C; (2) aged between 20 and 80 years; (3) can adhere to the treatment as planned and can receive follow-up; (4) patients are conscious and can actively cooperate with the treatment, examination and complete the correct description of the assessment items; and (5) patients themselves or their relatives sign the informed consent.
Exclusion criteriaSubjects with one of the following conditions were excluded: (1) those not meeting the above diagnostic and inclusion criteria; (2) pregnant or lactating patients; (3) patients with serious life-threatening primary diseases, including cardiovascular, cerebrovascular, hepatic, renal, hematopoietic and psychiatric diseases; and (4) those who receive other relevant treatments that may affect the observation of effect indicators in this study.
Randomization and allocation concealmentAn independent statistician who is not involved in the study will generate the randomization group: the numbers were randomly divided into two Groups A and B at a ratio of 1:1, i.e., A (Test group: Massage with the probiotic group) and B (Control group: probiotic group), using SPSS 19.0 software before the formal trial. The random sequence of the generated numbers and the grouping information were kept by the person in charge and kept confidential. Opaque brown envelopes were made according to the number of included cases, and the envelopes were numbered sequentially according to the order of numbers on the surface of the envelopes. The envelopes will contain the grouping information corresponding to the random sequence of numbers on the surface of the envelopes, such as 1(A) and 2(B). After signing the informed consent form and completing the basic information form, the envelopes were opened strictly in the order of the numbers on the envelopes, and patients were allocated to groups (trial or control) in accordance with the protocol in the envelopes.
BlindingThis is a participant-rater-blinded study, meaning that participants do not know the group to which they belong. Participants have a 50% chance of being assigned to the test and control groups: massage with the probiotic group and probiotic group. The patient’s group allocation is also unknown to the follow-up assessors. Although the massage therapist will not be blinded to his or her treatment assignments, the massage therapist will not be part of the outcome assessment or data analysis.
InterventionTest group (massage with probiotic group)The acupuncture points and areas are as follows: Zhongwan (RN12), Tianshu (ST25), Guanyuan (RN4), Qi Hai (RN6), Pishu (BL20), Shenshu (BL23), Dachangshu (BL25), Mingmen (DU4), Zusanli (ST36), Zhi Gou (SJ36) and abdomen. The locations of all selected acupoints are shown in Table 1. Operations: (1) Using the one-finger meditation massage method, the patient is in a supine position, and the operator uses the one-finger meditation massage method to push ST25, RN4, RN6, and RN12 for 2 min each; the one-finger meditation massage method requires concentration, sinking shoulder, dropping elbow, hanging wrist, palm deficiency, finger solid, tight pushing, and slow moving. The frequency of swinging is approximately 120–160 times/min; (2) Two minutes of clockwise abdominal massage; (3) Press and knead SJ36 and ST36 points for 1 min each; (4) The patient is in a prone position and rubs the lumbar back, BL23, DU4, BL20, and BL25 for approximately 2 min to penetrate the heat. The manipulation should be even, gentle, persistent, and powerful to achieve deep penetration; (5) Course of treatment: 10 days once, 3 times as a course of treatment, three consecutive courses of treatment (i.e., three months). The patient were given Bifidobacterium trifolium capsules (Shanghai Xinyi Pharmaceutical Co., Ltd., State Drug Administration S0950032) 630 mg/d, 3 times/d, 30 min after the meal for three months.
Table 1 Location of acupoints for treating IBS-C Control group (probiotic group)The patients were given Bifidobacterium trifolium capsules (Shanghai Xinyi Pharmaceutical Co., Ltd., State Drug Administration S0950032) 630 mg/d, 3 times/d, 30 min after the meal; the course of treatment were three months. Patients were advised to cultivate good lifestyle habits, avoid dairy products, soybeans, and other gas-producing foods and encouraged to consume moderate amounts of high-fiber foods.
Outcome measuresPrimary outcome5-HT and SP concentrationSerum 5-HT and SP concentrations in patients were determined before and after treatment using an enzyme-linked immunosorbent assay (ELISA). The level of 5-HT is closely related to the presence of diarrhea or constipation in irritable bowel syndrome, as well as SP [55, 56]. We will compare the efficacy of the two groups by ELISA of serum 5-HT and SP in patients before and after treatment.
IBS Severity Scale (IBS-SSS) assessmentOutcomes included the level of abdominal pain, frequency of abdominal pain, level of bloating, bowel satisfaction and effects on life. (1) Abdominal pain severity, frequency of pain in the abdomen, abdominal distension degree, defecation satisfaction, and effects on life were included. (2) Abdominal pain frequency score: abdominal pain frequency score = actual abdominal pain days/14 × 100. (3) IBS-SSS scale total score: IBS-SSS scale total score = abdominal pain severity score + abdominal pain frequency score. IBS-SSS scale total score = abdominal pain score + abdominal pain frequency score + abdominal distension score + bowel satisfaction score + impact on life satisfaction score + impact on life score.
Secondary outcomeBristol rating scale assessmentUsed to assess stool properties under visual observation during bowel preparation. 1 point: scattered hard masses, resembling nuts; 2 points: similar to salami but lumpy; 3 points: similar to salami but with superficial cracks; 4 points: similar to salami or snake, smooth and supple; 5 points: supple masses, with clear edges; 6 points: fluffy material, with indistinct edges, paste-like stool; 7 points: watery, without solids.
IBS Quality of Life Questionnaire (IBS-QOL scale)The total score of the scale and the score of each dimension of the scale were calculated separately. The scale consists of 8 dimensions: poor mood, behavioral disorders, self-image, health concerns, avoidance of food, social functioning, sexual behavior and expansion of relationships. The total scale score and each dimension score were converted into standard scores according to the following formula. Standard score = (actual score sum of each item - theoretical minimum score/theoretical score range) ×100%.
Evaluation of the evidence efficacyIn accordance with the Guiding Principles for Clinical Research on New Chinese Medicines (Trial), the efficacy index was calculated using the nimodipine method: efficacy index = [(pretreatment score - posttreatment score)/pretreatment score] × 100%, divided into four levels: clinically cured, effective, and ineffective. (1) Clinically cured: disappearance or almost disappearance of major symptoms and signs, effectiveness ≥ 95%; (2) effective: a significant improvement in the main symptoms and signs, 70% ≤ effectiveness < 95%; (3) a significant improvement in the main symptoms and signs, 30% ≤ effectiveness < 70%; (4) ineffective: no significant improvement in the main symptoms and signs, 30% ≤ effectiveness < 95%;
Follow-up observation: (1) Follow-up and observation of all healed and effective cases; (2) Follow-up and re-evaluation every 3 months for a total of 2 times; (3) Follow-up can be done by telephone or letting the patient come to the hospital for re-evaluation or visiting the hospital if necessary; (4) Symptom re-evaluation with a score ≥ 1 level is determined as a relapse, and the follow-up will be stopped next time.
Statistical methodsSample sizeThe test group sample size (massage with the probiotics group) and the control group (probiotics group) were randomly grouped in a 1:1 ratio, and the sample size was determined according to the bilateral hypothesis test, setting the test criterion as a = 0.05 (bilateral) and test efficacy as β = 0.20. The efficiency of the test group in the preexperimental observation is 90, and the efficiency of the control group is 60. The required sample was calculated to be approximately 60 cases, with an increase of 10% of cases taken off, and the actual sample size is approximately 66 cases; that is, 33 cases in the test group and 33 cases in the control group are selected.
Statistical analysisTwo independent researchers will record all experimental data on CRF forms and enter them into the computer. Data will counted by statisticians using SPSS 19.0 statistical software. The mean ± standard deviation (M ± SD) will used for measurement data, paired sample tests will be used for before-and-after control within groups, independent sample tests will used for comparisons between groups, and chi-square tests will be used for efficacy grading. p < 0.05 is considered a statistically significant difference.
留言 (0)