No previous reports described spontaneously vanishing GISTs, and this was an extremely rare case. The tumor, which grossly disappeared intraoperatively, was resected without excess or deficiency by LECS, leading to an accurate diagnosis and optimal postoperative treatment.
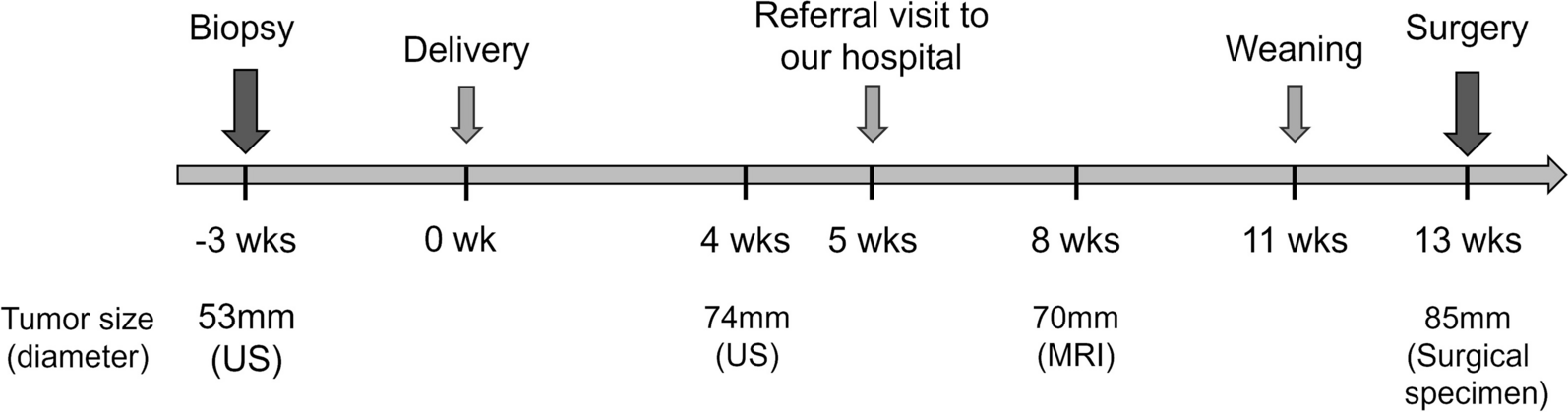
The terms spontaneous remission and spontaneous regression (SR) exist in the field of oncology [3]. SR of a malignant tumor is defined as the disappearance of part of the tumor or the entire tumor despite no treatment or inadequate curative treatment [4]. Several reports describe SR of neuroblastomas, renal cell carcinomas, malignant melanomas, and lymphomas, although the SR of a GIST has not been reported [5]. In this case we experienced, there has been no definitive conclusion as to whether the terms “spontaneous remission” or “regression” are appropriate to apply. The indisputable fact is that the tumor, which was over 50 mm in size at the time of initial diagnosis, appeared as a 20-mm tumor at the time of removal without treatment. The possible progression of the tumor if left untreated cannot be determined. However, the crucial point is that the tumor morphologically changed and was no longer visible to the naked eye. Because of this phenomenon, designing a treatment plan was difficult.
Endoscopy, EUS, and CT are commonly used to diagnose GISTs [6]. In our case, preoperative imaging with endoscopy, EUS, and CT revealed typical findings of gastric GIST with a large tumor size. Thus, EUS-FNA was not performed, and surgery was decided as the first-line treatment. According to the Japanese guidelines for GIST treatment, surgery is the first choice for submucosal tumors larger than 5 cm, and a definitive diagnosis by preoperative biopsy is not always necessary [7].
The objective of surgery for localized GISTs is to achieve R0 resection to the greatest extent possible. Lymph node dissection is not recommended, except when lymph node metastasis is clinically suspected. Therefore, wedge or segmental resection with preservation of organ function to maintain quality of life is recommended [8]. Previous studies demonstrated that laparoscopic resection is feasible and safe for gastric GISTs and is less invasive than traditional open surgery, and laparoscopic and open surgeries for GISTs have similar oncologic outcomes [9].
LECS is the standard surgical procedure for GIST treatment because it is minimally invasive and adequate resection can be achieved [2, 10, 11]. Laparoscopic surgeries for GISTs larger than 5 cm have better short-term outcomes in terms of operating time, blood loss, perioperative complications, and hospital stays, and comparable long-term outcomes in terms of disease-free survival and overall survival [12]. At our institution, LECS is the first-line treatment for the intraluminal growth type of GISTs, regardless of size.
The presumed causes of tumor morphology changes, as in the present case, include hemorrhage, infection, necrosis, penetration, and perforation. Several reports described such conditions in patients with GISTs, but all of these conditions caused acute abdominal symptoms requiring emergency treatment[13, 14]. Furthermore, none of these conditions were associated with changes in tumor morphology. In our case, the patient showed no clinical signs of abdominal pain, fever, hematemesis, hematemesis, hemorrhage, or progressive anemia during the one month between the time of endoscopy, EUS, CT, and surgery. The pathology also showed no secondary findings suggestive of hemorrhage, infection, necrosis, or perforation.
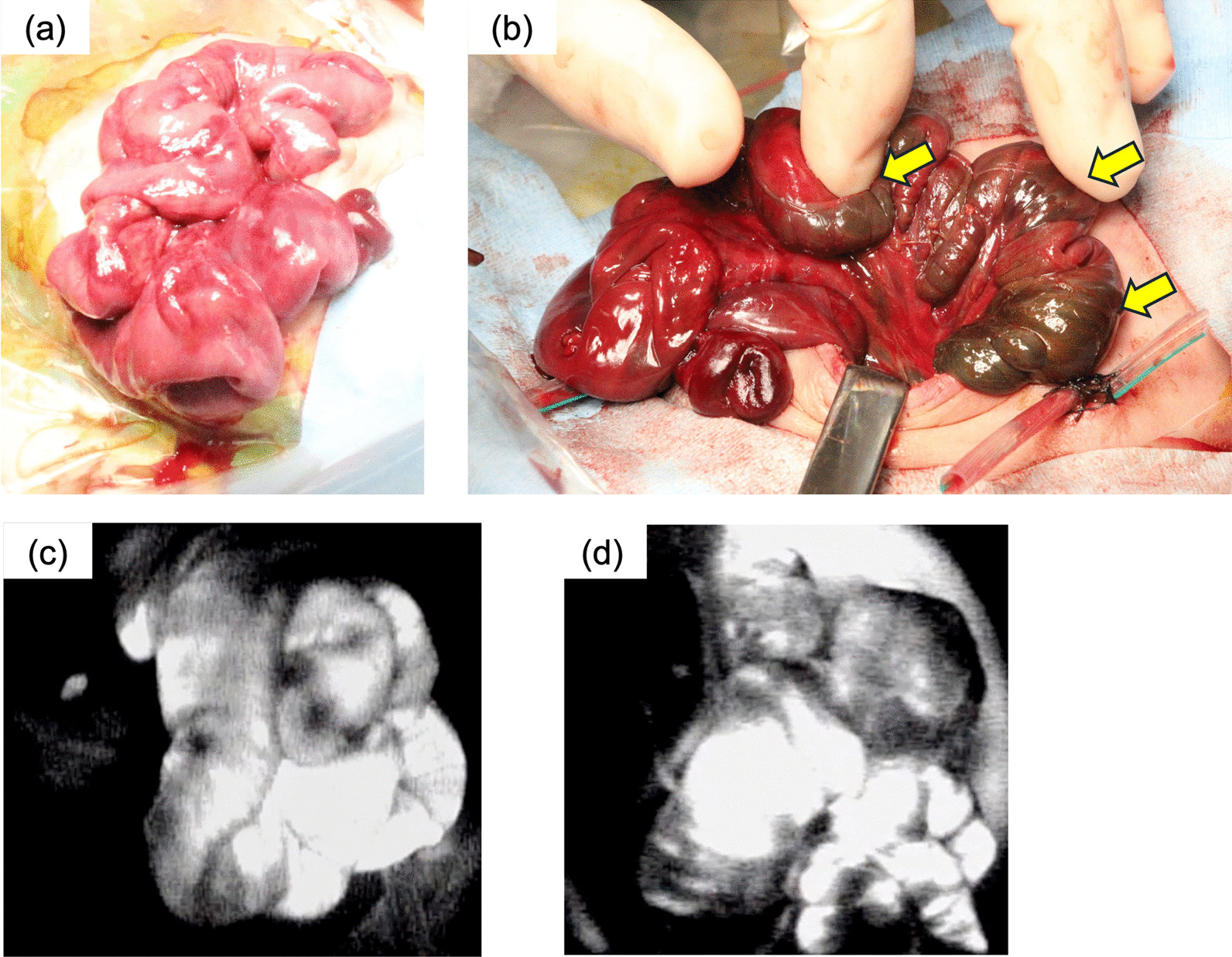
Surprisingly, no obvious mass could be observed during the intraoperative endoscopy. The surgical team had to make a very difficult decision as to whether to resect or to stop the surgery and follow up. The decision about what area to resect was also challenging. Considering the possibility of a tumor remnant, the decision was reached to resect the tumor scar. Although no previous reports describe the extent of resection, we performed full-thickness resection with a margin of 2–3 cm from the probable tumor scar by LECS. As a result, the histopathological diagnosis of GIST was confirmed, the resection margin distance was not excessive, and the best surgical treatment was provided. Even after attentive observation of the resected specimen, it was incapable of noting the presence of the tumor from the mucosal surface grossly, and a 22 mm mass was identified histologically in the gastric submucosa to the muscularis propia. A retrospective review suggested that the tumor could not have been identified by conventional endoscopy at the time the LECS was performed, although its presence could have been confirmed by EUS. Additionally, the EUS findings would have been very useful in deciding to resect and determining the extent of the resection. Performing EUS routinely during LECS is not practical due to the need for special equipment and scopes. Nonetheless, in situations similar to this case during LECS, EUS can be a valuable strategy.







留言 (0)